


Chronic Obstructive Pulmonary Disease
Order Instructions:
Dear Admin,
Your task is submit your final Project Report. The completed report should be properly presented with a title page, table of contents, and references where necessary.
For this project, you will have studied the Philips Electronics model of business excellence through speed and teamwork (BEST). You will find this model described Project Study in the attachment.
You will also have read the following brief but important journal article: TQM and business excellence: is there really a conflict?
Also, read project proposal, project outline, and project case study all of them in the attachment before you start to write the project.
Your task is:
1.To assess the BEST model, with particular reference to the importance of teamwork in a company like Philips Electronics.
2.To evaluate the model against Adebanjo’s proposition that ‘business excellence and quality can and need to complement each other to provide organisations with the operational and business success they aspire to and which is necessary for survival in today’s market.’
3.To show how BEST tools and competencies could be applied to the pursuit of business excellence in your company or another company you think could benefit from using the model.
Also,
1) The answer must raise appropriate critical questions.
2) Do include all your references, as per the Harvard Referencing System,
3) Please don’t use Wikipedia web site.
4) I need examples from peer reviewed articles or researches.
5) Turnitin.com copy percentage must be 10% or less.
Note: To prepare for this essay please read the required articles that is attached
Appreciate each single moment you spend in writing my paper
Best regards
SAMPLE ANSWER
Chronic Obstructive Pulmonary Disease
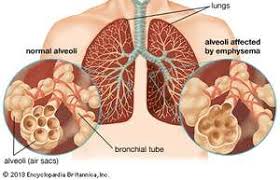
This is a serious lung condition that manifests with emphysema coupled with chronic bronchitis. It is mainly prevalent in patients that are 40 years and above, especially cigarette smokers (Cherney, 2014, Pg. 50). These patients present with symptoms of coughing, production of sputum, or breathlessness. Owing to emphysema, the patients frequently experience shortness of breath, a situation where they have to make an extra effort to inhale sufficient oxygen by maintaining a high speed of breathing. In emphysema, the lungs of patients can only accommodate small volumes of air. There is also a notable deficiency in the amount of oxygen that reaches most body tissues. Old age is a predisposing factor to the disease and more so if associated with excessive smoking (Hanania, Sharma, & Sharafkhaneh, 2010, Pg. 600). It is therefore relevant for gerontological care nurses to give special attention to the condition. This paper not only discusses COPD in details, but also explores further into other secondary conditions associated with the condition. Selected mechanisms applied by nurses in handling COPD patients are also explored in detail. Such methods relate to COPD assessment as well as evaluation. Issues are addressed from the perspective of the nurse as well as from the patient’s perspective.
Assessment of COPD Patients
Just like in most other health care set ups, assessment of COPD requires collection patient’s history, from which an evaluation is made and appropriate medical measures taken. Health officials are expected to conduct history examinations on their patients and eliminate differential diagnoses to zero in to the patient’s status with regard to COPD. A complete history collection usually offer details whether patients or their close relatives have ever been diagnosed with respiratory abnormalities, and more so emphysema, bronchitis or COPD at large. Childhood lung infections and atopic illnesses relate directly with the likelihood of COPD diagnoses on patients. In addition, history collection investigates on the living conditions of the patients, both in the past as well as in the present. In most cases, environment is a significant player in the aetiology of not only COPD, but also other common respiratory disorders. Such experiences as livingor working in dusty places plays are generally a threat to one’s respiratory health (Dweik & Mazzone, 2015, Pg. 10). When attending COPD patients, knowledge on the patient’s exposure to such conditions serves to enhance competence among nurses.The best techniques when attending patients involves nurses’ optimal knowledge on their patients from varied life aspects.
Miller’s Theory
Miller made remarkable contributions in the nursing profession by designing a theory that would guide nurses when attending aged patients. The theory is still widely applied in most health institutions in the world today. The theory has been subjected to constant modifications by its implementers in nursing care. It therefore offers up-to-date guidelines making it very relevant and appropriate for nurses who attend old people. In the present, Miller’s theory is commonly termed as “the functional consequences theory of promoting wellness in older adults” (Hunter, 2012, Pg. 37). He theory offers scientifically supported ways of improving the life quality among the aged populations, in addition to expanding their lifespan. It also relates all aspects of care in an integrated manner. A relationship is developed between nurses and patients with regard to the environment. Its incorporation of factors that affect health lure nurses to its application and to them, the theory just simplifies their day-to-day work. The theory emphasizes on important matters in the care for the aged, such as the risk factors that accompany aging, diminished body functionality as a result of old age and the linkage between one’s mind, body and spirit (Hunter, 2012, Pg. 38). In addition to problem identification, the theory suggests on appropriate ways of handling the challenges. It for instance suggests that care for the aged be directed toward alleviation of the negativity of functionality, the most predominant consequence of risk predisposition. The preferable outcomes achieved with the theory see to it that old people retain their body functionality to the best possible extent.In the care of an old OCPD patient like Kathleen, Miller’s theory is a first-hand instrument for a nurse. Despite the many challenges in her life, like being unable to cook for herself, Kathleen can still restore fun in her life with the application of Miller’s suggestions.
Age-Related Changes in COPD
As a COPD patient ages, like in the case of Kathleen, the ability to maintain wellness is decreased, patients become more prone to respiratory, cardiovascular, musculoskeletal and neurological among other disorders. Kathleen experience depression, which prompts her to seek solace by isolating herself from the community. Such a situation is common with COPD patients following neurological disorders. Again, the lady is observed to express musculoskeletal impairments when her mobility is reduced. The most conspicuous effect of COPD on Kathleen is the impairment of her respiratory system, where she developed shortness of breath as a result of emphysema.
Consequences of negativity in body functionality are also evident in Kathleen case when she fails for instance to cook for herself. Malnutrition is a serious problem and would make life more terrible for the COPD patient. It often results into increased risk to infections (NHS, 2015, Pg. 82). Usually, old people require energy to maintain basic body processes. Other matters of living affected by diagnosis with COPD among old people include physical life: environmental and social; as well as psychological life. To overcome problems associated with COPD, nursing care would involve educating the patients as well as practising the techniques that are suggested to achieve high results, such as the ones provided in Miller’s theory.
Care for COPD Patients
There has been improved research in the field of aetiology and pathophysiology of COPD in the last 50 years. There used to be a mistaken belief that little could be done on the progressive and irreversible nature of COPD. Since COPD is closely related to smoking many patients may feel as if they are not treated well due to a “self-inflicted illness.” It is this view that has commonly evoked an unsympathetic response from the patients’ relatives and unfortunately, some clinicians. Mostly, COPD affects individuals that cannot demand high standards of care such as the elderly and the poor (Bellamy & Booker, 2011, Pg. 89). Nurses should therefore, work toward attaining realistic aims of care provision such as slowing down or stopping the progression of the condition, reducing disability through achieving best possible symptom relief, and decreasing the number and severity of exacerbations.
The Role of Nurses in Care Provision
Early diagnosis is an essential step to attaining the above- stated objectives. Health officials also need to carry out regular reviews in order to make sure that necessary interventions are provided, information and education needs are attained, and signs and symptoms are well managed. The long-term management illness such as COPD is suited well to nurse-led care, so long as the nurse is trained well. COPD has a complex diagnosis and management procedure especially for elderly patients that have co-morbidity. For quality healthcare delivery, nurses should have high-quality training, continued improvement of professional development and work as a team with their colleagues.
Progression of COPD
The only effective intervention that has been identified in the slowing down of COPD progression is smoking cessation. Smoking quickly accelerates the decline of FEV1. However, this can be slowed down to an FEV1 of anon-susceptible smoker or a non-smoker at any level of COPD. Early cessation ensures that a patient acquires better outcomes, but it is not too late.
According to Roach, Bronner and Oreffo, healthcare professionals should create awareness on the subject of smoking cessation at every encounter (Roach, Bronner& Oreffo, 2011, 57). By so doing, they can prompt a smoker that is committed to thinking twice about smoking and its associated consequences. They may also encourage individuals that could be contemplating quitting make a serious cessation.
Some pharmacological medicines have also been developed to help patients quit smoking. Some of these medications include bupropion, varenicline, and nicotine replacement therapy (Kon, Hansel& Barnes, 2011, Pg. 67). Therefore, clinicians should prescribe these medications to smokers that want to quit since they may improve their chances of success. There are some smokers that would like to quit and at the same time require special support. Such smokers should be referred to specialist services.
Reduction of COPD Symptoms
Breathlessness and a persistent cough are disabling and distressing. The primary clinical methods of managing these symptoms are;
- Long and short-acting bronchodilators
- Mucolytics
- Pulmonary rehabilitation
Bronchodilators
These medications only have an effect on FEV1 in COPD. However, they can also reduce the tone of bronchomotor, decrease hyperinflation of the respiratory system and improve the efficiency of respiratory muscles. COPD patients that take bronchodilators breathe efficiently and more comfortably. They also have an improved tolerance to exercise. The main categories of bronchodilators used are beta agonist and anticholinergic bronchodilators.
Mucolytics
These are drugs that aid in reducing sputum viscosity. As a result, they make it easier for patients to clear the sputum. Recent studies have shown that mucolytics can also reduce exacerbation number and improve the symptoms associated with coughing and production of sputum (Lee-Chiong, 2010, Pg. 362). Carnocisteine and mecysteine are some of the mucolytics used for long-term management of COPD.
Pulmonary Rehabilitation
Many COPD patients choose to live with breathlessness by shunning exercises. Patients lose their confidence, self-esteem, feel depressed, and isolate themselves from others. Pulmonary rehabilitation is aimed at reversing this. Patients should focus mainly on aerobic training so that they can condition their muscles once more and their endurance to exercise. Continued exercise also aids in reducing breathlessness. However, for successful pulmonary rehabilitation, patients should be committed and motivated as well. The patients should also be able to exercise as this will co-morbid cardiovascular related diseases and musculoskeletal problems that prevent the patients from exercising accordingly.
Reducing Exacerbations
According to MacNee, ZuWallack & Keenan, patients should be educated on self-management in order to reduce the worsening of exacerbations (MacNee, ZuWallack & Keenan, 2009, Pg. 134). Patients should also be provided with clearly written advice and also taught about when they should seek medical attention. Nurses should also ask patients about the number of exacerbations they experience afterwhich they will prescribe long-acting bronchodilators to those that have frequent exacerbations.
Conclusion
Tremendous progress has been achieved in comprehending the management of COPD. However, COPD is still a considerable burden on some patients and the caregivers but its prospects are quite promising (Bernhardt & Kasko, 2011, Pg. 36). COPD has been has been branded the “Cinderella” disease of the respiratory system, but the chances of “Cinderella” approaching the ball are improving.
Bibliography
Bellamy, D., & Booker, R. (2011). Chronic obstructive pulmonary disease in primary care: All you need to know to manage COPD in your practice.
Bernhardt, N. E., & Kasko, A. M. (2011). Nutrition for middle aged and elderly. New York: Nova Biomedical Books.
Bernhardt, N. E., & Kasko, A. M. (2011). Nutrition for middle aged and elderly. New York: Nova Biomedical Books.
Cherney, K. (2014, September 16). COPD: What’s Age Got to Do with It? Retrieved May 10, 2015 from http://www.healthline.com/health/copd/age-of-onset#Overview1
Dweik, R. A., Mazzone, P. J. (2015). Occupational Lung Disease. Retrieved May 10, 2015 from http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/pulmonary/occupational-lung-disease/Default.htm
Hanania, N. A., Sharma, G., & Sharafkhaneh, A. (2010). COPD in the Elderly. Medscape, 31(5), 596-606
Hunter, S. (2012). Miller’s Nursing for Wellness in Older Adults. Lippincot Williams. 35-45
Kon, O. M., Hansel, T. T., & Barnes, P. J. (2011). Chronic obstructive pulmonary disease: (COPD). Oxford: Oxford University Press.
Lee-Chiong, T. L. (2010). Sleep Medicine Essentials. New York, NY: John Wiley & Sons.
Lötvall, J., & Busse, W. W. (2011). Advances in combination therapy for asthma and COPD. Chichester, West Sussex: John Wiley & Sons.
MacNee, W., ZuWallack, R. L., & Keenan, J. (2009). Clinical management of chronic obstructive pulmonary disease. Caddo, OK: Professional Communications.
NHS. (2015). Malnutrition. Retrieved May 10, 2015 from http://www.nhs.uk/conditions/Malnutrition/Pages/Introduction.aspx
Nici, L., & ZuWallack, R. L. (2012). Chronic obstructive pulmonary disease: Co-morbidities and systemic consequences. New York: Humana Press.
Roach, H. I., Bronner, F., & Oreffo, R. O. C. (2011). Epigenetic aspects of chronic diseases. London: Springer.
Voelkel, N. F., & MacNee, W. (2011). Chronic obstructive lung diseases. Hamilton, Ont: BC Decker.
We can write this or a similar paper for you! Simply fill the order form!
