


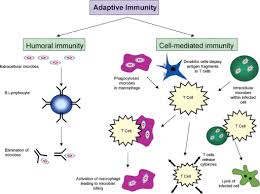
Adaptive immune response
Week 2 Discussion:1
An allergy can be defined as an adaptive immune response directed against non-infectious environmental substances. Allergens are antigens that cause allergic responses (McCance, Huether 2014). In this case, Janet is experiencing different symptoms accompanied with different diagnosis that indicate an underlying allergy response. She has itchy eyes, nasal congestion, and watery nasal discharge. She also states that she has a tickling cough along with episodes of sneezing. Janet also gets frequent “colds” every spring and fall. Although many of these symptoms overlap when diagnosing, Janet is experiencing allergic rhinitis, acute sinusitis, and allergic conjunctivitis.
Allergic rhinitis is characterized by having symptoms of sneezing, nasal pruritus, airflow obstruction, and mostly clear nasal discharge. Not only was she experiencing these symptoms mentioned above but also presented with medium polyps on each side which is linked to allergic rhinitis (Wheatley & Togias, 2015). Upon physical examination, she also experienced tenderness over maxillary sinuses indicating acute sinusitis. Clinically, sinusitis is classified by nasal congestion, rhinorrhea, facial pain, and sneezing (Aring & Chan, 2016). Finally, she is also presenting redness on sclera and slightly swollen exhibiting allergic conjunctivitis.
Although there is a lot of information supporting allergies, there are a few questions that could be asked upon examination.
1. How long have you been experiencing these symptoms?
2. Have you ever had allergy testing?
3. Do you have any pets?
4. Have you ever had a history of asthma?
5. Are you exposed to smoke, mold, dust?
Rhinitis is the inflammation of the nasal mucosa. When a person is exposed to an allergen (pollen, molds, smoke, dust, etc.) it causes in an infiltration of mast cells, T cells, B cells, macrophages, and eosinophils within the nasal lining. The T cells release cytokines that promote the production of IgE. IgE later triggers the release of histamine and leukotrienes that cause vasodilation, increased capillary permeability, itching, runny nose, mucous secretion and smooth muscle contraction. The mediators and cytokines that have been released during this first exposure to the allergen then prompt a further cellular inflammatory response (late-phase inflammatory response) which occurs over the following 4-8 hours leading to nasal congestion and recurrent symptoms (Small & Kim, 2011).
Hypersensitivities are over-exaggerated immune responses and can be broken down into different classified reactions: allergy, autoimmunity, and alloimmunity. Hypersensitivity Type I (IgE-mediated) reactions are mediated through the binding of IgE to Fc receptors on mast cells. This causes mast cell degranulation and in turn causes the release of histamine and other inflammatory substances. Type II (tissue-specific) occurs when antibody binds to tissue-specific antigens. It is mediated by IgM or IgG targeting membrane-associated antigens. This hypersensitivity can be caused by five possible mechanisms: complement-mediated lysis; opsonization and phagocytosis; neutrophil-mediated tissues damage; antibody- dependent, cell mediated cytotoxicity; and modulation of cellular function. Type III (immune complex-mediated) reactions are caused by the formation of immune complexes that are deposited in target issues, where they activate the complement cascade, producing chemotactic fragments that attract neutrophils into the inflammatory site. Neutrophils then release lysosomal enzymes that result in tissue damage. Type IV (cell-mediated) has a cell-mediated response rather than antibodies unlike other hypersensitivity reactions. These reactions can involve either cytotoxic T lymphocytes (Tc cells) or Th1 cells (McCance, Huether 2014). All of Janet’s signs and symptoms that she presented with are indicative of type 1 hypersensitivity.
References
Aring, A., & Chan, M. (2016). Current Concepts in Adult Acute Rhinosinusitis. Retrieved from https://www.aafp.org/afp/2016/0715/p97.pdf
McCance, K.L, Huether, M. (2014). Pathophysiology: The biologic basis for disease in adults and children (7th Ed.). St. Louis, Missouri. Elsevier Mosby.
Small, P., & Kim, H. (2011). Allergic rhinitis. Allergy, asthma, and clinical immunology: official journal of the Canadian Society of Allergy and Clinical Immunology, 7 Suppl 1(Suppl 1), S3. doi:10.1186/1710-1492-7-S1-S3
Wheatley, L. M., & Togias, A. (2015). Clinical practice. Allergic rhinitis. The New England journal of medicine, 372(5), 456-63.
Week 2 responses 2
Based on her symptoms, Atopic dermatitis would be consistent with Janet’s flaky, erythematous rash on her arms. Up to 80% of people with atopic dermatitis have a personal or family history of asthma, allergic rhinitis, or food allergy. The cause of this dermatitis “involves an interplay of genetic predisposition, altered skin barrier function associated with filaggrin gene missense mutations (proteins that bind keratin in the epidermis), reduced ceramide (a stratum corneum lipid) levels, altered innate immunity, and altered immune responses to allergens, irritants, and microbes” (McCann & Huether, 2014, p. 1654). Memory T cells express cutaneous lymphocyte antigen, which leads to lymphocytes traveling to the skin. When mast cells are activated, eosinophils, macrophages and expression of IgE contribute to the inflammatory process (McCann & Huether, 2014, p. 1654).
Since Janet has a history of getting frequent colds, that would be another differential diagnosis I would consider. Signs and symptoms would include a runny or stuffy nose, in which she complains of watery nasal discharge. A sore throat, which could account for her pharynx being slightly erythematous, as well as cough, congestion, and sneezing, in which she complains of all. A cold could also cause slight body aches, mild headache, and a low-grade fever and malaise. Her temperature was 98.8, but she has not complained of any head or body aches.
My third and primary diagnosis is allergic rhinitis which is seasonal or perennial itching, sneezing, rhinorrhea, nasal congestion, and sometimes conjunctivitis, caused by exposure to pollens or other allergens. Diagnosis is by history and occasionally skin testing. First-line treatment is with a nasal corticosteroid (with or without an oral or a nasal antihistamine) or with an oral antihistamine plus an oral decongestant.
To further evaluate her and to make a more definitive diagnosis, there are several other questions I’d like to ask Janet. These would be:
• Do you have a family history of allergic reactions, seasonal allergies, etc.? This question would help confirm my primary diagnosis of allergic rhinitis, as research shows that if one or both parents has a history of allergies, the child could have a 40-80% chance of also being susceptible (Rote & McCance, 2014).
• Are you exposed to animals and pet dander, dusty environments, cigarette smoke, etc.? These are fairly common triggers of allergic rhinitis, so establishing if there is exposure could help determine the causes of Janet’s symptoms, as well as help her avoid them and decrease her incidence of flare-ups.
• In regard to the skin symptoms, is the rash localized to the flexor surface of the elbow, and does the rash come and go or worsen with exposure to certain environmental factors? Or is the rash on other parts of the body as well, such as the scalp, and flares up regardless of exposure? These questions will assist in differentiating eczema versus psoriasis, as eczema, or atopic dermatitis, is often brought on by exposure, whereas psoriasis is an autoimmune response.
• Have the symptoms of both the allergic rhinitis and skin rash recently started, or have these symptoms occurred throughout your lifetime?
• Is there history of immediate family having skin issues similar to your symptoms? This can also help differentiate psoriasis, as it is often genetically hereditary (McCann & Huether, 2014).
The pathophysiological process of allergic rhinitis is a Type I hypersensitivity reaction. The tissues most commonly affected by histamine effects are the ones containing large amounts of mast cells, which include the skin, the gastrointestinal tract, and the respiratory tract. The allergens cause the inflammation of the mucous membranes in the nose, sinuses, sclera, and pharynx, and also cause increased mucus production and itching. Janet is experiencing textbook symptoms of allergic rhinitis and should be started on a daily antihistamine, such as cetirizine or loraditine, among others.
There are four types of hypersensitivity reactions.
- Type I – mediated by IgE and the tissue mast cells.
- Type I most often occurs in response to environmental antigens
- Type II – Generally when the immune response targets a certain cell or tissue. Type II occurs when antibody binds to tissue-specific antigens.
- Type III – Causes by antigen-antibody complexes that are made in circulation and dropped off later in vessel walls or tissues. The antibody binds to a soluble antigen, then deposits it into a tissue, but are not organ-specific.
- Type IV – This type is the only one mediated by T lymphocytes and do not involve antibody. Tissue breakdown is usually caused by either Tc cell toxins killing the cell or the release of enzymes and toxic reactive oxygen species (Rote & McCance, 2014).
Janet is experiencing a type I hypersensitivity reaction. Some type I allergic responses can be controlled by blocking histamine receptors with antihistamines, however the primary mechanism of control is the autonomic nervous system. This system includes biochemical mediators such as epinephrine and acetylcholine, which like the mediators of the inflammatory response, have profound effects on cells. They bind to appropriate receptors on mast cells and the target cells of inflammation thereby controlling the release of inflammatory mediators from mast cells and the degree to which target cells respond to inflammatory mediators (McCann & Huether, 2014, p. 272).
References
McCann, S. A., & Huether, S. E. (2014). Structure, function, and disorders of the integument. In K. L. McCance, S. E. Huether, V. L. Brashers, & N. S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (7th ed., pp. 1616-1652). St. Louis, MO: Elsevier Mosby.
Rote, N. S., & McCance, K. L. (2014). Alterations in immunity and inflammation. In K. L. McCance, S. E. Huether, V. L. Brashers, & N. S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (7th ed., pp. 262-297). St. Louis, MO: Elsevier Mosby.
We can write this or a similar paper for you! Simply fill the order form!
