


Bloom Taxonomy
Bloom Taxonomy
Order Instructions:
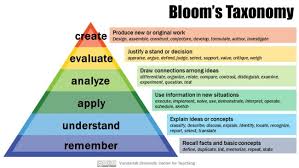
Study Bloom’s Taxonomy; apply the principles of it to provider-patient communication during a crisis. Compare best practices of communicating with patients in a crisis to Bloom’s Taxonomy in terms of patient needs.
Requirements:
1. Five pages maximum. I will not read more.
a. Reference List and Title pages do not count toward the 5 page maximum
2. Times New Roman, 12 point font, 1” margins all around, double space
3. Resources required:
a. Five required resources cited must be beyond the textbook. (Limit: 7)
i. One of the 5 must be an interview that you personally conduct (in person,
phone, or email). No more than one interview.
ii. One or more of the 5 must be from a professional journal or magazine
iii. The other 3 sources cited may be from any combination of the following: professional journal, magazine, newspaper, book (not your textbook)
b. You may cite from your textbook; any textbook citations will not be counted
toward your 5 required
c. Citation: APA format. See https://owl.english.purdue.edu/owl/resource/560/01/
i. Use In-text citation (no footnotes or endnotes)
ii. Reference List (does not count as part of your 5 page maximum)
SAMPLE ANSWER
Bloom Taxonomy
The present health care system dictates that delivery processes integrate various interfaces and patient handoff amid myriad health care practitioners with different levels of educational and professional background. During the timeframe of a four-day hospital stay, a patient might come into contact with 50 different personnel, including doctors, clinicians, technicians, and others. Dynamic clinical practice thus includes many cases where essential information should be correctly communicated. Team cooperation is critical. When health care specialists are not communicating productively, the safety of a patient is at risk for various reasons: insufficient essential information, mix-up of information, ambiguous orders over the telephone, and ignored adjustments in status. Poor communication leads up to circumstances where medical errors can take place. These mistakes have the capacity to amount in severe injury or surprise patient demise. Medical flaws, particularly those caused by lack of communication, are widespread challenge in today’s health care organizations. Conventional medical education stresses the significance of a practice that is free from errors, using severe peer pressure to accomplish perfection at the time of diagnosis and treatment. Mistakes are thereby conceived normatively as a harbinger of failure. This situation generates an atmosphere that prohibits the fair, honest assessment of errors needed if organizational learning is to occur. It is significant to stress that nurturing a team cooperation environment may have problems to solve: extra time, conceived loss of independence, lack of confidence, conflicting ideas, amid others. However, many health care personnel are aware of the poor communication and teamwork, as a consequence of a culture of truncated outcomes that has bloomed in many health care situations (Helmreich and Schaefer, 2009).
According to Irwin, McClelland and Love (2006)communication is the core factor in medical care. In essence communication between physicians and patients is amassing a growing amount of attention with the health care in the U.S. In the last few years descriptive and investigational research has attempted to focus on the communication activities during medical consultations. Nevertheless, the knowledge obtained from these endeavors is restricted. This is likely because amid inter-personal relationships, the physician-patient collaboration is one of the most sophisticated ones. While advanced technologies could be utilized for medical diagnosis and treatments, interpersonal communication is the key apparatus by which the doctor and the patient trade information (Stiles & Putman, 2007). Particular factors of doctor-patient communication appear to have considerable effect on patients’ attitudes and safety, for instance, contentment with care, positive response to treatment, recall and having knowledge about medical information, dealing with disease, qualify of life, and even condition of health. Cooperation and communication are particularly essential in the case of a chronic disease, such as a cancer (Fallowfield, Maguire & Baum, 2002). Today, specialists of communication have progressively been focusing on psychological features of cancer. Creating a proper inter-personal cooperation between physicians and patients can be interpreted as a significant function of communication. Furthermore, proper inter-personal relationship forms the basis for optimum medical care. On the other hand, the significance of a good physician-patient relationship relies on its therapeutic qualities. Another key function of medical communication is supporting the exchange of information between the physician and the patient.
Information can be regarded as a resource brought into the verbal exchange between the two parties. From a medical standpoint, physicians need information to determine the correct diagnosis and treatment strategy. From the patient’s standpoint, two needs have to be accomplished when meeting with the physician: the need to know and understand and the need to experience a sense of being known and understood. To be capable of achieving doctor’s and patient’s needs, both alternate between information-transmission and information- hunting. Patients have to provide details about their symptoms, physicians’ needs to considerably look out relevant information. At times patients may be inclined to ask for as much information as possible, doctors appear to know patients needs for information. For instance, where cancer is involved, the desire for information is most great. A great number of cancer patients’ discontentment with transmission of information emanates from concordance between views of patients and physicians. When relaying information to cancer patients about their disease (good or bad), doctors might explain medical information more empirically while patients explain it as a matter of individual relevance. As a consequence, the doctor might experience a satisfying sense that he has offered right and relevant information. The patient conversely might feel he has discovered nothing satisfying. Recent research indicates that about 45 percent of cancer patients have reported that no information has been provided relating to dealing with their disease (Fallowfield et al., 2002), however most patients wanted such information. Doctors must thereby first motivate their clients to exchange their key worries without interruption (Ben-Sira, 2008).
Psychological privacy involves a patient’s capacity to be in charge of active and cognitive inputs and outputs, to think and formulate behaviors, values to establish with whom to share information. Nevertheless, asking delicate questions and divulging confidential information is inevitable if the physician desires to find an effective diagnosis and treatment. The degree to which doctors communicate in a more dynamic, high-regulation style, could be conceived by patients as abuse of their psychological privacy. Physicians’ attitudes during patient examinations are regulated by societal values. It seems that at the time of medical interactions limited privacy is needed. Constant eye contact, for instance, could be viewed by the patient as excessively intimate for the relationship. Conversely physical privacy can be regarded as a relevant aspect of non-verbal communication and can lead to improved quality of the inter-personal interactions between physicians and patients (Stiles and Putman, 2007). Other result gauges utilized to examine the quality of the physician-patient interaction are patients’ recall and understanding information. As it stands, most patients fail to recall or comprehend what the physician has told them. Patient compliance is also a broadly utilized result variable and is regarded a measure of the productivity of provider-patient communication. Doctor-patient interaction might have significant outcomes for patient’s health outcomes, thus this relationship can be viewed as a type of social support. Lack of information appears to play a vital function in psychological challenge that can come up during the diagnosis and treatment (Irwin, McClelland & Love, 2006).
References
Ben-Sira.Z. (2008). “Affective and instrumental components in the physician patient relationship: an additional dimension of interaction theory.” Journal of Health Sociological Behavior, 170-185.
Fallowfield. L. J., Hall A., Maguire. G. P. and Baum. M. (2002).“Psychological outcomes of different treatment policies in women with early breast cancer outside a clinical trial.” British Medical Journal, 301- 575.
Helmreich. R.L & Schaefer H.G. (2009). Team performance in the operating room and Human error in medicine. Hillside, NJ: Lawrence Erlbaum.
Irwin W. G., McClelland R. and Love.A. H. G. (2006). “Communication skills training for medical students: an integrated approach.” Medical Education, 387-390.
Stiles. W. B. and Putnam. S. M. (2007).Analysis of verbal and non-verbal behavior in doctor- patient encounters: In Communicating with Medical Patients. Newbury Park, CA: Sage Publications.
Appendix: Interview
I chose to interview a personal acquaintance of mine who happens to be a screenplay enthusiast. I think it is a fantastic occupation path since it balances creativity and professional writing.
- What are you pursing as an undergraduate student?
I am studying Journalism.
- How will your undergraduate studies influence your future career?
I am on track to work in the corporate world, probably as an editor
- When did you first develop interest in screenplay writing?
I like to think when you first write a screen-play and gets positive comments from people who have been in the production scene for some time, you get interest in that moment. It had never occurred to me that this was something I’d be doing as pastime thing.
- How much experience with screenplay writing do you have?
None as a matter of fact, but I have always been involved with creative writing on the side (for instance, poems and flash stories).
- What are some of your objectives for the future?
Finishing my undergraduate, find a job, get a job, and see what fate throws my way. I have come to discover in life that whatever you make plans, the big guy above somehow has a totally different idea.
- Would say that screenwriting you will be engaged in as a side project rather than a full time career?
I don’t want to find myself restricting myself at all. My undergraduate will put me up in the corporate world, but this might as well turn into an amazing gig in the future.
We can write this or a similar paper for you! Simply fill the order form!
