Developed Programs for Health Promotion and Education Order Instructions:
Developed Programs for Health Promotion and Education
Find a program (provide a link to the program) which was developed to provide health promotion and education to a specific population. Evaluate this program on its ability to identify with the specific population, on its implementation of effective intervention methods, and on its program planning strategy. This evaluation will be very broad in scope and not as in-depth as your research assignment. Review three peers’ postings, access the program links, and compare your assessment to theirs? What additional insights do you have?
Developed Programs for Health Promotion and Education Sample Answer
Programs Developed To Provide Health Promotion and Education
Any population aims at living in a clean, healthy and disease-free environment. This is often achieved only happen when a given population is well conversant with all the rules that revolve around achieving good health.
Kentucky Homeplace (Ruralhealthinfo.org) program was started in the United States to address lifestyle choices, substandard health insurance and environmental factors that have caused an array of avoidable diseases in rural Appalachian Kentucky. Appalachian Kentucky is one of the unhealthiest regions in the United States. This region has had rising cases of obesity, cancer, heart disease and diabetes. Kentucky residents lack the appropriate knowledge regarding health conditions due to cultural inhibitors, poor transport, and financial burdens (Blank, 2013).
The program has greatly brought about improvement in the health and education in more than 29 counties in the Appalachian region, Eastern Kentucky. Kentucky Homeplace trains people who were born in Kentucky as Community Health Workers (CHWs) in a bid to provide access to numerous health services to the population.
Moreover, Kentucky Homeplace has provided free health care services for more than a decade now to the entire population of Kentucky. The free health care services they provide include Eye exams, Diabetes Self-Management, dental services, health coaching for families and free health information.
Kentucky Homeplace over the years has kept the targeted population healthier. This is evidenced by their participation in care coordination and health coaching on chronic disease management, diabetes, preventive screenings and prenatal care. In the last decade, the program has served more than 150,000 clients and have provided over 4 million services with a medication service value of 300 million dollars.
Developed Programs for Health Promotion and Education References
Blank, R. A. (2013). The price of life: the future of American health care. Columbia University Press.
Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Maternal and child health nursing**
Chapter 50: Nursing Care of a Family When a child Has a Vision or Hearing Disorder
Basic nursing: Concepts, skills & reasoning**
Chapter 25: Medicating Patients (sections on “Administering Topical Medications: ophthalmic medications, otic medications”; “Procedures on Administering Ophthalmic Medication, Irrigating the Eyes, and Administering Otic Medication”)
Chapter 31: Sensory Perception (except section on “Seizures”)
Web-Based and Other Professional Resources:
Nursing: Scope and standards of practice (2015)**
Sensory Perceptual Visual and Hearing Disturbances Sample Answer
Sensory Impairment
An individual experiencing sensory impairment may face quite a number of challenges in life. With respect to higher level needs that are defined in Maslow’s hierarchy of needs. A visually challenged individual may find it harder to actualize these higher-level needs. The higher level needs that include self-actualization, self-esteem and love, and belonging needs, are among the particular needs that this paper will try to elaborate on how challenging they are to a visually challenged individual to meet them.
Love and belonging is nature to most if not all human beings. These needs depict the nature of the interpersonal relationships that are adopted by most humans. However, for a visually challenged person. It may be quite difficult for them to find a sense of belonging in an environment that does not favor him or her. Creating interpersonal relationships with people without actually seeing their physical appearance will be the main issue to be dealt with.
Consequently, self-esteem needs are quite important in Maslow’s hierarchy. But for a visually challenged person, attaining this needs may be a challenge. They may find it extremely hard to gain confidence. It might be quite difficult for this particular individual to be able to satisfy his or her desire to be valued by other people when he or she is visually challenged.
Lastly, self-actualization needs are on the pinnacle of Maslow’s hierarchy. Self-actualization entails five key things that are key to human beings. However, for visually challenged individuals, to fully satisfy their self-actualization need may prove to be hard if the person has not yet accepted the impairment condition that faces him or her.
The nursing intervention that would be applied by a registered nurse may include the following practices. First of all, when meeting the patient, the nurse will have to make a good first impression. Reason being the first impression go a long way into helping visually impaired patients feel cared for. This also helps in creating a healthy relationship between the two parties (Treas & Wilkinson, 2013). Second of all, the nurse would help the patient meet their self-esteem and self-actualization goals by helping them get to know the environment they are staying in. This would help them feel confident by not requiring aid all the time to perform the basic life activities from time to time.
Therefore, for a visually impaired individual, the attainment of the love and belonging, self-esteem and self-actualization goals may be a cumbersome task. However, with the application of the right nursing intervention by a registered nurse. The attainment of these needs, in the long run, maybe an overcomeable situation.
Sensory Perceptual Visual and Hearing Disturbances References
Treas, L. S., & Wilkinson, J. M. (2013). Basic nursing: concepts, skills, & reasoning. FA Davis.
Ethical standards in allocation of healthcare resources
Ethical standards in allocation of healthcare resources among the elderly population and end of life care
Order Instructions:
This is a discussion post, I will send three articles that pertains to this paper. Thanks
SAMPLE ANSWER
Ethical standards in allocation of healthcare resources among the elderly population and end of life care
The number of elderly people (65 years) is expected to double to 80 million over the next 30 years. The share of the elderly population will increase 13% – 20% in 2030. This implies that soon, there will be a higher ratio of elderly people as compared children. The population aging is a huge force with political, economic and social implications to the society (Hayutin, Dietz, & Mitchell, 2010). For instance, the rapid increase of cost of healthcare in the past years has created ethical discussion on allocation of resources. The main ethical issue on allocation of resources among the elderly is not entirely based on the quantity of treatment provided, but rather establishing protocols that seek optimum care based on the patient needs (Milstead, 2016).The organization decision making model of healthcare resources among the elderly population and end of life care should be determined by the following ethical standards namely; a) need, b) right, c) merit and d) priority (Craig, 2010, p. 29).
The ethical standard of right highlights the fact that every person is entitled to equal access and consideration of care. As described by Thomas Jefferson in the Declaration of Independence (1776), equality in health care is inherent and inalienable. Therefore, every individual should be given equal opportunity so that they can access quality and safe care without regard to an individual’s capacity or ability to pay. The ethical standard of merit indicates providing care to people based on their needs and fitness. This involves assessing individual cognitive function, degree of illness progression, legal status among others. This ethical framework guides use of the limited resource to yield the most successful outcome (Craig, 2010, p. 29).
The ethical framework of need is based on evaluation of patient’s health status. In this context, an elderly patient who needs cosmetic surgery to repair scaring caused by burn have greater need as compared to another patient’s needs for the same healthcare procedure for rhinoplasty. In this context, the most sever painful conditions should receive preferential treatment during resource allocation (Pavlish et al., 2011). The ethical framework of priority is important especially when ranking patient’s group. In current settings, there lacks effective framework on priority of care, which makes the healthcare providers to use their own discretion to determine who receives care; in most cases, the wealthy receive care before the poor deserving patients. In an ethical resource allocation framework, the priority is always the needy patient, so the monetary gains of an organization must not outweigh the patient’s outcome (Craig, 2010, p.29).
Ethical implications of resource allocations
The shift towards high population rate of the older population has enormous economic, social and political implication to the society. This is because as people live longer, there will be many people above 65 years as compared to children. It is estimated that by 2032, 1 in 5 Americans will be above 65 years. This indicates that there will be fewer potential workers per every retiree, and the financial as well as social cost of the aging population will increase. This indicates that the fiscal burden on tax payers will skyrocket (Hayutin, Dietz, & Mitchell, 2010).
The shift towards population will also challenge resource allocation. Suburbs and traditional nuclear families will increasingly become single and will comprise mainly of the older couples. Diversity will increase among the older people where 60% of the older population will be from minorities. The cost of healthcare is likely to be propelled by increase in technological advancement. Therefore, it is likely that the current healthcare spending might crowd-out spending for other healthcare needs across the country. If no interventions are put in place, the current deficits will leave a high interest for principal payments for future generations (Hayutin, Dietz, & Mitchell, 2010).
Evidently, these unprecedented demographic development calls for an urgent and strategic action. This calls for a deeper understanding so as to effectively deal with the new realities of life. This discussion demonstrates that is appropriate measures are put in place; the high cost of care could be reduced and could free up some resources to reduce public deficits in the future (Crippen & Barnato, 2011, p. 126).
References
Craig, H. D. (2010). Caring enough to provide healthcare: An organizational framework for the ethical delivery of healthcare among aging patients. International Journal for Human Caring, 14(4), 27–30.
Crippen, D., & Barnato, A. E. (2011). The ethical implications of health spending: Death and other expensive conditions. Journal of Law, Medicine & Ethics, 39(2), 121–129. doi:10.1111/j.1748-720X.2011.00582.x\
Milstead, J. A. (2016). Health policy and politics: A nurse’s guide (5th ed.). Burlington, MA: Jones and Bartlett Publishers.
Pavlish, C., Brown-Saltzman, K., Hersh, M., Shirk, M., & Rounkle, A. (2011). Nursing priorities, actions, and regrets for ethical situations in clinical practice. Journal of Nursing Scholarship, 43(4), 385–395. doi:10.1111/j.1547-5069.2011.01422.x
We can write this or a similar paper for you! Simply fill the order form!
This is a discussion post for my class in Policy and Advocacy for Improving Population Health. I will attach the two articles that we are to review for this paper. I will also include the syllabus. Thank you.
Nurses play a critical role in health centers by caring for the approximately 22 million veterans as well as the 3 million reserve members. This population is diverse as it entails frail, elderly veterans who have served in Iraq, Korea, and Afghanistan. Several veterans are returning home in need of healthcare services. One of the health needs that these veterans require is management of the physical wounds that they have acquired during war (Jackonis, Deyton & Hess, 2008). The also require mental care since most of them suffer from post traumatic stress disorder (PTSD) which makes some of them violent or even scared once they are exposed to similar scenarios they went through in the field. The veterans’ family members should also be accorded support majorly because when one of their loved ones has been called to serve, his/her family is affected. Moreover, family dynamics undergo significant changes from the time of deployment of the veteran and adapting once he is back home is quite difficult and stressful process for every family member.
How to advocate for veterans
One of the ways of advocating for veterans is by ensuring that they receive timely, compassionate, and appropriate care once they visit the health center. Moreover, I can advocate for these individuals by ensuring that they know and understand their rights as veterans. I will therefore remind them of these rights and even post them in the outpatient or inpatient areas where they visit frequently. For the homeless, I will endeavor to understand why they are homeless and then help them by forwarding their names to The Department of Veterans Affairs and ensure that they are given a permanent residence.
Advocating skills
While advocating for the veterans, I intend to make use of my communication skills. Begley, (2010) points out that communication is one of the important pillars in nursing practice. With communication, I will engage the veterans effectively and know what they are going through. I will also use these skills when approaching various stakeholders who will provide solutions to the veterans. I can develop the communication skills by ensuring that I use the right body language when talking to the veterans, I maintain eye contact during discussions, and I use the right tone and show compassion when talking to them.
Roles of a nurse as an advocate
As an advocate, a nurse is charged with the responsibility of protecting the patients’ rights (Albina, 2016). For instance, it is a nurse’s responsibility to find out what the patient needs when s/he is sick. The advocates also liaison with between the doctors and patients by helping the patient understand their diagnosis and ensure patient centered care is observed (Choi, 2015). Since patients have different choices and preferences, it is the role of a nurse advocate to suggest alternative treatments for the patient to ensure that he/she is satisfied.
References
Albina, J. K. (2016). Patient abuse in the health care setting: The nurse as patient advocate. AORN journal, 103(1), 73-81.
Begley, A. M. (2010). On being a good nurse: reflections on the past and preparing for the future. International journal of nursing practice, 16(6), 525-532.
Choi, P. P. (2015). Patient advocacy: the role of the nurse. Nursing Standard, 29(41), 52-58.
Jackonis, M. J., Deyton, L., & Hess, W. J. (2008). War, its aftermath, and US health policy: toward a comprehensive health program for America’s military personnel, veterans, and their families.
We can write this or a similar paper for you! Simply fill the order form!
Case Report -Foetal Alcohol Spectrum Disorders
Case: Leena Kerama
Leena is a 26 year old women of Aboriginal decent. She has been admitted to the
mental health unit with a diagnosis of severe alcohol use disorder (DSM V 303.0, ICD10
F10.20) and alcohol-induced depressive disorder (DSMV 291.81). Leena’s past medical
history reveals a 10 year history of severe alcohol dependence consuming an average of
8 to 10 standard drinks of alcohol (wine or beer) per day (which continued during
pregnancy) and a two year history of symptoms of depression (low mood and diminished
interest or pleasure in all or almost all activities) associated with alcohol consumption.
Leena gave birth to a baby boy (Mani) six months ago.
Leena
a) Description of severe alcohol use disorder (DSM V 303.0, ICD10 F10.20) and alcohol-induced depressive disorder (DSMV 291.81)
b) Pathophysiology – the effect alcohol has on the adult brain
c) Signs and Symptoms
d) Contemporary treatment (pharmacological and non-pharmacological)
e) Nursing management within the multidisciplinary care team
f) Treatment outcomes
SAMPLE ANSWER
Introduction
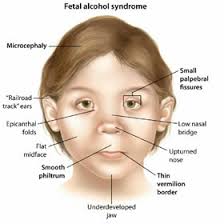
Fetal alcohol spectrum disorder (FASD) is used to refer to a condition that occurs from adverse effects on development especially when alcohol is taken during pregnancy. FASD is a brain disorder that comes with physical abnormalities. According to recent studied FASD is estimated to occur in 1 out of 100 live births but the numbers are higher in areas or communities that alcohol consumption are high (Asia News Monitor, 2015).
FASD is associated with primary disabilities that are directly from toxic effects of alcohol changing cell development. FASD conditions usually affect the nervous system and the brain since the organs are always under construction throughout pregnancy. Therefore the effect on the brain and nervous system leads to lifelong functional, emotional and cognitive difficulties (Asia News Monitor, 2015).
Excessive drinking especially taking 4 or more units per occasion may increase the risk of physical problems and unusual facial features during pregnancy especially in the first trimester. FASD can lead to secondary disabilities including mental health disorder social problems and educational (Asia News Monitor, 2015).
Description of severe alcohol use disorder (DSM V 303.0, ICD10 F10.20) and
Alcohol-induced depressive disorder (DSMV 291.81)
Alcohol Withdrawal is a diagnosis in DSM-5 which might be a life-threatening condition found in people who drink heavily over a period of time, but they then stop or dramatically decrease their alcohol consumption. The consumption period vary from weeks, months or years.
The more the individual drinks during this time, the more likely it is for alcohol withdrawal symptoms to manifest. The manifested symptoms are usually found in adults but may occur among children and youths. The manifestations of alcohol symptoms show the level of addiction.
Pathophysiology – the effect alcohol has on the adult brain
An acute effect of alcohol on human brain has been studied and has helped in rationalizing the development of psychotropic drugs that will assist in treating adverse effects of alcohol.
Alcohol is an addictive drug that stimulates the release of neurotransmitter dopamine from cells that originates in ventral tegmental area of the brain (VTA). THE VTA is associated with behavioral motivation and reward where if exposed to alcohol, dopamine is released into the nucleus known to reinforce drinking behaviors or make the drinking experience more enjoyable (Ritchie & Timothy & Corley & Geraldine & Davies, G., et al, 2014).
Excessive consumption of alcohol also affects the balance between excitatory and inhibitory neurotransmitters. This is because Electrochemical activation of neurons is controlled by the two hence alcohol consumption will inhibit ion flow between excitatory and inhibitory neurotransmitters leading to the imbalance (Ritchie & Timothy & Corley & Geraldine & Davies, G., et al, 2014).
The hippocampus is responsible for memory and learning and alcohol consumption reduces the size of the hippocampus. Alcohol consumption usually affect the hippocampus since its sensitive and contact with alcohol is poisonous to the nerve cells leading to damage to the cell. This therefore may lead to memory lose or may hinder learning altogether (Prakash & Neelu & Amool & et al, 2015).
Adverse consumption of alcohol may lead to lifelong problems including poor impulse control, which leads to unsafe sexual activity and unexpected bouts of violence. An individual may also experience memory loss, blackouts and poor retention of information (Lital & David & Harold, 2013).
An individual may experience permanent inability to walk straight. This because the part of the brain controlling balance is sensitive to alcohol hence continuous consumption may lead to permanent disability especially when the condition cannot be treated anymore (Prakash & Neelu & Amool & et al, 2015).
Signs and Symptoms
Alcohol use disorder ranges from mild, moderate or severe, depending on the number of symptoms one is experiencing. They include:
Inability to limit amount of alcohol intake
Having strong urge to drink alcohol
Spending a lot of money buying alcohol
Failing to do regular obligations including going to work, school or even going home
Continuing to drink alcohol even when one know it’s causing physical, social or interpersonal problems
Withdrawing from interacting with other people or reducing social activities including hobbies
Experiencing withdrawal symptoms such as sweating, shaking and nausea when one is not drinking (Asia News Monitor, 2015).
Contemporary treatment (pharmacological and non-pharmacological)
Treatment of alcohol use disorder is done using the 30-60 days approach where patients attend 2-3 sessions per week and are encouraged to abstain from talking alcohol while other will be given prescription to help them recover. Thereafter the patient enters the continuing care phase where they attend self-help meetings. Contemporary treatment therefore combines the traditional abstinence and staying sober approach with developed drugs to assist alcohol user to completely stop taking alcohol (Mental Health Business Week, 2015).
Patients with mental illness and those dependent on alcohol consumption should be given more care or be treated with professional multidisciplinary team to ensure that they are able to recover (Dennis & Victor & Mady & Brendan, 2013).
Nursing management within the multidisciplinary care team
Patients are usually monitored at least twice per week once they begin the detoxification program by a specialist nurse. The monitoring can be face to face or can be done through the phone. Alcohol content in the body will be taken frequently using urine drug-screening monitor. If any alcohol substance is detected the individual is discontinued from the program or they can start all over (Picci & Francesco & Marco, et al, 2014)
After the detoxification program a follow up treatment should be conducted by the specialist nurse to avoid patients from relapsing. Individual who fears that they may relapse should be given medication to prevent them from relapsing (Kattimani & Bharadwaj, 2013).
Treatment outcome
Most patients after undergoing alcohol detoxification usually recover from the disorder. However a few of them may relapse especially when they indulge in company that takes alcohol. This therefore will require them to start the program all over again in order to gain sobriety (Ken & Kushner &Matt, 2013).
Conclusion
Alcohol use disorder is becoming rampant in the society. Different avenues should be used to educate and treat those affected by the disease. Therefore qualified specialist in the field should be able to identify every patient needs in order to treat them accordingly.
References
Asia News Monitor, (2015). United States: Learn to Recognize the Signs of an Alcohol Problem. Asia News Monitor; Bangkok. 12 May 2015.
Asia News Monitor (2015) United States: Marijuana vs. Alcohol: Which Is Really Worse for Your Health? Asia News Monitor: Bangkok. 07 Oct 2015.
Dennis, M., Victor, C., Mady, C., Brendan, S., (2013). Treating Alcohol and Drug Use Disorders/Alcohol and Drug Use: The Authors Reply. Health Affairs; Chevy Chase32.3. PP. 630.
Kattimani, S., Bharadwaj, B., (2013). Clinical management of alcohol withdrawal: A systematic review. Industrial Psychiatry Journal; Mumbai22.2. Pp. 100-108.
Lital, R., David, T., Harold, W., (2013). Exendin-4 induced glucagon-like peptide-1 receptor activation reverses behavioral impairments of mild traumatic brain injury in mice. Age. Dordrecht35.5. PP. 1621-36.
Mental Health Business Week, (2015). Patents; “Combination Treatment for Alcohol Dependent Patients” in Patent Application Approval Process (USPTO 20150209372). Mental Health Business Week; Atlanta. Aug 22, 2015: PP. 154.
Picci, R., Francesco, O., Marco, Z., et al (2014). Quality of life, alcohol detoxification and relapse: Is quality of life a predictor of relapse or only a secondary outcome measure? Quality of Life Research; Dordrecht23.10. PP. 2757-67.
Prakash, S., Neelu, S., Amool, S., et al (2015). Personality disorder, emotional intelligence, and locus of control of patients with alcohol dependence. Industrial Psychiatry Journal; Mumbai24.1. PP. 40-47.
Ritchie, S. J., Timothy, B. C; Corley, J., Geraldine, M., Davies, G., et al (2014). Alcohol consumption and lifetime change in cognitive ability: a gene × environment interaction study. Age; Dordrecht36.3:PP. 9638.
Winters, Ken C.W., Kushner, Matt, G.K., (2013). Treatment Issues Pertaining to Pathological Gamblers with a Comorbid Disorder. Journal of Gambling Studies, supply toward an Improved Understanding of Comorbidity: New York19.3. PP. 261-7.
We can write this or a similar paper for you! Simply fill the order form!
Privacy and security in electronic health services
Privacy and security in electronic health services
Order Instructions:
Case Assignment
For your Module 4 Case Assignment, in 2-3 pages, answer each of the “questions for discussion” listed below each case. Develop your answers in 150 to 250 words for each question within the context of the background material. In addition, incorporate relevant applicable laws.
Section 1:
Explain the characteristics of technical, physical, and organizational privacy and security concerns.
Section 2: Case 4.8: E-Mail Goes Astray
Kaiser Permanente, one of the nation’s largest health insurers with 8.5 million subscribers, accidentally compromised the confidentiality of the medical information of 858 of its members. The problem occurred when a technician began sending out a large number of e-mail messages that had been backlogged while Kaiser’s system was being upgraded. Some e-mail messages were sent to the wrong recipients. Members access the website and use the e-mail system to fill prescriptions, make appointments, and seek medical advice. Some of the messages contained names, home telephone numbers, medical account numbers, and medical advice. When the technician noticed the problem, he stopped sending out e-mails but did not notify Kaiser managers of the problem. The next morning, two Kaiser subscribers notified the company that they had received other subscribers’ e-mails. The following message appears on the website:
“Your information is confidential. We are dedicated to keeping your personal health information confidential. We take many precautions to make sure others can’t pretend to be you and get your confidential information from the Web site. As long as you don’t give out your PIN, any confidential information you send or receive on this Web site can be seen only by you and Kaiser Permanente staff who have a ‘genuine business need.’ ” The director of Kaiser’s Web site indicated that once the error was discovered, Kaiser officials attempted to telephone each of the subscribers whose e-mails had been sent to the wrong person and, “We have fixed the problem.”
Source: Brubaker B. ‘Sensitive’ Kaiser e-mails go astray. The Washington Post. August 10, 2000: E01.
Questions for Discussion:
1.Who is responsible for the breach in confidentiality? The technician? Kaiser Permanente? And why?
2.Will this breach of confidentiality discourage subscribers from accessing the Kaiser Web site to fill prescriptions and seek medical advice? How can subscribers be reassured that their information will be kept confidential in the future?
Case 4.7: Patients’ Files Used for Obscene Calls
An orthopedic technician who had been convicted of child rape and indecent assault used the password of a former hospital administrator to gain access to confidential medical records of 954 patients at a major hospital. He then made obscene telephone calls to female patients as young as 8 or 9 years old.
The technician’s access to the confidential patient records began in December and continued until he was fired four months later. The hospital was not aware of the problem until a trace on the telephone line of a girl who was receiving obscene calls indicated that the calls originated from the hospital. The computer system failed to detect the outdated password and did not alert employees who were responsible for maintaining the information system that one individual was accessing a large number of patient files. Moreover, the hospital did not conduct background checks when hiring new employees.
Source: Brelis M. Patients’ files allegedly used for obscene calls. The Boston Globe. April 11, 1995: 1.
Questions for Discussion:
1.Should healthcare institutions conduct background checks on new employees who will be allowed access to confidential patient information? What information should be accessible to such employees?
2.How could the hospital have prevented the misuse of patient information from occurring? Was the hospital’s security system at fault for this breach of security?
3.Should the hospital be held accountable for the actions of the technician?
Case 4.44: University Tightens Computer Security
A university is tightening its computer security after hackers broke into a computer at the medical school and secretly used it to generate a flood of e-mail advertisements. Efforts by the university to cope with the break-in have caused balky and intermittent e-mail service for seven months for hundreds of staff members. At least once, e-mail service throughout the system shut down for two days. University officials did not detect the break-in until at least a couple of weeks later, when someone forwarded an advertisement sent by the computer.
A university spokesperson said that no file information was improperly accessed. Instead the hackers merely used the system to generate e-mail promoting other websites. The university announced that $150,000 would be spent to install new equipment to restore the e-mail system. A number of security measures were being upgraded to prevent the computer system from being broken into in the future.
Source: Birch D. Hopkins tightens computer security. The Baltimore Sun. May 29, 1999: 1B-2B.
Questions for Discussion:
1.Are university medical center information systems especially vulnerable to hackers? Why, or why not?
2.Is the medical center accountable for any harm that is caused by unauthorized entry into patient records?
Module Overview
Concerns over the privacy and security of electronic health information fall into two general categories: (1) concerns about inappropriate releases of information from individual organizations and (2) concerns about the systemic flows of information throughout the healthcare industry and related industries. Inappropriate releases from organizations can result either from authorized users who intentionally or unintentionally access or disseminate information in violation of organizational policy or from outsiders who break into an organization’s computer system. The second category, systemic concerns, refers to the open disclosure of patient-identifiable health information to parties that may act against the interests of the specific patient or may otherwise be perceived as invading a patient’s privacy. These concerns arise from the many flows of data across the healthcare system, between and among providers, payers, and secondary users, with or without the patient’s knowledge. These two categories of concerns are conceptually quite different and require different interventions or countermeasures.
Presentations and Required Readings
•The following is primary reading required for this module: Privacy and Security Concerns1
•This article discusses the primary goals of information security in healthcare and examines policy and appropriate uses of medical data: Confidentiality of Electronic Medical Records2
•Zachary Wilson offers a good explanation of the difference between internal and external sources of attacks. Additionally, he illustrates a wide range of vulnerabilities and how they can be exploited. (Do not get hung up in the technical concepts and jargon at this point. We will cover the more technical aspects later in this course.) Vulnerabilities and attacks3
•The following provides a brief overview of basic concepts surrounding information security along with an introduction to vulnerabilities, controls and policies: Security Concepts4
•Read Chapter 4 “Privacy and Confidentiality” from the following book that is available through the eBrary resource, which can be accessed from the TUI CyberLibrary:
?Anderson, J. G. (2002). Ethics and Information Technology : A Case-Based Approach to a Health Care System in Transition. Springer-Verlag New York, Incorporated, Secaucus: NJ. 63-112. Retrieved on September 8, 2007, from the eBrary database.5
•The following is the United States Department of Human Services summary version of the HIPAA Privacy Rule. HIPAA Privacy Rule6
•Wi-Fi Security concerns7
Sources for Presentation Material Referenced Above
For the Record: Protecting Electronic Health Information (1997). Committee on Maintaining Privacy and Security in Health Care Applications of the National Information Infrastructure Protecting Electronic Health Information. Washington, DC, USA: National Academies Press. 54-81. Retrieved from the eBrary database.
Barrows, R. C., and Clayton, P. D. (1996). Privacy, Confidentiality, and Electronic Medical Records. Journal of the American Medical Health Informatics Association, 3 (2), 139-148. Retrieved from the PubMed Central database.
Anderson, J. G. (2002). Ethics and Information Technology : A Case-Based Approach to a Health Care System in Transition. Springer-Verlag New York, Incorporated, Secaucus: NJ. 63-112. Retrieved from the eBrary database.
Alam AS, Al Sabah SAA, Chowdhury AR (2007). Wi-Fi Security The Great Challenge. National Conference on Communication and Information Systems. National Conference on Communication and Information Security.
SAMPLE ANSWER
Section 1
The physical, technical, and organizational privacy and security concerns are categorized into two main forms; concerns about the flow of information systematically within the whole healthcare industry and concerns over the inappropriate release of information within an organization. This may arise when some individuals are given access to some confidential information hence violating a company’s privacy policy (Kshetri, 2013). The systemic concern, on the other hand, is the release of particular patient identifiable information about their health that may be against their wishes hence presenting a major invasion of patient privacy.
The concerns hold different characteristics. For example, there is organizational threats which involve vulnerability of individual organization electronic health records to external or internal agents. Internal agents are those with authorization and have access to information yet they abuse their privileges.
Conversely, external agencies do not have access to the information, yet they try to manipulate the data or rendering the system unusable. Another characteristic includes the concerns that may arise due to sensitive information that could easily be used against the patients as a means of acquiring a leverage over them (Boric-Lubecke et al., 2014). The information mostly targeted are those of celebrities, employers, politicians, and journalists.
The basic approach to countering threats to privacy in healthcare is erecting policies against the act of violation and setting heavy fines against anyone who violates privacy rules. Organizations should also have continuous checkup of their system’s accessibility and employ trustworthy workers to man the system.
Section 2
Case 4.8: Emails Goes Astray
Question 1
The technician was in charge of the breach. The act of not checking the backlogged information before confirming who the email was sent to, suggests so. The other reason was the number of emails sent before realizing the mistake; the medical information of 858 of its members had compromised which is a high volume. Also, instead of reporting the problem to the superiors, the technician left the insurance company to deal with the mistake he had committed. Kaiser Permanente was not responsible for the breach as they even tried to correct and put the subscribers at ease as they handled their information. Under HIPAA privacy rule, the responsibility of health insurers and organizations is to be accountable to the disclosure of their patients and confidential communication. Therefore, Kaiser Permanente did the right thing of informing its subscribers about the technical challenges on the website. They also emphasized on the pretenders warning them in the case of such an issue.
Question 2
The breach will discourage subscribers from the Kaiser web due to reduced trust in confidentiality of the organization. People tend to learn or fear from others mistakes. The subscribers can be reassured by integrating a better system that requires constant change of passwords thus narrowing the margin of email being hacked and informing them. This also ensures that the company adjusts well to the need of the subscribers. Notifying them that they are securing the site for them will make them feel assured and valued. This goes hand in hand with reassuring them that their information is safe. Employing better technicians, to prevent incompetence at work and informing subscribers of the root of the problem after an investigation is essential as it informs the subscribers that the case was not completely forgotten and they are involved in the processes taking place in the organization.
Case 4.7: Patients Files Used for Obscene Calls
Question 1
Clinical centers should carry out background checks on all new employees before allowing access and employ them. It should be carried out by searching through their public records, private investigations, checking their websites and face to face interviews that requires a detailed history of all previous endeavors and checking if it all fits public record (Yüksel, Küpçü & Özkasap, 2017). The main benefits include increased in value of hire, prevents shame of employing criminals, ensures regulatory acquiescence; satisfies industrial standards, reduces chances of drug abuse and less absenteeism and improves workplace safety and security. Information that should be accessible to such employees should be petite. The technician should only be given access to names of patients and medical records under supervision. Allowing such minimal ensures that they do not get the personal information that can be used to irritate patients. The medical files would be required to conduct his work.
Question 2
There are multiple ways of preventing such a breach. The hospital could have performed a full background check on the technician which could have reduced the risk employing an incompetent individual. In the case study, the hospital had employed the technician yet he was previously convicted of indecent assault and child rape. The hospital should have regularly updated the accessibility passwords. The incident in the case study was due to a failure of updating password allowing for the access of the orthopedic technician even after he was fired. The hospital should have to conduct more frequent vulnerability assessments tests; monthly or every two months. Updating the software systems would also have prevented failure on alerting the people in charge of maintaining information systems. The hospital security system was responsible for the breach as it failed to inform the employees in charge of maintaining information systems.
Question 3
For the technician’s actions, the hospital should be held liable. The hospital was responsible for the employment of a rape offender and indecent assault, to begin with; they did not conduct background checks while hiring new employees. The security system of the hospital allowed the technician access even after he was fired. During his time as a technician, supervision was not provided giving him freedom of action. The hospital also granted access to personal confidential information to a technician, yet receptions and secretaries are the people supposed to possess such information. The hospital was not aware till the girl’s obscene calls were traced inside the hospital. The hospital information system, including employees, were incompetent as this could have been noted at early stages but it got to four months.
Case 4.44 University Tightens Computer Security
Question 1
The University Medical Center Information Systems are not vulnerable to hackers. As from the context the hacker who secretly used them to obtain a flood of e-mail for just advertisement purpose suggests that he or she was not interested in the medical information or records within the system. No information is recorded to be missing as reported by the spokesman. The main aim was to create flood email, and any of the superior computer systems would also have been an easy target. Hackers use an external server to avoid detection while sending emails or viruses like Trojan to render a given site useless. They look for the easy access mainframes to operate; in this case, the medical school computers were previously not as well protected the efforts done after the hack. To restore email system they spent $150,000 installation of new equipment and numbers of security measures were upgraded in the process.
Question 2
The health center is responsible for any harm that happens on patient health records. The spokesperson touched on the issue of improper access of information saying that none was obtained. This shows that the medical center should beef up the security of the information and prevent similar hacking cases from occurring in future. Medical centers are bound by Health Insurance Portability and Accountability Act, (HIPAA) rules to prevent disclosure privacy and security of the patients’ information, confidential communication. HIPAA privacy rule safeguards all identifiable health information of patients that is relayed by a covered entity or business associate. The university had the right of protecting its clients’ information against any hackers with the intention of violating the rules of privacy, as per HIPAA, within the medical center. Therefore, expenses on the installations were put across as well as an upgrade and prevent future hacking incidents.
References
Boric-Lubecke, O., Gao, X., Yavari, E., Baboli, M., Singh, A., & Lubecke, V. M. (2014, June). E-healthcare: Remote monitoring, privacy, and security. In Microwave Symposium (IMS), 2014 IEEE MTT-S International (pp. 1-3). IEEE.
Kshetri, N. (2013). Privacy and security issues in cloud computing: The role of institutions and institutional evolution. Telecommunications Policy, 37(4), 372-386.
Yüksel, B., Küpçü, A., & Özkasap, Ö. (2017). Research issues for privacy and security of electronic health services. Future Generation Computer Systems, 68, 1-13.
We can write this or a similar paper for you! Simply fill the order form!
The concept of recovery oriented practice has increasingly become a prominent concept in mental health policy internationally. This notion originated from consumer perspectives that challenged traditional beliefs about course of mental health disorders and the effective treatment strategies, and it has become widely conceptualized that recovery oriented care is a deeply unique process that changes a person’s attitudes, feelings, values, goals and skills with the aim of improving life limitations caused by the mental illness (Doran et al., 2015). Using Janet’s case study Version 1 and Version 2, this essay expounds on the concept of recovery oriented care by focusing on recovery principles; and elaborating how recovery principles differ from clinical principles.
Recovery principles
Recovery principles refer to the collective approach used to respond to the mental health distress by supporting empowerment, autonomy and retention of hope. Fundamentally, the recovery principles focus on the benefit of acknowledging a person as a whole instead of defining them by their deficits or difficulties (Evans et al., 2017). In this context, recovery is supported through the implementation of collaborative and consultative treatment strategies to people with mental health issues. These strategies place the client at the center of care and emphasize on individuals strengths to support their self determination. The recovery principles are core to the professional standards for Australian and New Zealand mental health includes uniqueness of an individual, autonomy, rights and attitude of their carers, treating mentally ill people with dignity and respect, collaborative care enhanced through effective communication (Mental Health Commission, 2012).
Based on recovery principles, helping patients who experience mental health issues with psychotic clinical issues, such as bipolar disorder and schizophrenia, requires a range of skills and attitudes that are developed from sound knowledge foundation as well as inquisitive approach. The core recovery principle in this group of attributes is the ability to establish a respectful support and collaborative relationship (therapeutic alliance) with the client, their relatives, friends and their loved ones (Slade et al., 2014).
The main challenge for clinical practice during the recovery paradigm is the capacity to remain responsive to the patient’s change and family/loved ones concerns. However, this is vital because client’s capacity to exercise autonomy during decision making may fluctuate over time. For instance, the client may change their desired treatment approach frequently or the client’s family may hold different opinions about the best treatment. Therefore, the recovery principles enable the provider to develop the capacity to ‘be with’ instead of insisting on the standard clinical practice. For instance, in Janet’s Case study Version 2, “the psychiatrist was happy to reduce drugs after 10 days when Janet told her how horrible they were” (O’Hagan, 2014, p.227).
From this analysis, the healthcare provider should understand their own feelings and values to this practice. This is because their personal ethical beliefs and values could make them to inadvertently exhibit judgmental behaviors which could compromise care. The mental health care providers should perform rigorous and regular clinical supervision so as to retain clarity in nursing practice (Evans, Nizette, & O’Brien, 2017). Clinical supervision is one of the recovery principle recognized as professional standard for Australian as well and New Zealand mental health nurses. In addition, it is evident that recovery principles are based on reflective care that is not influenced by the individual’s personal values or ethics. These principles emphasize on self determination and collaborative partnership. For instance, in Janet’s case study version 2,Through collaborative treatment approaches, Janet was able to overcome the sexual abuse trauma; she is better, and now works as a mental health nurse, where she uses her experience to guide other mentally ill patient (O’Hagan, 2017, p.228).
The difference between recovery principles and clinical recovery
Recovery can be viewed through different lenses – personal experience (set of workforce competencies/practices) or clinical recovery process. This personal recovery approach is viewed as the post institutional service philosophy because it challenges the bedrock of traditional mental health system (Barder, 2012). Clinical recovery is a concept that emerged from the expertise of mental health care providers, and it entails treating of psychosocial symptoms so as to restore functioning or to bring back the patient’s life back to normal. Recovery principle differs in clinical recovery in that the concept emerged from expertise of people who have lived the experienced or mental illness (Hapell et al., 2013). On the other hand, recovery principle dwells on a deep unique change of a person’s values, attitudes and feelings with the aim of living a satisfactory life within the daily life limitations associated with the illness. It is basically creating a new purpose and meaning in client’s life as she or he grows beyond the catastrophic event associated with the mental illness (Williams et al., 2012).
As depicted in Janet case study Version 1, the traditional healthcare system perceives mental illness with no legitimacy. Most clients experience major mental health issues as frightening, desolate and also destructive. This is because the pain in mentally ill clients is at par with grief and torture of surviving a battle field or that of being accused of heinous crime (Leah, 2012). The only difference is that the latter experiences have legitimacy and the society has a well defined pathway for their justice and recovery; and surviving them is perceived as heroic and is admirable. On the other hand, mental health is met with fear, reproach and pity. Unlike clinical recovery, recovery principles recognize the importance of person recovery in that mental illness is perceived as a full human experience; therefore, it does not support justification for segregation, cruelty and coercion. A society that has person recovery mind concepts has place for people with mental health illness because seeks to provide a better pathway to better life (O’Hagan, 2014).
Another aspect of clinical recovery that acts as bedrock of the unfortunate traditional belief is community’s abdication of responsibility for the mentally ill people to the profession and services. In the current society, people seek answers to human problems from state- authorized profession institutions. Although to some extent this has been of benefit, it is associated with overdependence of deficit oriented institutions and professionals. Their reputed monopoly on expertise has disabled the mentally ill clients by keeping the stuck in the healthcare services as indicated by Janet’s case study version 1, “the mental health system is responsible for the Janet’s terrible state (O’Hagan, 2014, p. 224).
The devaluation of mental illness in conjunction with community abdication has is associated with naïve community consensus around client’s safety, which is based on discriminative assumption that mentally ill people are not responsible of their behavior, and that the mental health institutions and services must take responsibility of their behavior through tightly controlled approaches (Gilburt et al., 2013). The clinical recovery approach develops unsustainable assumptions that mentally ill persons must be controlled like robots; they lack freewill and those mental health institutions and professionals have magical powers to predict and that the strict measures towards the mentally ill people is meant to establish a safer community. Unfortunately, the unrealistic demands have led to increase in risk adverse practices such as liberty restrictions, locked doors and compulsory treatment just as those experienced by Janet Version 1 case study (Berglund, 2012; Ivey et al., 2012).
Clinical recovery is important, but focusing on clinical recovery alone makes the patient to feel defined by their mental health problem, thereby exacerbating the problem. This approach also makes a person to neglect other aspects of lives that could be cultivated and potentially lead to improved wellbeing (Evans & Brown, 2012). Most of the clinicians identify mental illness experiences such as hearing voices a focus of clinical recovery, which not only make it problematic, but also leads to waste or resources in order to get rid of personal idiosyncrasies that otherwise would be the patient’s assets if well understood and work with using the best approaches possible. On the contrary, the recovery principles of the mental health service seek to design treatment strategies for mental illness is that does not only keeping people out of acute crisis so that they can lessen their dependency and burden to the community. The strategies contemplate the possibility of holistic recovery instead of focusing on clinical issues only, which in most cases could be resolved (Le Boutillier et al., 2015).
Conclusion
Mentally ill people are human beings too; they have rights as other citizens and must be allowed to participate in their local communities. To ensure that the mentally ill patients are socially included in the community’s daily life, the society and mental health professions will be required to change their traditional beliefs and unfortunate assumptions about mental health. In this context, the final frontier is eradicating the barriers that prevent people from experiencing their entitlements as the other citizens. This involves transformation of “treat clinical symptoms- and recover” world view. In addition, the mental health systems should give priorities to treatments strategies that help the mentally ill patient to continue re-engaging with their life. However, the most important and the broadest challenge is the societal change. This implies that the mental health professionals should collaborate with people with lived experienced of mental illness to become partners and social activists who challenge the erroneous stigmatizing assumptions associated with mentally ill people which prohibits them from enjoying the same citizenship entitlements as other people in the community.
References
Barder, M.E.(2012). Recovery as the new medical model for psychiatry. Psychiatr Serv 63 (3) 277-279
Berglund, C. A. (2012). Enter the patient. In C. A. Berglund (Ed.), Ethics for health care (4th ed.) (pp.71-97). South Melbourne, Vic: Oxford University Press
Doran, E., Fleming, J., Jordens, C., Stewart, C. L., Letts, J., & Kerridge, I. H. (2015). Managing ethical issues in patient care and the need for clinical ethics support. Australian Health Review, 39(1), 44-50. doi: 10.1071/AH14034
Edwards, K-L., Munro, I., Welch, A. & Robins, A. (2014) Mental Health Nursing: Dimensions of Praxis. (2nd ed) South Melbourne: Oxford University Press.
Evans, J., & Brown, P. (2012). Videbeck’s Mental Health Nursing. Sydney: Lippincott Williams & Wilkins.
Gilburt, H., Slade, M., Bird, V., Oduola, S., & Craig, T. K. (2013). Promoting recovery-oriented practice in mental health services: a quasi-experimental mixed-methods study. BMC psychiatry, 13(1), 167.
Happell, B., Cowin, L., Roper, C. & Lakeman, R. & Cox, L. (2013). Introducing mental health nursing: A service user-orientated approach (2nd Ed). Crow’s Nest, NSW: Allen & Unwin.
Ivey, A., Ivey, M. & Zalaquett, C. with Quirk, K., (2012) Essentials of intentional interviewing: Counselling in a multicultural world (3rd ed). Belmont, USA:Brooks/Cole Cengage Learning.
Jones, K., & Creedy, D. (2012). Health and human behaviour (3rd ed.). South Melbourne, Vic: Oxford University Press.
Leahy, R. (2012) (Ed). Treatment plans and interventions for depression and anxiety disorders (2nd ed). New York; London: Guilford Press
Le Boutillier, C., Chevalier, A., Lawrence, V., Leamy, M., Bird, V. J., Macpherson, R., … & Slade, M. (2015). Staff understanding of recovery-orientated mental health practice: a systematic review and narrative synthesis. Implementation Science, 10(1), 87.
Mental Health Commission. (2012). Blueprint II: Improving mental health and wellbeing for all New Zealanders: How things need to be. Wellington: Mental Health Commission, 52.
O’Hagan, M. (2014). Madness made me: a memoir. New Zealand: Open Box/Potton & Burton.
Slade, M., Amering, M., Farkas, M., Hamilton, B., O’Hagan, M., Panther, G., Perkins, R., Shepherd, G., Tse, S. and Whitley, R. (2014), Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems. World Psychiatry, 13: 12–20. doi:10.1002/wps.20084
Williams, J., Leamy, M., Bird, V., Harding, C., Larsen, J., Le Boutillier, C., … & Slade, M. (2012). Measures of the recovery orientation of mental health services: systematic review. Social psychiatry and psychiatric epidemiology, 47(11), 1827-1835.
We can write this or a similar paper for you! Simply fill the order form!
As your third assignment toward completion of the Session Long Project you are asked to review the paper by A. Mains, A. Coustasse, K. Lykens: Physician Incentives: Managed Care and Ethics and answer the questions below.
1.Consider this idea from the paper: “Medicine is a moral enterprise. Because MCOs are involved in the delivery of medical care, they too, are moral entities. However, MCOs are also businesses.”
2.Explain the idea that the authors sought to convey.
3.Discuss the physician’s dual function under an MCO model of care.
4.What concerns do you have about the physician- patient relationship under MCOs?
Module Overview
Basically, managed care and managed care organizations (MCOs) was championed as a powerful force for containing healthcare costs. We will see that this is not necessarily the case. We will also see that managed care brings up a range of structural issues related to price fixing and market power.
In the United States after World War II, healthcare was based on an indemnity model or fee for service. In this case health insurers simply paid the bills for services ordered by physicians. These traditional plans provided few incentives for cost containment medical decisions.
Responding to the lack of cost containment measures in the indemnity model, private insurers began to “manage care” by exerting influence on the decisions made by physicians. Managed care is the process of structuring or restructuring the healthcare system in terms of financing, purchasing, delivering, measuring, and documenting a broad range of healthcare services and products.
Sometimes this process of restructuring took the form of bureaucratic rules, e.g. requiring physicians to seek administrative approval before proceeding with certain procedures. In other cases, financial incentives were used to shape physician behavior. By the mid 1990’s, “managed care” had become the dominant form of private sector health insurance.1
Today managed care organization (MCO) is a general term used to describe any number of health insurance arrangements that are intended to reduce unnecessary healthcare costs through a variety of mechanisms, including: economic incentives for physicians and patients to select less costly forms of care; programs for reviewing the medical necessity of specific services; increased beneficiary cost sharing; controls on inpatient admissions and lengths of stay; and the intensive management of high-cost healthcare cases.
Managed care organizations are structured with an imperative to consider both the impact on costs and also the impact on doctors’ decisions whether to join their networks.
These considerations by MCOs to both contain costs and attract physicians are influenced by the values and practices that physicians bring to healthcare. Physicians want to earn a living but not at the risk of endangering the lives they are meant to serve. These healthcare values held by physicians pose a strategic dilemma for managed care organizations needing to contain costs and attract physicians to assemble provider networks.
Low cost MCOs with contract restrictions on spending are seen as highly restrictive. On the other hand, MCOs with large physician networks write cost containment rules into contracts that are not overly burdensome.
It is interesting to think about how MCOs balance competing interests and ethical issues in cost containment, physician ideals, and quality of care.
There are a wide variety of managed care models that integrate financing and management with the delivery of healthcare services to an enrolled population.
Health Maintenance Organizations: HMOs are organized healthcare systems that are responsible for both the financing and the delivery of a broad range of comprehensive health services to an enrolled population. HMOs act both as insurer and provider of healthcare services. They charge employers a fixed premium for each subscriber. An independent practice association (IPA)-model HMO provides medical care to its subscribers through contracts it establishes with independent physicians. In a staff-model HMO, the physicians would normally be full-time employees of the HMO. Individuals who subscribe to an HMO are often limited to the panel of physicians who have contracted with the HMO to provide services to its subscribers.
Preferred provider organizations (PPOs) are entities through which employer health benefit plans and health insurance carriers contract to purchase healthcare services for covered beneficiaries from a selected group of participating providers. Most states have specific PPO laws that directly regulate such entities.
Exclusive provider organizations (EPOs) limit their beneficiaries to participating providers for any healthcare services. EPOs use a gatekeeper approach to authorize non–primary care services. The primary difference between an HMO and an EPO is that the former is regulated under HMO laws and regulations, whereas the latter is regulated under insurance laws and regulations.
These integrated health delivery organizations raise a variety of issues with the Department of Justice and the Federal Trade Commission. The issues include price fixing and antitrust problems based on market power.
Depending on how the groups are organized- horizontal versus vertical- and who is integrated- competing physician groups or a multi provider network a MCO may violate several antitrust laws.
Whenever an MCO possesses significant market power or deals with a group that has significant market power, antitrust implications should be considered. To determine market power, it is necessary first to identify the market in which the entity exercises power. For antitrust purposes, the relevant market has two components: (1) a product component and (2) a geographic component.
Price fixing is considered a per se violation of the antitrust laws. Per Se Violations conclusively violate antitrust laws and means there is no further investigation of its effects on the competitiveness of the market because its intentions are so obvious. A Per Se Violation would almost always limit competition and decrease productivity. Activities that fall under per se violations are acts such as horizontal price fixing and horizontal market division.
Price fixing occurs when two or more competitors come together to decide on a price that will be charged for services or goods. The per se rule applies to restraints in trade that are so inimical to competition and so unjustified that they are presumed to be unreasonable and, therefore, are illegal.
Aaron, Henry J. and Reischauer, Robert D., (1995) “The Medicare Reform Debate: What is the Next Step?” Health Affiars. 14:4. p.8-30
Required Reading
D.A. Mains, A. Coustasse, K. Lykens: Physician Incentives: Managed Care and Ethics. The Internet Journal of Law, Healthcare and Ethics. 2004 Volume 2 Number 1. DOI: 10.5580/24ae – See more at: http://ispub.com/IJLHE/2/1/12416
Diagnosing Physician-Hospital Organizations. Susan A. Creighton. Federal Trade Commission Remarks Before American Health Lawyers Association, Program on Legal Issues Affecting Academic Medical Centers and Other Teaching Institutions. January 22, 2004. Washington, DC. Retrieved from: http://www.ftc.gov/public-statements/2004/01/diagnosing-physician-hospital-organizations
Statement of department of justice and federal trade commission enforcement policy on multiprovider networks; Federal Trade Commission; Competition in The Healthcare Market place; Statements of Health Care Antitrust Enforcement Policy; Statement 9. (July 8, 2009). Retrieved from: http://www.law.uh.edu/faculty/jmantel/health-law/Statement9AntitrustEnforcementPolicy.pdf
The above policy has been updated (Statement 9 on Multi-provider Network), Read the updates below:
“Medicine is a moral enterprise. Because MCOs are involved in the delivery of medical care, they too are moral entities. However, MCOs are also businesses.”
MCOs are moral entities because they aim at deliver quality, safe and effective medical care. They are responsible of doing what is right and best for the service users while ensuring equitable distribution of the scarce health resources. However, the managed care control changes the patient physician relationship to a business-consumer relationship. This implies that the main goal of MCOs is to ensure that physicians adopts the principle of distributive ethic; which is basically providing the most safe and best quality of care to the greatest number of patients as possible using the allotted budget or incurring losses (Mains, Coustasse, & Lykens, 2004).
Under this moral obligation, the MCOs are guided by the utilitarianism- which basically entails performing the best action that maximizes utility. However, the MCOs are economic tenets that aim at reducing costs for service users and aims at generating profit simultaneously. Therefore, when making decisions regarding MCOs, providers should consider the economic effects when maintaining aggregating costs of care so as to avoid loses in either the MCOs or the physicians. This involves establishing control, incentives, bonuses, and withholds as well as other quality assurance initiatives that will ensure that physician practices are safe, quality and profit generating (Cooper and Rebitzer, 2004).
Physician dual function
In managed care, the physicians have dual functions namely a) patient fiduciary and b) Financial advocates. The physician play the unrestricted role of patient advocates by ensuring that the managed care model puts into consideration to patient’s autonomy, respects it, and exercise the ethical principle of beneficence. This implies that the physicians are patient’s advocates in voicing their concerns whenever the managed care model prioritizes its benefits over the patient’s interests, or any other good that is beyond establishing effective physician-patient relationship. This is an important role because the MCOs require expects the physicians to choose the society wellbeing over individual patient’s interest (Mains, Coustasse, & Lykens, 2004).
Therefore, when enrolling in these organizations, it is important for the physicians to understand that their first role is to be patient advocates. Under patient fiduciary role, the physicians are legally responsible for advising patients about all possible alternative care or technological advancement that can be used to manage their illness. The physicians are expected to remain prudent steward when advising and deciding the limits of patient care. This entails balancing between medical merits and financial risks. Trust, honesty and caring are foundation of establishing effective physician-patient fiduciary relationship (Cooper and Rebitzer, 2004).
Concerns about physician-patient relationship
Managed care is associated with moral and professional ethical dilemmas. For instance, MCOs focus on financial incentives and social optimal outcomes instead of single patient well-being. This brings forth the concept of “countervailing agency” which is basically the physician’s role to choose between individual patient’s interests and the society wellbeing. If a patient does not receive care as by MCOs, the physicians can be sued for malpractice. This puts the physicians at dilemma of delivering care based on MCOs expectations and risk for liability (Mains, Coustasse, & Lykens, 2004).
In addition, the MCOs emphasize on utilitarianism approach when solving the healthcare expenditure. Despite its advantages, this approach raises concerns of its validity and morality in physician- patient relationship. The professional sovereignty vs. physician financial incentives complex interaction results into a conflict of interest. It is important for the managers in healthcare system to choose a strategy that helps them identify how to favor the interests of the patients and the society. This calls for reforms to re-define the moral mission for MCOs to fulfill their goals and to preserve efficient physician-patient relationship ( Improving Health Care, 2004).
Mains, D.A., Coustasse, A., & Lykens, C.K. (2004). Physician Incentives: Managed Care and Ethics. The Internet Journal of Law, Healthcare and Ethics. Volume 2 Number 1. DOI: 10.5580/24ae – Retrieved from http://ispub.com/IJLHE/2/1/12416
Health Information System Case Assignment Order Instructions: Case Assignment
1. For this Case Assignment, you will be assuming the role of a lead person on a technology review committee at a multi-facility regional hospital. Your committee has been tasked with evaluating the plausibility and possible selection of a new Health Information System that will enable the hospital to electronically collect and share patient medical history information among its various hospital centers and departments.
Health Information System Case Assignment
2. Currently, each hospital center maintains paper copies and files of patient records, which are separately managed and stored at each facility. Few of the electronically based information systems are integrated between the various centers and locations.
3. To add to the challenge, the CIO informs you that most of the members on the committee have limited experience with information systems and databases. However, the CIO is aware that you are studying Health Informatics, so she has asked you to help familiarize the committee with fundamental concepts related to database systems and relevant health information standards.
4. Specifically, the CIO (and your professor) request that you prepare a brief overview of the following:
• Fundamentals of database characteristics and structure.
• Various types of medical data and information record relevant to this project.
• The importance of uniform terminology, coding, and standardization of the data.
• Various information standards and organizations that may be applicable, and possibly required, for this project.
1. In addition, search the Internet and find three healthcare information systems vendors that offer electronic medical record products. Compare and contrast the functions and features of each product and barriers to implementation (financial, physical, and personnel).
2. Remember, your committee mostly comprises clinicians and other healthcare practitioners. Accordingly, they do not have a great deal of technical knowledge related to information systems.
3. Submit your assignment by the end of this module.
Health Information System Case Assignment Module Overview
There is a need to describe healthcare concepts in a consistent manner. We as humans are able to assimilate, without confusion, many variations of descriptions. Computers, on the other hand, are very poor at recognizing concepts from inconsistent descriptions.
A preferred term is an agreed-upon short description of a concept, and a concept is an image created by the words that describe it. However, in some cases, a definition of a concept may still be needed. This is because, too often, the wording of a preferred term means something different to different users.
A unique identifier (or code) for each concept is required. Anything would do, as long as it is unique and suitable. If a preferred term is used, its description should not be changed; however, it does sometimes happen. Accordingly, a preferred term is generally not suitable as a code. In fact, words are not efficient ways to store identifiers in computers, as the computer may be required to store an identifier many times. Therefore, the code should be reasonably “compact,” preferably a “number” of some sort. Using a number is not an issue, because the computer can always display equivalent descriptive words that are seen by the users.
Coding is the process of matching a healthcare entity to a term in terminology and assigning it a code. The terminology may be called a coding system. Sometimes rules are offered to improve the accuracy of coding. These rules are commonly known as standards.
In this module, we will explore the language of Health Informatics. We will examine database fundamentals and types of health information data and records, and explore standards used to ensure the information is understood across various systems and disciplines.
This module covers a large amount of area and material. Do not get overwhelmed by trying to dig too deeply into the technical aspects. Indeed, each area can be an entire field of technical study of its own. Instead, focus on the concepts, application, and purpose surrounding structured data and standards as they relate to healthcare information.
Presentations and Required Reading
• Carefully read through the following material, which describes the fundamentals of databases, and their structure and function.
Health Information System Case Assignment and the Fundamental Database Characteristics
• Eric McCreath provides a well-illustrated and concise overview of database fundamentals in the following presentation: Database Basics Presentation2
• The following slide presentation identifies various types of medical data and records. Presentation by Peter Szolovits, MIT (February 2002). Nature of Medical Data3
• There are many standards guiding the format and use of healthcare-related information. The following is a comprehensive list and review of these standards. It is not necessary to memorize every one of them. Instead, just get a sense for the vast number of standards that exist. Pay particular attention to those standards that reference Health Level Seven (HL7) and Unified Medical Language System (UMLS). Review of Healthcare Information Standards4
• The following is a list of Standards Organizations. Standards Development Organizations5
• Read through this overview of the Unified Medical Language System. UMLS6
• Jiang Bo provides a good overview of Health Level Seven (HL7) in this presentation. HL77
Sources for Presentation Material Referenced Above
1Beaumont, R. (2000). Database and Database Management Systems. Retrieved from Fundamental Database Characteristics
2McCreath, E. (2002). Lecture Notes for COMP1200: Perspectives on Computing, Information Systems Database Basics. Retrieved from Database Basics Presentation
3Szolovits, P. (2003). Nature of Medical Data. MIT, Intro to Medical Informatics: Lecture-2. Retrieved from http://groups.csail.mit.edu/medg/courses/6872/2003/slides/lecture2-print.pdf
4Blair, J. S. (1999). An Overview of Healthcare Information Standards, IBM Healthcare Solutions. Retrieved from Review of Healthcare Information Standards
5Health Level Seven: Links to Standards Developers. Retrieved from Standards Development Organizations
6Unified Medical Language Fact Sheet. (2003). National Library of Medicine: Office of Communications and Public Liaison. Retrieve dfrom http://www.nlm.nih.gov/pubs/factsheets/umls.html
7Bo, J. (2003). Health Level Seven Overview Presentation. Bioinformatics Institute. Retrieved from HL7
Health Information System Case Assignment Sample Answer
Health Information System
Database management
A general database correlated with all the data of study is usually collected once within a well-defined as well as stated period. The study involves the collection of specific data that comprise data and medical records of previous dates used to diagnose medical complications. However, this study does not relate to those that are carried out for prevalent unique and rare diseases. Additionally, all the findings are computed and calculated with resolute averages and any other statistical methodologies involving calculations of frequency. General databases also comprise methods that make use of individual data performance (Alexander, 2016). These databases assist individual’s assessment in the most probable manner.
Effective health informatics and information system give the mechanism of the best organization. The structure and characteristic of the health database in health informatics are that the database is reliable and able to store all kinds of data relating to any medical records. The database may contain a table of entities that should be easily correlated by all departments in the health setting. This will imply that the relationship between the tables of entities can easily be defined. The tables of objects should be easily mapped to give the best interpretation concerning the medical data and information records.
The senior management plays a vital role in decision making and the formularization of the planning process. In the health information system, the senior management is concerned with;
Recognizing the complexities of the database and ease any of the arising complications by providing solutions about the health database.
Developing suitable website advanced content and help in developing essential management for the web content.
Developing a content of learning management in a healthcare information system.
Therefore, with this health information database, it is assumed that the senior management committee plays an important role within the organization with a sole mandate of structuring efficient health informatics that develops the structure in its entirety.
Health Information System Case Assignment and the Medical Records
West, Borland & Hammond (2015) point out that electronic medical and information records documents information about the patient including current diagnosis, medical and past medical history, treatment, family history as well as all relevant information corresponding to the patient treatment. They are only released under patient or physician authorization.
This information and records about the patient are kept up to date and mark so that reference can be made in future.
The records are usually in a tabulated form containing DOB columns, patient’s name, and the name of the physician, clinical diagnosis, and the treatment plan used. All other relevant information on the patient is contained in the Meta-data. Programming of reports and queries is also necessary. Moreover, the data format that is used should be in the simplest way possible to be readable and comprehended by any other person in health informatics.
The medical records in pocket card files and letter size folders are designed in a manner that follows the format of coding systems and uniform technology that is a standard feature for all other benefits such as:
The UMLS project can develop computer-based “Knowledge sources” that allows applications to retrieve any lost information arising due to terminology differences and relevant information scattering across databases.
It can allow for easy linkage of information systems such as bibliographic databases, expert systems, factual databases, and technology-based patient medical records.
Health Information Standards
The formation of this healthcare information system and infrastructure needs the incorporation of new and already existing architectures, services, and application systems. The fundamental elements of this system are patient-oriented care that is simplified and enabled by a Computer-based Patient Record system (CPR). Furthermore, continuousness of any healthcare enabled and supported by allotment, sharing, and distribution of relevant patient information on all information databases and networks, and the measurement outcomes are assisted by the specificity and greater availability of information regarding healthcare informatics.
Coding of health information has changed over time because narrative clinical text can now be translated to procedure and diagnosis codes. Coded data are gaining relevance in its use in the assessment of quality healthcare, severity adjustments, evaluation of patient safety, surveillance of public healthcare, supporting the decision in algorithm development. Coding can meet the standards of an evolving need to capture medical data in a simple and standardized format with a universal meaning applied at aggregate and individual levels. Data standardization has enhanced interpretation of health information and the understanding of accuracy and quality of data presented in a set of codes (Elkin et al., 2016). It has also allowed for great transformational changes in classification systems in health and clinical terminology.
Medical records in databases identify both physicians and doctors in a manner that maintains organization privacy and continuity. For instance, the patient medical records are recognized and identified with a unique Social Security Number (SSN). Physicians are also identified with their Universal Doctor numbers for purposes of registration in databases.
The National Provider File is being developed by the Healthcare Financing Administration (HFCA) to create a new identifier and provider for Medicaid and Medicare services to include all sites-of-care and caregivers. It will also make Medicaid programs available such as those provided by Cthe enter for Medicaid and Medicare Services (CMS). These can also include government agencies that adopt search services. Also, the Healthcare Financing Administration (HFCA) has also helped define the primary Medicare identifiers of provider services.
The Uniform Cord Council maintains the Universal Product Code (UPC). This UPC is used to label all healthcare products that are sold or supplied in retail settings. Moreover, The National Drug Code (NDC) is an important identifier in healthcare informatics.
Health Information System Case Assignment References
Alexander, S. (2016). Designing a Database to Facilitate Efficient Information Management at the Health Mentors Program Office.
Elkin, P. L., Johnson, H. C., Callahan, M. R., & Classen, D. C. (2016). Improving patient safety reporting with the common formats: Common data representation for Patient Safety Organizations. Journal of Biomedical Informatics, 64, 116-121.
West, V. L., Borland, D., & Hammond, W. E. (2015). Innovative information visualization of electronic health record data: a systematic review. Journal of the American Medical Informatics Association, 22(2), 330-339.
Assignment Instructions
• You will each choose 3 different journal published research study articles that explain the patient’s behavioral and/or psychological responses to having the illness. Do not include articles discussing the physiology or pharmacology of the illness, treatment of the illness or behavioral/psychological responses, or the risk factors for first developing the illness.
• Locate relevant journal published research study articles (these articles need to have been written after 1997 and you must NOT use general literature review articles.
• Choose the 3 articles that best relate to your case study patient.
• Briefly summaries the main topic and focus of each study and include a very summary of the study’s methodology, results, and discussion (i.e. where the authors explain the reasons for their findings and research conclusions) for the articles;
• discuss how each article explicitly and specifically explains the behavioral and psychological responses that the patient in your case study is experiencing in response to their illness.
• Make sure you are using article databases such as PsycINFO, MEDLINE, and CINAHL to run your searches. PsycINFO is likely to find you the most relevant articles for this assignment and all assignments within the behavioral stream. Just using Google or Google Scholar will NOT find you the articles you need. Also, make sure that the search terms you are using will give the databases the best chance of returning the articles you want. If you get no results with one search term, then try another or try and think laterally (e.g. what might be another word for “aggression” that you might find in the literature… hint: what about “irritability”? Or another word for “anxiety” might be “fear” etc.).
• The articles you include must have been published in a journal. Do not include theses, magazines, books or book chapters, letter to the editor or news articles. Academic journals publish all sorts of articles including research studies, book reviews, general literature reviews, editorials/commentaries, letters) but for the articles you include in your Annotated Bibliography you need to use only research study articles. A research study article will describe in detail a qualitative or quantitative research study (e.g., an experiment) including information about the study’s methodology, results, discussion and conclusions. For example, the Module 1 reading Zeilani and Seymour (2012) qualifies as a research study article because the authors describe how they collected and analyzed their data. A Module 3 reading, Lusk and Lash (2005) is a general literature review and does not qualify as a research study as the author does not specify how they went about sourcing information for their article. Lusk and Lash’s article is still a credible and valid source of reference information but it is not a research study and so cannot be used in the Annotated Bibliography assignment.
SAMPLE ANSWER
Peritonitis is a health condition that involves the inflammation of peritoneum (thin protective tissue layer that underlie the abdomen). This health condition is caused by infection which spreads around the body. It requires immediate treatment to prevent fatal complications from arising. In patients who have undergone surgical treatment, autonomic responses, mood swings and psychological coping responses are common. This paper explores 3 different journal study articles that explain patient’s behavioral and psychological responses to this illness. This study focuses on behavioral and psychosocial responses following surgical responses.
Boer, K. R., Mahler, C. W., Unlu, C., Lamme, B., Vroom, M. B., Sprangers, M. A., … Boermeester, M. A. (2007). Long-term prevalence of post-traumatic stress disorder symptoms in patients after secondary peritonitis. Critical Care, 11(1), R30.
Introduction/Literature review: This study investigates the behavioral response following secondary peritonitis. This is because numerous hospital admissions and intensive care unit (ICU) can be physically, emotionally and financially exhaustive. Patients who survive critical illness report critical poor quality of live and symptomology (PTSD) such as numbing, anxiety, loss of avoidant and intrusive recollections. The study suggests that the behavioral interventions are vital in patients with secondary peritonitis.
Methodology: This is a retrospective cohort in patients diagnosed with secondary peritonitis. The study comprises of 278 patients who had undergone surgery for secondary peritonitis, where 131 of them were long term survivors. The patients were interviewed Post-traumatic Stress Syndrome 10-question inventory (PTSS-10).
Study/ Results: The study indicates that in a cohort of 100 patients diagnosed with secondary peritonitis, 86% of them presented with post traumatic stress disorder. PTSD related symptoms were also present in 4.3 times higher in older male patients.
Discussion/explanation: The study indicates that 25% patients who have received surgical treatment for peritonitis are likely to be emotionally and physically upset due to surgical-related trauma, which could exacerbate illness behavior. The study suggests that patterns of behavior are seen as a product of socio-cultural conditioning and coping strategies. The study suggests that healthcare providers should recognize patient’s responses to various health procedures associated with pain and anxiety. Other symptoms such as impaired appetite, lack of energy and disturbed sleep can occur due to illness. In addition, some treatments can affect patient’s mood. These conditions can also be aggravated by other environmental factors such as financial strain of lack of physical and emotional support.
Application to the case study: The study findings contribute to the body of research that demonstrates that psychosocial responses in patients are associated with the socio-cultural factors. The suggests that the healthcare providers should incorporate psychosocial interventions in routine care so as to help patients such as Mr. Jacobs to manage stress associated with their new lifestyles of dependency, helplessness and pain. It is important for the healthcare providers to identify and be aware of this hidden morbidity among the patients diagnosed with secondary peritonitis.
Jennifer Finnegan-John and Veronica J. Thomas, “The Psychosocial Experience of Patients with End-Stage Renal Disease and Its Impact on Quality of Life: Findings from a Needs Assessment to Shape a Service,” ISRN Nephrology, vol. 2013, Article ID 308986, 8 pages, 2013. doi:10.5402/2013/308986
Introduction/Literature review: This study investigates the psychosocial experiences in patients with end stage renal disease. The study conducts needs assessment on renal patients to explore their psychological, spiritual and social needs. The study objective was to investigate behavioral responses and to conduct needs assessment so as to develop a comprehensive health psychology that can run concurrently with renal counseling.
Methodology: The study design is prospective qualitative. The study population consisted of 50 patients with end stage renal disease. The mean age of the participants was 55 years and 40% of them were from black and minority ethnic group. The study utilized series of semi- structured face to face interviews in renal patients and their carers in order to explore their behavioral and psychological responses and how the disease impacted their quality of life.
Study/ Results: The study findings indicated that depressive symptoms and disruptive behaviors are common in renal patients. This is associated with the psychological burden associated with the disease. Most of the patients in the study had feelings associated with depression and anxiety.
Discussion/explanation: This retrospective study indicates that depression and anxiety is a common behavioral response in patient diagnosed with renal disease. The study suggests that about 25% of patients who are diagnosed with the disease suffer from psychological burden. This behavioral response is associated with emotional numbness, avoidance of social activities and events. It is also associated difficulty in sleeping, disruptive and reckless behavior and is easily irritated. The study states that these are body responses to stress or perceived threat.
Application to the case study: The study indicates that depression and anxiety is a behavioral response that goes beyond the mental health. Based on this study, Mr. Jacob’s behavioral responses (irritability, social isolation and binge drinking) could be associated with the emotional burden of the disease. This research is interesting because it suggests that healthcare providers should engage with psychiatrists to help them better manage their improved outcome health.
Mckercher, C.M., Venn, A.J., Blizzard, L., Nelson, M., Palmer, A., Sshby, M., Scott, J., and Jose. M.D. (2012). Psychosocial factors in adults with chronic kidney disease: characteristics of pilot participants in the Tasmanian Chronic Kidney Disease study. BMC Nephrology, 14:83DOI: 10.1186/1471-2369-14-83
Introduction/Literature review: This study investigates behavioral and psychosocial responses in patient diagnosed with chronic illness. The literature links health outcomes with depression, anxiety and dispositional tendency described by aggression, cynicism attitudes and anger/irritability. The study also indicates that hostility, anger and depression are related with renal failure experiences. According to this study, these psychosocial responses are controlled by biomedical risk factors, and are associated with most aspects of immune function.
Methodology: This study design is quantitative. The study consisted of 105 patients above 18 years diagnosed with stage 4 CKD and was not under dialysis. The measures used in this study include depression (9- item patient Health questionnaire) and Beck Anxiety Inventory to investigate behavioral responses with disease progression and patient’s quality of life.
Study/ Results: The study findings indicated that hostility and patient’s behavioral responses to chronic disease are correlated with their plasma levels of CRP. The study findings indicated that the cycle of inflammation levels influence depressive behavior, indicating that depression is problematic indicator of patients under chronic pain.
Discussion/explanation: The longitudinal study findings indicated that there is a relationship between the CRP levels and psychosocial factors. The study also states that hormonal changes also induce inflammatory processes which in turn influence psychosocial responses. For instance, pain initiates systemic stress which activates neuro-endocrinological pathways (hypothalamic-pituitary-adrenal axis) leading to the secretion of stress hormone. Accumulation of stress hormone is associated with hostility and depressive symptoms. The study also suggests that genetic predispositions play a major role in both inflammation and hostility.
Application to the case study: The study findings contribute to the body of research that demonstrates that psychosocial responses in patients are associated with systemic inflammation. This indicates that the Mr. Jacob’s depressive behavior (irritability, social isolation and binge drinking) is associated with elevated levels of the systemic inflammation. This research is interesting because it suggests that healthcare providers should reduce systemic inflammation so as to improve patient’s ability to improve pain, and to help them cope with the illness-induced stress in their lives.
References
Boer, K. R., Mahler, C. W., Unlu, C., Lamme, B., Vroom, M. B., Sprangers, M. A., … Boermeester, M. A. (2007). Long-term prevalence of post-traumatic stress disorder symptoms in patients after secondary peritonitis. Critical Care, 11(1), R30. Retrieved from http://doi.org/10.1186/cc5710
Jennifer Finnegan-John and Veronica J. Thomas, “The Psychosocial Experience of Patients with End-Stage Renal Disease and Its Impact on Quality of Life: Findings from a Needs Assessment to Shape a Service,” ISRN Nephrology, vol. 2013, Article ID 308986, 8 pages, 2013. doi:10.5402/2013/308986
Mckercher, C.M., Venn, A.J., Blizzard, L., Nelson, M., Palmer, A., Sshby, M., Scott, J., and Jose. M.D. (2012). Psychosocial factors in adults with chronic kidney disease: characteristics of pilot participants in the Tasmanian Chronic Kidney Disease study. BMC Nephrology, 14:83DOI: 10.1186/1471-2369-14-83
We can write this or a similar paper for you! Simply fill the order form!