Psychopathology of HIV and Inflammatory Bowel disease
Psychopathology of HIV and Inflammatory Bowel disease
Order Instructions:
Post on or before Day 3 a brief description of the pathophysiology of your selected immune disorders. Explain how the maladaptive and physiological responses of the two disorders differ. Finally, explain how the factor you selected might impact the pathophysiology of each disorder. Disorders I chose are HIV and Inflammatory Bowel disease
SAMPLE ANSWER
HIV
Pathophysiology
Once the HIV virus gains entry into the cells, it attaches to the CD4 receptors as well as co-receptor through glycoproteins links. The virus encodes reverse transcriptase, allowing a copy of genetic component (DNA) to be constructed from viral RNA. Once integrated in the cells, the provirus can remain quiescent for a long period of time. The virus uses host cell machinery for replication process. Within few weeks, the virus will have replicated over 10million viral aspects per microlitre of plasma. This causes a decline in the amount of CD4 counts and immune mediators resulting to opportunistic infections (Hickey, Gounder, Moosa, & Drain, 2015).
Maladaptive and psychological response
The mutation rate of the virus is very high, causing increased resistance to HIV treatment. The virus uses host cell machinery for replication process. The Host initial response to the virus is determined genetically. Coping challenges fluctuates as the disease progress from one stage to another. Additionally, the patient gets depressed and their social roles and functions are adversely affected due to stigmatization and financial implication (Hickey, Gounder, Moosa, & Drain, 2015).
Inflammatory Bowel disease
Pathophysiology
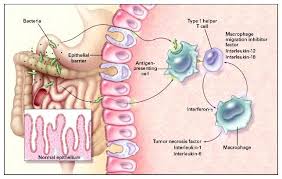
Inflammatory Bowel disease (IBD) is caused by dys-regulated immune response to intestinal micro-flora. The inflammation mainly occurs on the mucosa lining of the intestinal tract which forms ulceration, bleeding, and edema. Several studies indicates that IBD is influenced by genetic factors as well as inflammatory mediators such as cytokines, T cells, Helper T cells of both type 1 and Type 2 (Severance et al., 2013).
Maladaptive and psychological response
Research indicates that psychosocial factors offer an important role in clinical manifestation and pathophysiology. However, most of the patient could present psychological disorders such as depression, insomnia and anxiety. Psychosocial factors are thought to mediate alterations of immune systems resulting to immune mediated diseases such as Cancer and opportunistic diseases (Sajadinejad et al., 2012).
References
Hickey, A., Gounder, L., Moosa, M., & Drain, P. (2015). A systematic review of hepatic tuberculosis with considerations in human immunodeficiency virus co-infection. BMC Infect Dis, 15(1). doi:10.1186/s12879-015-0944-6
Sajadinejad, M., Asgari, K., Molavi, H., Kalantari, M., & Adibi, P. (2012). Psychological Issues in Inflammatory Bowel Disease: An Overview. Gastroenterology Research And Practice, 2012, 1-11. doi:10.1155/2012/106502
Severance, E., Gressitt, K., Yang, S., Stallings, C., Origoni, A., & Vaughan, C. et al. (2013). Seroreactive marker for inflammatory bowel disease and associations with antibodies to dietary proteins in bipolar disorder. Bipolar Disorders, 16(3), 230-240. https://www.doi:10.1111/bdi.12159
We can write this or a similar paper for you! Simply fill the order form!
for this paper, the writer must pay attention to details. The writer should carefully read all instructions before attempting the assignment. The writer must clearly respond to all items listed in the questions while clearly following the template provided using proper APA as indicated. The writer must use the chosen topic and must also clearly show the chosen model as indicated in the paper.
Community Health Strategy
Advance practice nurses can be found in every aspect of the health care field including out in the community. Advanced practice nurses not only care for the client but all aspects that surround their clients. In this assignment you will focus on promoting the health of the community. You will choose a topic concerning women’s health. In a 5 to 6 page APA formatted paper you will create and discuss a community health promotion that pertains to your topic. Make sure to:
1. Identify your chosen topic and the demographic area and population that you are targeting. The chosen Topic is (Vulvovaginal infections and sexually transmitted infections). The demography area and population is the African-American population in the Washington DC Metro area.
2. Discuss why this topic is important to this group (include background information) with references.
3. Use one community based health promotion model.
4. Discuss how this model was used in the creation of this community health promotion strategy.
5. Include your community health promotion strategy.
Assignment Requirements
The finished Assignment should be 4 pages minimum Analytical essay, encompassing all required items listed. The viewpoint and purpose of this Assignment should be clearly established and sustained.
Before finalizing your work, you should:
• be sure to read the Assignment description carefully
• consult the Grading Rubric (under the Course Home) to make sure you have included everything necessary;
• utilize spelling and grammar check to minimize errors; and
• review APA formatting and citation information found in the KU Writing Center, online, or elsewhere in the course.
Your assignment should:
• follow the conventions of Standard American English (correct grammar, punctuation, etc.);
• be well ordered, logical, and unified, as well as original and insightful;
• display superior content, organization, style, and mechanics;
• use APA 6th edition format for organization, style, and crediting sources including:
• properly formatted header
• 12-point, double-spaced, Times New Roman font
• use of in-text citations
• title page and reference page
• use of headings (if applicable)
SAMPLE ANSWER
Community Health Strategy
The health of communities is the priority of nurse practitioners. Studying diseases among different populations and in varied regions improves the understanding of nurses, and therefore facilitates patient care. Other than attending patients directly, nurses require establishing strategies that would benefit their communities on health matters.
Studying a particular type of disease in a narrow population could lead to more effective community health strategies. With such type of a study, nurses can identify issues that could not have been determined through studies that are too general.
Population, Demographic Area and Disease Identification
The essay explores Sexually Transmitted Infections (STIs) among African Americans residing within Washington DC. The paper emphasizes on vaginal as well as vulvar infections.
Vulvovaginal Infections and Sexually Transmitted Infections
Among the commonest health hazards striking the female gender are the reproductive tract infections. Often, infections on either the vagina or the vulva lead to the inflammation of the respective organ. Women can acquire reproductive system infections either through sexual intercourse or other means. Common vaginal and vulva infections include those of protozoon, viral or bacterial origins.
Trichomoniasis, gonorrhea, HIV/AIDS, vaginosis, herpes, chlamydia infection, and syphilis are just but examples of highly prevalent Sexually Transmitted Infections (STIs). While some infectious agents limit their damaging effects to the reproductive system, some such as HIV/AIDS virus extend to other body systems. Different populations face unequal risks to most of the infections. Among the infections causing vaginal and vulvar inflammation are genital candidiasis, trichomoniasis as well as vaginosis (Moreira Mascarenhas, Sacramento Cunha Machado,Borges da Costa e Silva,FernandesWeyll Pimentel, Teixeira Ferreira,Silva Leoni, &Grassi, 2012, Pg. 1)
Prevalence of STIs among the African Americans in Washington
Brown, Sales, DiClemente, Salazar, Vanable, Carey, and Stanton (2012) reported that African Americans in general have a disproportionate exposure to STIs (Pg. 1491). Research indicates that among other STIs, chlamydia infection and gonorrhea are most prevalent, especially among female adolescents within the African American population (Brow et al., 2012, Pg. 1491). With Chlamydia, for example, Center for Disease Control and Prevention (CDC) found from research that cases of the disease are six times higher in black women than they are in their white counterparts. For the males, as CDC further indicated, occurrence of chlamydia was nine times higher in the blacks as compared to the whites (2012).
The Importance of Studying Vulvovaginal Infections and Sexually Transmitted Infections among Black Americans in Washington DC
So many factors necessitate the study of STIs among African Americans. Investigations are not only important for the African Americans in Washington, but also for those in America at large.
Background information
Black Americans constitute 4% of the population in Washington DC (United States Census Bureau, 2015). Owing to their high predisposition to STIs, African Americans are worth special attention. Again, the varied nature of STIs calls for effective interventions.
Considering their numbers, African Americans are among the minority groups, both in Washington DC and in the US at large. In most cases, minority groups encounter hardships while accessing certain services in the community. As such, the minoritiesgroups end up receiving care of lower value than that enjoyed by the majorities.Financial strains and other barriers among populations limit their access to health care services.Nijhawan, Chapin, Salloway, Champion, Roberts and Clark (2012) wrote that for trichomoniasis, for example, lack of quality gynecological care accounts for high number of cases among minority populations (Pg. 3).
African Americans Face High Risk to a Variety of STIs
A number of findings indicate disproportionality in the predisposition of African Americans to STIs. Swartzendruber, Sales, Brown, DiClemente and Rose for instance, indicated that women within the group face higher risk for both HIV/AIDS and trichomonasvaginalis (2014, Pg. 240). Other infections to which African Americans depict higher predisposition than normal include gonorrhea, chlamydia and syphilis (CDC, 2012). Owing to the facts and the current research findings established, it is important to study STIs among African Americans.
Community Based Health Promotional Model
To fight STIs among African Americans, one of the most applicable strategies include the Community Organization Model of Health Promotion.
Concepts of the Community Organization model
In the model, healthcare practitioners take a central position toward promotion of health in the community. To implement measures, healthcare workers rely on the community for support and material resources (US department of Health and Human Services, 2011, Pg. 8). With the method, healthcare practitioners cooperate with social organizations such as learning institutions and religious groups to pursue the common goal of health promotion (US Department of Health and Human Services, 2011, Pg. 8).
Advantages of Using the Community Organization Model
The Community Organization Model allows nurses to associate with the society. Through the model, nurses and other healthcare professionals can help the community in identifying problems within their environment. For instance, nurses can sensitize African Americans on their high predisposition to sexual illnesses. After understanding their situation, people within the population would take more precautions to protect themselves. The community would also get involved for the promotion of their own health. It would be easier solving the menace with optimal involvement of the affected population.
How Community Organization Model was used in the Creation of Health Promotion Strategy
The community organization model motivated the strategy that aimed at promoting the health of African Americans.
The Activities Involved
Community assessment was performed, and it was established that there was need for the study of vulvovaginal infections, as well as STIs among African Americans. The model also motivated the involvement of clinicians in addressing the situation. Usually, community organization model requires cooperation between the members of the society and healthcare practitioners (U.S Department of Health and Human Services, 2011, Pg. 9).
The Expected Outcomes after the Application of the Model
Since the model connected clinical care providers to the community, the health of African Americans was expected to improve. The clinicians would offer necessary information to the community on matters concerning their sexual health. Interaction between involved parties would facilitate the move toward a healthier society.
Improvement of Sexual Health among African Americans as aCommunity Health Promotion Strategy
Sexual behavior was found to be an essential element in the high occurrence of STIs among African Americans (Brown et al., 2012, Pg. 1493). The public therefore, need knowledge on safe methods of participating in sexual activities. Again, education on practices that would reduce infection through non-sexual practices is necessary. Employing an educative strategy would help in community health promotion. Nurses can offer the education needed by the community.
Conclusion
Following the raised risk for STIs among African Americans, relevant bodies need to work tirelessly to promote the health of the population. Stakeholders need to employ effective strategies that would offer the best outcomes. When addressing a health issue affecting an entire population, methodologies applied need to take a communal approach, rather than focusing on singular patients. To reduce the susceptibility of African Americans to vulvovaginal infections and STIs, clinicians and other health advisory groups need educating the population. They should sensitize the community on its high susceptibility to the infections, in addition to offering it the protective measures.
References
Brown, J. L., Sales, J. M., DiClemente, R. J., Salazar, L. F., Vanable, P. A., Carey, M. P., … Stanton, B. (2012). Predicting Discordance between Self-reports of Sexual Behavior and Incident Sexually Transmitted Infections with African American Female Adolescents: Results from a 4-city Study. AIDS and Behavior, 16(6), 1491–1500.
Moreira Mascarenhas, R. E., Sacramento Cunha Machado, M., Borges da Costa e Silva, B. F., FernandesWeyll Pimentel, R., Teixeira Ferreira, T., Silva Leoni, F. M., &Grassi, M. F. R. (2012). Prevalence and Risk Factors for Bacterial Vaginosis and Other Vulvovaginitis in a Population of Sexually Active Adolescents from Salvador, Bahia, Brazil. Infectious Diseases in Obstetrics and Gynecology, 2012, 1-6.
Nijhawan, A. E., Chapin, K. C., Salloway, R., Andrea, S., Champion, J., Roberts, M., & Clarke, J. G. (2012). Prevalence and Predictors of Trichomonas Infection in Newly Incarcerated Women. Sexually Transmitted Diseases, 39(12), 1-14.
Swartzendruber, A., Sales, J. M., Brown, J. L., DiClemente, R. J., & Rose, E. S. (2014). Correlates of Incident Trichomonasvaginalis Infections Among African American Female Adolescents. Sexually Transmitted Diseases, 41(4), 240–245.
U.S Department of Health and Human Services. (2011). Community Health Workers Evidence-Based Models Toolbox HRSA Office of Rural Health Policy. Retrieved June 7, 2015 from http://www.hrsa.gov/ruralhealth/pdf/chwtoolkit.pdf
Understanding people and the health care environment
Understanding people and the health care environment
Order Instructions:
Discuss the factors contributing to the breakdown between health care providers and patients from a culturally and linguistically diverse background, therefore, discuss influence of culture on communication & access to health care services and what are some of the communication barriers to accessing health with patients from a different cultural background (focus on refugees in Australia).
Explore the impact of people’s ( immigrants/refugees/culturally diverse people) ) engagement with health care services.
SAMPLE ANSWER
Understanding people and the health care environment
It is hypothesized that language barrier is an independent variable; which is responsible for poor access to quality healthcare by Australian Refugees. Several surveys indicate that the quality of care correlates with the nature of the relationship between the healthcare provider and the patient. According to Refugee statistics in 2014, there are about 11.7million refuges being hosted in developed countries; 0.3% of them are hosted in Australia. Additionally, over the last decades, there has been increased in population of the foreign-born. This rapid growth of refugee has increased healthcare disparities associated with the language barrier and cultural diversity in Australia (Clarke et al. 2014).
In this context, culture refers to a pattern of human being behavior; beliefs, practices, values and other customs. Cultural values and beliefs affect healthcare in many ways. First, culture affects people’s way of seeking care. Some cultures have different beliefs on disease etiology which influences the decision making processes; especially when choosing the preferred type of therapy. Additionally, cultural familiarity with healthcare systems could influence acceptability of modern care. Cultural aspects, influence people’s way of life such as adapting to health-related knowledge or lifestyle; in some cases, it influences the relationship and interaction with the healthcare provider (Artuso et al. 2013)
Culture has many systems; one aspect of systems includes communication and language. There is a partial overlap between culture and language. For example, refugees who speak French can be from different parts of the world with distinct culture. Therefore, there is diversity within the similar language-speaking community; and beyond the broad statistical grouping (Hiruy & Mwanri 2013). The healthcare conventional model depicts a strong relationship between several independent variables which influence the ability to access healthcare facility; and to utilize the resources; these variables include predisposing characteristics such as age; sex, and ethnicity (Davies et al. 2014).
The issues of language barriers are also independent variables which have been identified to have an effect on healthcare. The language barrier makes people have difficulty in expressing their signs and symptoms; have difficulty in understanding the foreign medical terminology or even follow the necessary instructions towards accessing care (Al Abed et al. 2014). For example, it has been found that non-speaking women are less likely to receive mammogram or Pap smear test. The research study also found that the nonspeaking community lack regular primary care; which is associated with a reduced quality of life. The language barrier is associated with lack of access to healthcare; and is often associated with reduced access to transport and medical insurance (Mahmoud et al. 2012).
Language and cultural components are often used interchangeably, such that impacts of culture are often indistinguishable with those of culture. However, proficiency in language does not necessarily imply that a person understands its cultural values and beliefs. For instance, a person born in one continent could choose to learn a different language from a dissimilar continent (Clarke et al. 2014). Though the person may be fluent in speaking and understanding foreign language, he or she may not understand health values and beliefs, alternative health remedies and existing rituals. In this context, learning foreign language only improves patient-doctor communication; but, it would not overcome the prevailing cultural differences and influences to healthcare systems (Cheng, Drillich & Schattner 2015).
The language barrier causes many individuals to be unfamiliar with health care systems in Australia. This often results to misunderstandings between healthcare providers and service users. This makes the service users experience that the health system is crisis oriented; making it difficult for the patient to understand processes in preventive care and schedule appointment. The recent study on asylum seeking refugees indicated that they did not understand why they would not receive treatment when they went to hospitals without appointment. Others had different interpretation and perception of emergency, and would show up in the emergency department even with no emergency condition (Al Abed et al. 2014).
The language barrier also affects the quality of care to service user as well as patient satisfaction. The language barrier result to medical errors which put patient safety in danger. Studies done indicated that medical error incidences were more common when service user and service providers spoke different languages. The language barrier could result to in accurate recording of the patient’s medical history, poor communication could also lead to erroneous prognosis or misdiagnoses. Additionally, language barriers could make patients fail to follow medical instructions, overtreatment of patients and interfere with medical adherence (Zhang et al. 2015).
The language barrier and cultural barriers influence people’s healthcare literacy. Health literacy refers to the people’s ability to gather knowledge; process and comprehend the basic healthcare and social care information. Health literacy is a component of effective communication and is affiliated with the language barrier (Al Abed et al. 2014). Health literacy is inversely associated with education attainment and socioeconomic background. However, there is need to carry out more research to establish the exact relationship between the language barrier, cultural barriers and servicer user and provider relationship and on specific healthcare outcomes. The research should look into the role of English /language proficiency, cultural diversity on health literacy; and how it impacts the patient’s outcome (Clarke et al. 2014).
References
Al Abed, N., Hickman, L., Jackson, D., Digiacomo, M. and Davidson, P. (2014). Editorial. Contemporary Nurse, 46(2), pp.259-262.
Artuso, S., Cargo, M., Brown, A. and Daniel, M. (2013). Factors influencing health care utilization among Aboriginal cardiac patients in central Australia: a qualitative study. BMC Health Services Research, 13(1), p.83.
Cheng, I., Drillich, A. and Schattner, P. (2015). Refugee experiences of general practice in countries of resettlement: a literature review. British Journal of General Practice, 65(632), pp.e171-e176.
Clark, A., Gilbert, A., Rao, D. and Kerr, L. (2014). Excuse me; do any of you ladies speak English? Perspectives of refugee women living in South Australia: barriers to accessing primary health care and achieving the Quality Use of Medicines. Australian Journal of Primary Health, 20(1), p.92.
Davies, J., Bukulatjpi, S., Sharma, S., Davis, J. and Johnston, V. (2014). Only your blood can tell the story€ – a qualitative research study using semi- structured interviews to explore the hepatitis B related knowledge, perceptions and experiences of remote dwelling Indigenous Australians and their health care providers in northern Australia. BMC Public Health, 14(1), p.1233.
Hiruy, K. and Mwanri, L. (2013). End-of-life experiences and expectations of Africans in Australia: Cultural implications for palliative and hospice care. Nursing Ethics, 21(2), pp.187-197.
Mahmoud, I., Hou, X., Chu, K. and Clark, M. (2012). Language and utilisation of emergency care in Queensland. Emerg Med Australas, 25(1), pp.40-45.
This essay explores diabetes as a highly prevalent disease among Indian seniors. Diabetes mellitus is usually more common than insipidus and the essay emphasizes on the former. Two subtypes of diabetes mellitus earn most attention in the study. They are diabetes type 1 and diabetes type 2, also referred to as insulin-dependent and insulin-independent respectively (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 524). In Indian population, diabetes type 2 is more common and severer than type 1.With the characteristic change of livelihood in the recent years, the old in India get higher risk to diabetes than in the earlier days. Some primary care measures in the management of the situation are in place, and there is prospective to better the practice.
Epidemiological Background of Diabetes in India
Diabetes has affected a large population in India, and it still remains a major health issue. The disease accounts for a large percentage of deaths in the country especially among the aged. Currently, 62 million Indians have the condition according to research (Kaveeshwar & Cornwall, 2014, Pg. 45). Studies indicate India as among the nations most affected by diabetes. In 2000, investigations indicated the country as the most hit by diabetes. While India had a diabetic population of 31.7 million, America, the second placed had 20.8 million. China was third with 17.7 million people being diabetic (Kaveeshwar & Cornwall, 2014, Pg. 45). There is likelihood that when global diabetic population increases, India will have contributed the largest population. Factors predisposing Indians to diabetes are many and the situation creates uncertainties for the nation regarding the issue. Though some factors are easily identifiable, others are complicated and stakeholders in healthcare face the challenge of understanding them. Issues that hinder researchers from understanding risk factors include the population’s heterogeneity in relation to ethnicity, culture and socioeconomics (Kaveeshwar & Cornwall, 2014, Pg. 46). Factors currently identified include genetics and the Indian environment. As an environmental factor, livelihood in India predisposes people to obesity, which in turn makes them prone to diabetes.Regional variations are also identified as risk determinants, whereby Indians in rural areas are less exposed to diabetes than their counterparts in towns. The Indian Council of Medical Research (ICMR) found that Maharashtra and Tamil regions have higher statistics of affected people than Chandigarh and Jharkhand, which are to the north of the state (Kaveeshwar & Cornwall, 2014, Pg. 46). Such disparities are also common in other countries such as Australia (Sukala, Page, Rowlands, Lys, Krebs, Leikis, & Cheema, 2012, Pg. 432). Research is yet to prove whether the fact of most people in northern India being migrants while those in south are host could influence the variations. Geographical locations in India also influence diabetes management as access to screening and necessary medication is limited in the rural areas. People who suffer from diabetes in poor regions are more likely to die of the same compared to those in developed regions. In impoverished regions, there is higher likelihood of inadequacy of education offered to people. The aged, for example, may not access education on preventive practices and could face greater risk of diabetes than their educated counterparts (Khalil, Tan, & George, 2012, Pg. 577). The prevalence of diabetes in India is peculiar in that the population is not as much exposed to obesity like in some western countries, yet it records higher cases of diabetes than them. Obesity is not more common in India than these countries, yet it is usually the lead causal factor (Rao, Kamath, Shetty & Kamath, 2011, Pg. 54). In the recent, diabetic complications have increased among the older Indians. A large diabetic population in India expresses inability to control blood sugar level, and ends up developing abnormalities in their vascular structures.
Challenges in the management of diabetes in India include unavailability of HbA1c tests to most Indians (Kumar, 2010, Pg. 128). Insulin therapies are also hard to administer following decreased clinical activeness. Indian guidelines also fail to sufficiently address issues with insulin use therefore making it hard to practice the clinical role (Unnikrishnan, Anjana, & Mohan, 2011, Pg. 10). Managing the current status of diabetes in India requires efforts from the, government as well as other involved parties (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 530). The Indian government has made efforts toward the control the illness. Efforts by the government include the establishment of National Diabetes Control Program (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 524). Healthcare practitioners require helping the population with strategies that address early detection, prevention, and management of diabetes (Kaveeshwar & Cornwall, 2014, Pg. 47). Generally, issues addressed on management of diabetes in India include increasing access to services, increasing the affordability of medicines, improving service quality as well as conducting more studies to develop helpful initiatives (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 525).
Social Determinants in the Management of Diabetes in India
Management of diabetes is subject to several social factors. Stakeholders need to pay attention to such factors in their strategies to improve outcomes in diabetic patients. There is the necessity of research to test outcomes based on social determinants. To curb the increased prevalence of diabetes in India, such research studies are mandatory. Social factors also entail environmental issues, in addition to cultural ones. Diabetes is prevalent among the poor, middle-earning as well as rich populations. India is generally a middle-earning country, and diabetes is more prevalent among the poorer people. Environmental influences in diabetes include feeding habits and physical activities. Intake of food that is highly calorific has increased among Indians causing development of obesity and hence diabetes. Measures in diabetes management include monitoring of one’s diet to lower the risk of taking too much fats and sugar. Asif wrote that people aim at maintaining the safest concentration of sugar and lipids in blood (2014). Health professionals advocate for increased uptake of fruits, whole grains, vegetables, low-fat dairy products and food high in unsaturated fats (Asif, 2014). On the other hand, diabetes management requires reduced intake of red meat, legumes, fish and nuts (Asif, 2014).The International Expert Committee provided dietary guidelines for management of diabetes. In the guidelines, experts advise patients to take carbohydrates as starch. While patients should avoid refined sugars, they may take non-nutritive sweeteners. In addition, people should avoid animal fats, salt, and tobacco smoking (2009, Pg. 1328). Again, failure to engage in physical strains as is the common situation with advanced technology, places people at the risk of diabetes. Given that India has realized substantial developments in technology, the aged in the country are unlikely to take manual activities. For instance, the old would prefer driving to walking even when covering short distances. Failure to exercise leads to too much fat deposits in the body and individuals are likely to become obese. Since the old have machines at their disposal, management of diabetes could be difficult as it requires them to forego machines for manual actions. As a measure to manage diabetes, care providers educate patients on matters relating to the disease. As Larranaga, Docet and Garcia-Mayor wrote, teams concerned with the management of diabetes should monitor insulin regimens, while still educating patients (2011, Pg. 190). Psychosocial approaches are also important in the management of diabetes in India. Kalra, Sridhar, Balhara, Sahay, Bantwal, Baruah, and Kumar addressed psychosocial influences in diabetes management. The researchers indicated that optimal outcome in managing the disease entails physical, social as well as psychological fitness (2013, Pg. 380). Psychological status, particularly, affect administration of self-care in diabetic patients. Kalra et al. noted that psychological factors affecting patients in India differ significantly from those associated with patients elsewhere (2013, Pg. 380). Economic factors are also crucial in the management of diabetes. A significant part of the Indian population is poor, and may not meet the financial costs of insulin treatment. In addition, culture and religion as social practices determine the level of diabetes management. Generally, these practices interact with healthcare provision, hence influencing it. Some attitudes developed with culture, combined with illiteracy may hinder care for diabetic patients. Some uneducated people are unlikely to understand the complexity of issues associated with diabetes management. Use of traditional medicine, a relatively common practice in India, also influences diabetes management from a societal perspective. 14% of Indians use herbal medication and some people in the population may not readily accept convectional medicine that most care providers offer (Kalra, et al. 2013, Pg. 379).
Primary Healthcare Delivery in the Management of Diabetes among the Aged in India
Milat, O’hara and Develin explained that primary care usually focuses on disease prevention (2009, Pg. 87). As such, campaigns characterize the type of care. If properly conducted, primary care can reduce the occurrence of diabetes. In people who are already diagnosed with the disease, elderly Indians for this case, primary care aims at attaining a normal concentration of sugar in their blood. (Ramachandran, Das, Joshi, Yajnik, Shah, & Kumar, 2010, Pg. 8). There is need for clinicians to offer quality care to patients as complications of diabetes could result into other life-threatening illnesses. Ramachandran et al. noted hat more than half of diabetic patients in India possess poor ability to control their blood sugar, and their vascular structures have abnormalities (2010, Pg. 8). Clinicians also require awareness on high standards of care especially with newly developed therapeutic agents. United Kingdom Prospective Diabetes Study (UKPDS) offered recommendations that 53% of diabetes patients receive insulin therapy for six years, while 75% should take more than one treatment strategies for approximately nine years. When offering primary care, practitioners should understand that too much insulin could induce obesity, worsening the situations of patients resistant to it (Ramachandran et al., 2010, Pg. 8). In primary care, clinicians can attend large populations of patients and establish follow-ups. When attending aged people with diabetes, practitioners in India should establish links with their patients to facilitate the process of care delivery. Nurses should lead in implementation of strategies that educate patients on diabetes. In addition, primary care providers need to be optimistic, and encourage their patients to increase their chances of recovery. Though diabetes is a chronic disease, patients can still lead an enjoyable lifestyle if they receive high quality primary care. Since nurses have intensive expertise in counseling, they assume the most effective position in primary care for diabetic patients. In addition to offering primary care, nurses should develop strategies to improve their services to patients. Nurses require being creative and initiative as professional virtues. When combined with their caring character, the two traits would enable nurses make essential transformations in diabetes management.It is also advisable that since the occurrence of diabetes varies with genetics, culture, social practices and geographical locations, nurses and other practitioners should be sensitive of the variations. Generally, primary care should see to it that preventive measures are fully exploited just as the ones addressing diabetes treatment. In primary care for instance, clinicians should encourage patients to engage into healthy livelihood. Dietary and exercise intervention are essential at the primary level of care for old people with diabetes. Other parties involved in primary care for diabetic patients include dieticians, pharmacists, physicians and psychologists. Professionals from various fields should cooperate to facilitate primary care. Team work as seen in interdisciplinary teams could offer the best outcomes in diabetes management. Patient care is often complex but can be promoted if stakeholders associate appropriately. Practitioners should ensure that the care they offer is patient-centered, and that it constitutes healthy communications with patients, partnerships and focuses beyond the situation at hand. Practitioners require explaining essential concepts of the disease to patients. In addition, they should be able to assess the feelings, expectations as well as beliefs of their patients. Generally, care providers need developing common grounds with their patients. When primary care is patient centered, there are higher chances that satisfaction will be obtained for both the providers and receivers of services.
Future Healthcare Directions in the Management of Diabetes among the Aged in India
Currently, the occurrence of diabetes among the aged in India is alarming. There should be long-term strategies to help overcome the situation. There are, therefore, rapid changes in the management of diabetes as approaches are unlimited (Universit5y of Melbourne, 2011). Researches are carrying out studies to develop better means of addressing diabetes among all populations. For instance, there are moves to develop new drugs that can be more effective than the current regimens. Ramachandran et al. explored possible drugs that may help fight diabetes in the future. The researchers indicated that analogues of glucagon as well as those of dipeptidyl peptidase-4 could offer better therapeutic agents in the future (2010, Pg. 8). Researchers are carrying out clinical studies on new drugs and in the near future, there could be drugs that would change the common regimens applied for diabetes. Drugs in advanced developmental stages include DPP-4 inhibitors, which include vidagliptin and sitagliptin (Ramachandran et al., 2010, Pg. 8). As Ramachandran et al. expressed, the two drugs improve the sensitivity of beta cells to insulin, and could be useful for diabetes mellitus type 2 (2010, Pg. 8). Measures that address livelihood seem to offer the best approach on management of diabetes. Dietary modifications and engagement in exercise can lead to high performance in minimization of diabetes cases in India, especially among old people. Oral drugs, which currently are the most used in diabetes, may not be the first-line choices as times goes by. Better means of managing diabetes will be developed to ease the burden of having to take medications on daily basis.Drugs that would be more preferred in the future, should not only manage diabetes, but also its comorbidities. Again, their use should guarantee optimal safety while still being effective. Since insulin is the central hormone in diabetes, researchers are likely to develop its receptor agonists as therapeutic agents (Sanofi Diabetes, 2012). There are also moves to develop long-acting drug compounds that would have great effect in management of diabetes.Usually, challenges with the current diabetes therapies necessitate the development of new therapies.
Conclusion
India has the highest cases of diabetes mellitus in the world. Diabetes mellitus is more prevalent among the old than it is with the young. Indian population faces several risk factors that predispose them to the disease. These factors include genetics as well as social and cultural factors. Social practices and cultural beliefs often influence health care provision. In most cases, cultural beliefs work against care provision for the aged diabetic patients in India. To address the high occurrence of diabetes in India, clinicians and the government take a central position. It is upon clinicians to ensure that they offer quality care to diabetic patients in the move to manage the disease.
References
Asif, M. (2014). The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. Journal of Education and Health Promotion, 3, 1. doi:10.4103/2277-9531.127541
Kalra, S., Sridhar, G. R., Balhara, Y. P. S., Sahay, R. K., Bantwal, G., Baruah, M. P., … Prasanna Kumar, K. M. (2013). National recommendations: Psychosocial management of diabetes in India. Indian Journal of Endocrinology and Metabolism, 17(3), 376–395. doi:10.4103/2230-8210.111608
Kaveeshwar, S. A., & Cornwall, J. (2014). The current state of diabetes mellitus in India. The Australasian Medical Journal, 7(1), 45–48. doi:10.4066/AMJ.2013.1979
Khalil, H., Tan, A., & George, J. (2012). Diabetes management in Australian rural aged care facilities: A cross-sectional audit. Australas Med J, 5(11), 575–80
Kumar, A., Goel, M. K., Jain, R. B., Khanna, P., & Chaudhary, V. (2013). India towards diabetes control: Key issues. Australas Med J, 6(10), 524–531.
Larrañaga, A., Docet, M. F., & García-Mayor, R. V. (2011). Disordered eating behaviors in type 1 diabetic patients. World Journal of Diabetes, 2(11), 189–195. doi:10.4239/wjd.v2.i11.189
Mkilat, A. J., O’Hara, B., & Develin, E. (2009). Concepts and new frontiers for development – What role should health promoters play in lifestyle-based diabetes prevention programs in Australia? Health Promotion Journal of Australia, 20(2), 86-94
Ramachandran, A., Das, A. K., Joshi, S. R., Yajnik, C. S., Shah, S., & Kumar, K. M. (2010). Current Status of Diabetes in India: Need for Novel Therapeutic Agents. JAPI, 58, 7-10
Rao, C. R., Kamath, V. G., Shetty, A., Kamath, A. (2011). A cross-sectional analysis of obesity among a rural population in coastal southern Karnataka, India. Australas Med J, 4(1), 53–57.
Sukala, W. R., Page, R. A., Rowlands, D. S., Lys, I., Krebs, J. D., Leikis, M. J., & Cheema, B. S. (2012). Exercise intervention in New Zealand Polynesian peoples with type 2 diabetes: Cultural considerations and clinical trial recommendations. Australas Med J,5(8), 429–35
The International Expert Committee. (2009). International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care, 32, 1327–34
Unnikrishnan, R. I., Anjana, R. M., &Mohan, V. (2011). Importance of Controlling Diabetes Early–The Concept of Metabolic Memory, Legacy Effect and the Case for Early Insulinisation. JAPI, 50, 8–12.
We can write this or a similar paper for you! Simply fill the order form!
An advance care plan is a structured and ongoing communication or discussion between a patient and a professional health caregiver which is meant to communicate the future wishes of the patient in matters concerning treatment and care options should they not be able to communicate these wishes at that particular time. (Oliver, 2013, pg 135) The discussion might also involve a third party such as the patients close family member. Mr. Mario who lives with his wife, Rosa, is a 46 year old man with stage 4 pancreatic cancer who has just been told by his oncologist that the chemotherapy treatment he was receiving is no longer effective. Over the past few days, Mr. Mario has been experiencing symptoms such as nausea. The following is an essay concerning Mr. Mario’s advance care plan.
Initiating the conversation on advanced care planning
This conversation is meant to discuss with a patient the method and means he would like to be treated or taken care with once he or she falls seriously ill and he is not able to make such decisions then. Usually, this conversation is started when it is clear that a patient’s health risk is very high and so is the case with Mario. The conversation on advanced care planning with Mario should have been initiated after being told by the oncologist that the chemotherapy was unlikely to be ineffective and that is the same period when he decided that he would focus on the time he has with his family. During the initiating of the conversation, it is important to explain to Mr. Mario what the conversation is all about and the importance. It is after this that he should then be asked if there is anyone who he thinks should be present during the conversation. This should then be followed by the deliberate allowing of time so as to provide the patient with an opportunity to reflect. (Yeung, Escalante & Gagel, 2009, pg.46)
After that, the conversation can then begin and this must be done by using words not too insensitive to the patient for example, ‘I would like to discuss with you about your wishes of future care in case you get very sick which might not happen but just in case it does you will not be able to express your wishes and at that point it would be very important to know what you would have wanted’, ‘Have you considered about the place or type of care you would want to have in case you became too sick to take care of yourself?’ or ‘most people usually think about what they may want in the future and they usually have their wishes drafted in a document called Advance Health Directive. Would you like to know more about this Advance Health Directive?’
Preparing for the conversation
There are some very important issues that should be taken into consideration in preparation of the advance care planning discussion and this is mostly so as to protect and maintain the welfare of the patient and this are as follows
Firstly, one should review all medical files notes or files of the patient. This is meant to ensure that all that all the relevant and critical clinical information concerning the patient are available. The same can still be achieved through consulting other medical care experts involved with the patient. (Goldstein & Morrison, 2013, pg 273)
Secondly, the health care professional should also ensure that he or she has a private and comfortable area to carry out the discussion. This area should be free from interruptions from anyone. This will help in boosting concentration while collecting all the necessary information. In addition to finding a private area, one should determine if there is a family member who can participate in the discussion. This family member should be a very close family member. This can be determined through scrutinizing the patients’ health and personal documents.
Moreover, it should be made sure that the patient is in a mental capacity to participate in the discussion. This is so because the patient, if not in the capacity to discuss these matters, can easily fall into a depression. If there is a family member participating in the discussion, the same should also be made sure to avoid any cases of afterwards depression. Chambers, Germain & Brown, 2010, pg55)
One should ensure that he or she has drafted a structure that will be used during the advanced care planning process. This can be achieved for example, through having a structure that contains leading question. The draft structure should be able to contain the following components;
it should lead one in identifying the goals, advantages and disadvantages of the methods and interventions that the patient would want sought
it should be able to ensure that the patient knows the level of seriousness of his stage four pancreatic cancer.
It should be able to lead the patient in knowing that his disease is palliative.
It should also be able to identify the patient’s fears or greatest concerns.
It should be able to determine what the patient thinks about the advance care planning.
One should have an understanding and be well conversant with all local laws that concern the drafting and implementation of such critical documentation. One should also ensure that he or she has adequate knowledge on how to access the necessary documents.
Lastly, arrangements for the appropriate support services should be made prior to the initiating of the conversation. Among other things, this support service can be helpful in consoling the patient if he or she gets emotional during the conversation and breaks down.
Who should be involved in the discussion?
An advanced care planning discussion usually involves a patient and it also advisable for very close family member to be present although the consent of the patient will have to be sought first. In the case of Mr. Mario, his close family member is his wife Rosa, so it would be appropriate to involve his wife in the discussion. Both the participants will be required to participate in the discussion through sharing their opinions concerning the advance care plan. Mr. Mario could also choose for his attorney to be present especially if he is interested in transferring his power of attorney to a different person such as Rosa who would be required by the power of attorney to make decisions for his husband when the husband is not in a capacity to do so. Whatever is discussed in the advance care plan is then documented which will make it easy to use for future references. The wishes are then legalized through filling out legal forms entailing all your wishes. This can be done with the help of an attorney although it is not necessary. (Noogle, 2012, pg 57)
Information to be included in the advance care plan
There are issues that should be included in an advance care plan. For an effective outcome, this should mostly be in the form of questions. The issues to be addressed should be as follows;
Firstly, there should be goals, advantages and disadvantages of any interventions that might be required when taking care of the patient. These goals may include decisions of emergency treatments to keep the patient alive such cardiopulmonary resuscitation (CPR) which is meant to restore the heartbeat if it stops, comfort care which involves relieving pain, artificial nutrition or artificial hydration which are meant to provide nutrition to the patient through a tube when the patient is unable eat or drink. This is meant to ensure that Mr. Mario fully understands the consequences of any method before preferring for it to be used in the advance care plan. (Thomas & Lobo, 2011, pg 239)
Secondly, the plan should be able to address the patients preferred place for receiving future care and this is meant to ensure that the patient is comfortable in receiving this care for example; this could be asked as ‘where would you prefer to receive future care?’
Although not necessary, the patient should be given the opportunity to decide whether he would like to donate any organ or tissue in case of death and the question asked could be; ‘incase of death, would you like to donate any of your body organ or tissue? If so where or to whom would you want the above stated organ or tissue donated?’ (Vadivelu, Kaye & Berger, 2013, pg 100).
The advance care plan should be able to make sure that the patient and his wife are aware of the extent of seriousness and risk of his pancreatic cancer. This is one of the means of ensuring that the participants are in the right mental capacity to get involved in the discussion. For example, this could be asked in the form; ‘are you aware of the extent of risk of your level four pancreatic cancer? If so what do you think are the risks involved?’
The care plan should be able to inquire from the patient the people he would like to make decisions for them in case they are unable to make these decisions. The care plan should still be able to inquire if the patient has shared his wishes with his family or friends. This could be in the form; ‘Incase your are not able to make any decision, whom would you like to act in your capacity in making these decisions? Apart from your wife, have you informed any other family member or friend of your wishes?’
The plan should be able to diagnose Mr. Mario’s gravest and deepest fears concerning his pancreatic cancer. The same should also be inquired from his wife, Rosa. For example this could be asked as ‘what are your deepest fears concerning this disease?’
Lastly, the advance care plan should give Mr. Mario or his wife the opportunity to ask any question related to Mr. Mario’s health that might have not been addressed in the care plan. This could be asked as ‘Is there any other issue concerning the disease that you would want addressed here?’
Reviewing of the advance care plan
This involves the revisiting of the advance care plan discussions and at times the decisions set out in the advance care plan can be changed. It is usually advisable for the reviewing to be done regularly due to a number of reasons which can apply in Mr. Mario’s case. The following are the main reasons for reviewing the plan or circumstances that might trigger the reviewing process
Firstly, Mr. Mario or his wife could request for the reviewing or change their mind about a decision that they had made earlier this might for example, be triggered by the infeasibility of an option that they had recommended maybe due financial constraints or a number of other issues.
Secondly, there could be a change in circumstances that might require the reviewing of the plan. For example, change in medical conditions whereby a new disease or condition is discovered in the patient. The same could also be triggered by change of individual conditions for example incase Rosa, Mr. Mario’s wife, dies or any other person mentioned in the advance care plan and whose death affects the plan.
Thirdly, the reviewing can be done when Mr. Mario returns to the hospital for example when he is going back for a checkup or when the health care professional visits Mr. Mario at his home. Usually, the reviewing of the plans is usually set to be done constantly and in such cases the reviewing is done when the patient visits the hospital or when the health care professional visits the patient at home. (Hartmann, Loprinzi & Mayo Clinic, 2012, pg 45)
Fourthly, the reviewing can be done if the medical options that are present in the advanced care plan changes the needs of Mr. Mario in regards to the plan for example in the discovering of a co morbidity.
Fifthly, Mr. Mario can revoke the advance care plan any time and this will require the preparation of a new advance care plan. In such a scenario Mr. Mario might view the earlier on plan as not been appropriate due to a number of reasons and this will require him to revoke the care plan and request for the drafting of a new one.
Lastly, during the making of the advance care plan, Mr. Mario can state a review interval of which after the interval time lapses, the making of a new advance care plan will be required. For example, Mr. Mario could state that he would require reviewing the care plan after every two months. After the lapse of these two months, Mr. Mario will then be required to review the care plan.
Activation of the advance care plan
This involves the point and time at which the discussion in the plan will be implemented. In Mr. Mario’s scenario this will take place under the following circumstances.
Firstly, activation can occur if Mr. Mario enters into a comma for example, after he collapses at the shopping centre and becomes non responsive and is taken to the hospital. If he completely fails to respond, then implementation of the care plan will be deemed necessary.
Secondly, the activation can occur in case of Mr. Mario deaths. In this case the advance care plan will be activated in that, if he had requested in the care plan for his body tissue or organ to be donated, then his wish will have to be fulfilled. (Barnsteiner, Disch, Walton & Sigma Theta Tau International, 2014, pg 107)
Thirdly, the activation maybe triggered by the person who has the power of attorney. This involves transferring your rights to make decisions concerning certain issues to another person who is required by law to make decisions that will be in your best personal interests if you are not in a capacity to make these decisions. In this case Mr. Mario could have given this power to his wife Rosa so if by any chance Rosa feels that Mr. Mario is not in a capacity to make decisions then she can ask for the implementation of the advance care plan.
Fourthly, the activation of the care plan can be triggered if Mr. Mario experiences dementia. This is a condition whereby the patient’s mental ability is impaired and cannot make decisions as a reasonable man. In such a case the patient will not be in the right mental capacity to make a reasonable decision so this will require the fulfilling of his wishes as he had earlier on stated in the care plan. (Leah & Susana 2013)
Lastly, the activation can be triggered by a medical condition which will make it impossible for Mr. Mario to communicate his decisions such as stroke or paralysis. In such a condition, the patient might be in good mental capacity to make decisions for himself but the communication of this decision might be difficult hence necessitating the use of his wishes as stated in the advance care plan
In conclusion, an advance care plan plays a very crucial role since it betters the quality of life of the patients, provides medical care which is less aggressive, helps families prepare for the death of a loved one and also helps in resolving family conflicts. (Thomas & Lobo, 2011, pg 78)
References
Oliver, D. (2013). End of life care in neurological disease. London: Springer
Yeung, S.-C. J., Escalante, C. P., & Gagel, R. F. (2009). Medical care of cancer patients. Shelton, Conn: People’s Medical Publishing House.
Goldstein, N. E., & Morrison, R.S. (2013). Evidence-based practice of palliative medicine. Philadelphia: Elsevier/Saunders.
Hartmann, L. C., Loprinzi, C. L., & Mayo Clinic. (2012). The Mayo Clinic breast cancer book. Intercourse, PA: Good Books.
Weis, J,. & Horneber, M. (2014). Cancer related fatigue
Noogle, C. A. (2012). Neuropsychology of cancer and oncology. New York: Springer Pub.
Chambers, E. J., Germain, M., & Brown, E. A. (2010). Supportivecare for the renal patient. Oxford: Oxford University press.
Fischer, S., Gozansky W., Sauaia A., Min S.,Kutner J., Kramer A. (2006). A practical tool to identify patients who may benefit from a palliative approach: the caring criteria Shrewsbury, UK: NHS 285
Thomas, K., & Lobo, B. (2011). Advance care planning in end of life care. Oxford: Oxford University Press.
In Vadivelu, N., In Kaye, A. D., & In Berger, J. M. (2013). Essentials of palliative care.
Melnyk , B. M., & Fineout-Overhault, E. (2011). Evidence based practice in nursing & healthcare: A guide to best practice. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
In Christensen, A. J., In Martin, R., & In Smyth, J. M. (2014). Encyclopedia of health psychology.
In LoBiondo-Wood, G., & In Haber, J. (2014). Nursing research: Methods and criticsl appraisal for evidence-based practice.
Barnsteiner, J. H., Disch, J.M., Walton, M. K., & Sigma Theta Tau International, (2014). Person and family centered care.
Leah, R., & Susana L. M. (2013). Advance care planning: communicating about matters of life and death. New York: Springer Pub.
We can write this or a similar paper for you! Simply fill the order form!
Your papers needs to highlight specific arguments and ideas in your choose of topic By highlighting these , you need to show the a) the epidemiological data b) the current literature in the field chosen .
Questions you should address
Asking questions such as the following will help you sift through your sources and organize your essay.
What’s been done in this topic area to date? What is the research and population based s, recent key trends ?
What are the gaps and / or weaknesses in the health services provided? Are there new/novel ways of at the issue?
The Marking Criteria for this Assignment
Present a synopsis of the epidemiological background over time ?
What are the key social determinates?
Critically examine the key aspects of primary health care delivery of this health issue
What might be the future healthcare directions?
SAMPLE ANSWER
Global Health
Introduction
This essay explores diabetes as a highly prevalent disease among Indian seniors. Diabetes mellitus is usually more common than insipidus and the essay emphasizes on the former. Two subtypes of diabetes mellitus earn most attention in the study. They are diabetes type 1 and diabetes type 2, also referred to as insulin-dependent and insulin-independent respectively (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 524). In Indian population, diabetes type 2 is more common and severer than type 1.With the characteristic change of livelihood in the recent years, the old in India get higher risk to diabetes than in the earlier days. Some primary care measures in the management of the situation are in place, and there is prospective to better the practice.
Epidemiological Background of Diabetes in India
Diabetes has affected a large population in India, and it still remains a major health issue. The disease accounts for a large percentage of deaths in the country especially among the aged. Currently, 62 million Indians have the condition according to research (Kaveeshwar & Cornwall, 2014, Pg. 45). Studies indicate India as among the nations most affected by diabetes. In 2000, investigations indicated the country as the most hit by diabetes. While India had a diabetic population of 31.7 million, America, the second placed had 20.8 million. China was third with 17.7 million people being diabetic (Kaveeshwar & Cornwall, 2014, Pg. 45). There is likelihood that when global diabetic population increases, India will have contributed the largest population. Factors predisposing Indians to diabetes are many and the situation creates uncertainties for the nation regarding the issue. Though some factors are easily identifiable, others are complicated and stakeholders in healthcare face the challenge of understanding them. Issues that hinder researchers from understanding risk factors include the population’s heterogeneity in relation to ethnicity, culture and socioeconomics (Kaveeshwar & Cornwall, 2014, Pg. 46). Factors currently identified include genetics and the Indian environment. As an environmental factor, livelihood in India predisposes people to obesity, which in turn makes them prone to diabetes.Regional variations are also identified as risk determinants, whereby Indians in rural areas are less exposed to diabetes than their counterparts in towns. The Indian Council of Medical Research (ICMR) found that Maharashtra and Tamil regions have higher statistics of affected people than Chandigarh and Jharkhand, which are to the north of the state (Kaveeshwar & Cornwall, 2014, Pg. 46). Such disparities are also common in other countries such as Australia (Sukala, Page, Rowlands, Lys, Krebs, Leikis, & Cheema, 2012, Pg. 432). Research is yet to prove whether the fact of most people in northern India being migrants while those in south are host could influence the variations. Geographical locations in India also influence diabetes management as access to screening and necessary medication is limited in the rural areas. People who suffer from diabetes in poor regions are more likely to die of the same compared to those in developed regions. In impoverished regions, there is higher likelihood of inadequacy of education offered to people. The aged, for example, may not access education on preventive practices and could face greater risk of diabetes than their educated counterparts (Khalil, Tan, & George, 2012, Pg. 577). The prevalence of diabetes in India is peculiar in that the population is not as much exposed to obesity like in some western countries, yet it records higher cases of diabetes than them. Obesity is not more common in India than these countries, yet it is usually the lead causal factor (Rao, Kamath, Shetty & Kamath, 2011, Pg. 54). In the recent, diabetic complications have increased among the older Indians. A large diabetic population in India expresses inability to control blood sugar level, and ends up developing abnormalities in their vascular structures.
Challenges in the management of diabetes in India include unavailability of HbA1c tests to most Indians (Kumar, 2010, Pg. 128). Insulin therapies are also hard to administer following decreased clinical activeness. Indian guidelines also fail to sufficiently address issues with insulin use therefore making it hard to practice the clinical role (Unnikrishnan, Anjana, & Mohan, 2011, Pg. 10). Managing the current status of diabetes in India requires efforts from the, government as well as other involved parties (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 530). The Indian government has made efforts toward the control the illness. Efforts by the government include the establishment of National Diabetes Control Program (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 524). Healthcare practitioners require helping the population with strategies that address early detection, prevention, and management of diabetes (Kaveeshwar & Cornwall, 2014, Pg. 47). Generally, issues addressed on management of diabetes in India include increasing access to services, increasing the affordability of medicines, improving service quality as well as conducting more studies to develop helpful initiatives (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 525).
Social Determinants in the Management of Diabetes in India
Management of diabetes is subject to several social factors. Stakeholders need to pay attention to such factors in their strategies to improve outcomes in diabetic patients. There is the necessity of research to test outcomes based on social determinants. To curb the increased prevalence of diabetes in India, such research studies are mandatory. Social factors also entail environmental issues, in addition to cultural ones. Diabetes is prevalent among the poor, middle-earning as well as rich populations. India is generally a middle-earning country, and diabetes is more prevalent among the poorer people. Environmental influences in diabetes include feeding habits and physical activities. Intake of food that is highly calorific has increased among Indians causing development of obesity and hence diabetes. Measures in diabetes management include monitoring of one’s diet to lower the risk of taking too much fats and sugar. Asif wrote that people aim at maintaining the safest concentration of sugar and lipids in blood (2014). Health professionals advocate for increased uptake of fruits, whole grains, vegetables, low-fat dairy products and food high in unsaturated fats (Asif, 2014). On the other hand, diabetes management requires reduced intake of red meat, legumes, fish and nuts (Asif, 2014).The International Expert Committee provided dietary guidelines for management of diabetes. In the guidelines, experts advise patients to take carbohydrates as starch. While patients should avoid refined sugars, they may take non-nutritive sweeteners. In addition, people should avoid animal fats, salt, and tobacco smoking (2009, Pg. 1328). Again, failure to engage in physical strains as is the common situation with advanced technology, places people at the risk of diabetes. Given that India has realized substantial developments in technology, the aged in the country are unlikely to take manual activities. For instance, the old would prefer driving to walking even when covering short distances. Failure to exercise leads to too much fat deposits in the body and individuals are likely to become obese. Since the old have machines at their disposal, management of diabetes could be difficult as it requires them to forego machines for manual actions. As a measure to manage diabetes, care providers educate patients on matters relating to the disease. As Larranaga, Docet and Garcia-Mayor wrote, teams concerned with the management of diabetes should monitor insulin regimens, while still educating patients (2011, Pg. 190). Psychosocial approaches are also important in the management of diabetes in India. Kalra, Sridhar, Balhara, Sahay, Bantwal, Baruah, and Kumar addressed psychosocial influences in diabetes management. The researchers indicated that optimal outcome in managing the disease entails physical, social as well as psychological fitness (2013, Pg. 380). Psychological status, particularly, affect administration of self-care in diabetic patients. Kalra et al. noted that psychological factors affecting patients in India differ significantly from those associated with patients elsewhere (2013, Pg. 380). Economic factors are also crucial in the management of diabetes. A significant part of the Indian population is poor, and may not meet the financial costs of insulin treatment. In addition, culture and religion as social practices determine the level of diabetes management. Generally, these practices interact with healthcare provision, hence influencing it. Some attitudes developed with culture, combined with illiteracy may hinder care for diabetic patients. Some uneducated people are unlikely to understand the complexity of issues associated with diabetes management. Use of traditional medicine, a relatively common practice in India, also influences diabetes management from a societal perspective. 14% of Indians use herbal medication and some people in the population may not readily accept convectional medicine that most care providers offer (Kalra, et al. 2013, Pg. 379).
Primary Healthcare Delivery in the Management of Diabetes among the Aged in India
Milat, O’hara and Develin explained that primary care usually focuses on disease prevention (2009, Pg. 87). As such, campaigns characterize the type of care. If properly conducted, primary care can reduce the occurrence of diabetes. In people who are already diagnosed with the disease, elderly Indians for this case, primary care aims at attaining a normal concentration of sugar in their blood. (Ramachandran, Das, Joshi, Yajnik, Shah, & Kumar, 2010, Pg. 8). There is need for clinicians to offer quality care to patients as complications of diabetes could result into other life-threatening illnesses. Ramachandran et al. noted hat more than half of diabetic patients in India possess poor ability to control their blood sugar, and their vascular structures have abnormalities (2010, Pg. 8). Clinicians also require awareness on high standards of care especially with newly developed therapeutic agents. United Kingdom Prospective Diabetes Study (UKPDS) offered recommendations that 53% of diabetes patients receive insulin therapy for six years, while 75% should take more than one treatment strategies for approximately nine years. When offering primary care, practitioners should understand that too much insulin could induce obesity, worsening the situations of patients resistant to it (Ramachandran et al., 2010, Pg. 8). In primary care, clinicians can attend large populations of patients and establish follow-ups. When attending aged people with diabetes, practitioners in India should establish links with their patients to facilitate the process of care delivery. Nurses should lead in implementation of strategies that educate patients on diabetes. In addition, primary care providers need to be optimistic, and encourage their patients to increase their chances of recovery. Though diabetes is a chronic disease, patients can still lead an enjoyable lifestyle if they receive high quality primary care. Since nurses have intensive expertise in counseling, they assume the most effective position in primary care for diabetic patients. In addition to offering primary care, nurses should develop strategies to improve their services to patients. Nurses require being creative and initiative as professional virtues. When combined with their caring character, the two traits would enable nurses make essential transformations in diabetes management.It is also advisable that since the occurrence of diabetes varies with genetics, culture, social practices and geographical locations, nurses and other practitioners should be sensitive of the variations. Generally, primary care should see to it that preventive measures are fully exploited just as the ones addressing diabetes treatment. In primary care for instance, clinicians should encourage patients to engage into healthy livelihood. Dietary and exercise intervention are essential at the primary level of care for old people with diabetes. Other parties involved in primary care for diabetic patients include dieticians, pharmacists, physicians and psychologists. Professionals from various fields should cooperate to facilitate primary care. Team work as seen in interdisciplinary teams could offer the best outcomes in diabetes management. Patient care is often complex but can be promoted if stakeholders associate appropriately. Practitioners should ensure that the care they offer is patient-centered, and that it constitutes healthy communications with patients, partnerships and focuses beyond the situation at hand. Practitioners require explaining essential concepts of the disease to patients. In addition, they should be able to assess the feelings, expectations as well as beliefs of their patients. Generally, care providers need developing common grounds with their patients. When primary care is patient centered, there are higher chances that satisfaction will be obtained for both the providers and receivers of services.
Future Healthcare Directions in the Management of Diabetes among the Aged in India
Currently, the occurrence of diabetes among the aged in India is alarming. There should be long-term strategies to help overcome the situation. There are, therefore, rapid changes in the management of diabetes as approaches are unlimited (Universit5y of Melbourne, 2011). Researches are carrying out studies to develop better means of addressing diabetes among all populations. For instance, there are moves to develop new drugs that can be more effective than the current regimens. Ramachandran et al. explored possible drugs that may help fight diabetes in the future. The researchers indicated that analogues of glucagon as well as those of dipeptidyl peptidase-4 could offer better therapeutic agents in the future (2010, Pg. 8). Researchers are carrying out clinical studies on new drugs and in the near future, there could be drugs that would change the common regimens applied for diabetes. Drugs in advanced developmental stages include DPP-4 inhibitors, which include vidagliptin and sitagliptin (Ramachandran et al., 2010, Pg. 8). As Ramachandran et al. expressed, the two drugs improve the sensitivity of beta cells to insulin, and could be useful for diabetes mellitus type 2 (2010, Pg. 8). Measures that address livelihood seem to offer the best approach on management of diabetes. Dietary modifications and engagement in exercise can lead to high performance in minimization of diabetes cases in India, especially among old people. Oral drugs, which currently are the most used in diabetes, may not be the first-line choices as times goes by. Better means of managing diabetes will be developed to ease the burden of having to take medications on daily basis.Drugs that would be more preferred in the future, should not only manage diabetes, but also its comorbidities. Again, their use should guarantee optimal safety while still being effective. Since insulin is the central hormone in diabetes, researchers are likely to develop its receptor agonists as therapeutic agents (Sanofi Diabetes, 2012). There are also moves to develop long-acting drug compounds that would have great effect in management of diabetes.Usually, challenges with the current diabetes therapies necessitate the development of new therapies.
Conclusion
India has the highest cases of diabetes mellitus in the world. Diabetes mellitus is more prevalent among the old than it is with the young. Indian population faces several risk factors that predispose them to the disease. These factors include genetics as well as social and cultural factors. Social practices and cultural beliefs often influence health care provision. In most cases, cultural beliefs work against care provision for the aged diabetic patients in India. To address the high occurrence of diabetes in India, clinicians and the government take a central position. It is upon clinicians to ensure that they offer quality care to diabetic patients in the move to manage the disease.
References
Asif, M. (2014). The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. Journal of Education and Health Promotion, 3, 1. https://www.doi:10.4103/2277-9531.127541
Kalra, S., Sridhar, G. R., Balhara, Y. P. S., Sahay, R. K., Bantwal, G., Baruah, M. P., … Prasanna Kumar, K. M. (2013). National recommendations: Psychosocial management of diabetes in India. Indian Journal of Endocrinology and Metabolism, 17(3), 376–395. https://www.doi:10.4103/2230-8210.111608
Kaveeshwar, S. A., & Cornwall, J. (2014). The current state of diabetes mellitus in India. The Australasian Medical Journal, 7(1), 45–48. https://www.doi:10.4066/AMJ.2013.1979
Khalil, H., Tan, A., & George, J. (2012). Diabetes management in Australian rural aged care facilities: A cross-sectional audit. Australas Med J, 5(11), 575–80
Kumar, A., Goel, M. K., Jain, R. B., Khanna, P., & Chaudhary, V. (2013). India towards diabetes control: Key issues. Australas Med J, 6(10), 524–531.
Larrañaga, A., Docet, M. F., & García-Mayor, R. V. (2011). Disordered eating behaviors in type 1 diabetic patients. World Journal of Diabetes, 2(11), 189–195. https://www.doi:10.4239/wjd.v2.i11.189
Mkilat, A. J., O’Hara, B., & Develin, E. (2009). Concepts and new frontiers for development – What role should health promoters play in lifestyle-based diabetes prevention programs in Australia? Health Promotion Journal of Australia, 20(2), 86-94
Ramachandran, A., Das, A. K., Joshi, S. R., Yajnik, C. S., Shah, S., & Kumar, K. M. (2010). Current Status of Diabetes in India: Need for Novel Therapeutic Agents. JAPI, 58, 7-10
Rao, C. R., Kamath, V. G., Shetty, A., Kamath, A. (2011). A cross-sectional analysis of obesity among a rural population in coastal southern Karnataka, India. Australas Med J, 4(1), 53–57.
Sukala, W. R., Page, R. A., Rowlands, D. S., Lys, I., Krebs, J. D., Leikis, M. J., & Cheema, B. S. (2012). Exercise intervention in New Zealand Polynesian peoples with type 2 diabetes: Cultural considerations and clinical trial recommendations. Australas Med J,5(8), 429–35
The International Expert Committee. (2009). International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care, 32, 1327–34
Unnikrishnan, R. I., Anjana, R. M., &Mohan, V. (2011). Importance of Controlling Diabetes Early–The Concept of Metabolic Memory, Legacy Effect and the Case for Early Insulinisation. JAPI, 50, 8–12.
We can write this or a similar paper for you! Simply fill the order form!
Guidelines attached….. APA Referencing and Turnitin Report required
SAMPLE ANSWER
An advance care plan is a structured and ongoing communication or discussion between a patient and a professional health caregiver which is meant to communicate the future wishes of the patient in matters concerning treatment and care options should they not be able to communicate these wishes at that particular time. (Oliver, 2013, pg 135) The discussion might also involve a third party such as the patients close family member. Mr. Mario who lives with his wife, Rosa, is a 46 year old man with stage 4 pancreatic cancer who has just been told by his oncologist that the chemotherapy treatment he was receiving is no longer effective. Over the past few days, Mr. Mario has been experiencing symptoms such as nausea. The following is an essay concerning Mr. Mario’s advance care plan.
Initiating the conversation on advanced care planning
This conversation is meant to discuss with a patient the method and means he would like to be treated or taken care with once he or she falls seriously ill and he is not able to make such decisions then. Usually, this conversation is started when it is clear that a patient’s health risk is very high and so is the case with Mario. The conversation on advanced care planning with Mario should have been initiated after being told by the oncologist that the chemotherapy was unlikely to be ineffective and that is the same period when he decided that he would focus on the time he has with his family. During the initiating of the conversation, it is important to explain to Mr. Mario what the conversation is all about and the importance. It is after this that he should then be asked if there is anyone who he thinks should be present during the conversation. This should then be followed by the deliberate allowing of time so as to provide the patient with an opportunity to reflect. (Yeung, Escalante & Gagel, 2009, pg.46)
After that, the conversation can then begin and this must be done by using words not too insensitive to the patient for example, ‘I would like to discuss with you about your wishes of future care in case you get very sick which might not happen but just in case it does you will not be able to express your wishes and at that point it would be very important to know what you would have wanted’, ‘Have you considered about the place or type of care you would want to have in case you became too sick to take care of yourself?’ or ‘most people usually think about what they may want in the future and they usually have their wishes drafted in a document called Advance Health Directive. Would you like to know more about this Advance Health Directive?’
Preparing for the conversation
There are some very important issues that should be taken into consideration in preparation of the advance care planning discussion and this is mostly so as to protect and maintain the welfare of the patient and this are as follows
Firstly, one should review all medical files notes or files of the patient. This is meant to ensure that all that all the relevant and critical clinical information concerning the patient are available. The same can still be achieved through consulting other medical care experts involved with the patient. (Goldstein & Morrison, 2013, pg 273)
Secondly, the health care professional should also ensure that he or she has a private and comfortable area to carry out the discussion. This area should be free from interruptions from anyone. This will help in boosting concentration while collecting all the necessary information. In addition to finding a private area, one should determine if there is a family member who can participate in the discussion. This family member should be a very close family member. This can be determined through scrutinizing the patients’ health and personal documents.
Moreover, it should be made sure that the patient is in a mental capacity to participate in the discussion. This is so because the patient, if not in the capacity to discuss these matters, can easily fall into a depression. If there is a family member participating in the discussion, the same should also be made sure to avoid any cases of afterwards depression. Chambers, Germain & Brown, 2010, pg55)
One should ensure that he or she has drafted a structure that will be used during the advanced care planning process. This can be achieved for example, through having a structure that contains leading question. The draft structure should be able to contain the following components;
it should lead one in identifying the goals, advantages and disadvantages of the methods and interventions that the patient would want sought
it should be able to ensure that the patient knows the level of seriousness of his stage four pancreatic cancer.
It should be able to lead the patient in knowing that his disease is palliative.
It should also be able to identify the patient’s fears or greatest concerns.
It should be able to determine what the patient thinks about the advance care planning.
One should have an understanding and be well conversant with all local laws that concern the drafting and implementation of such critical documentation. One should also ensure that he or she has adequate knowledge on how to access the necessary documents.
Lastly, arrangements for the appropriate support services should be made prior to the initiating of the conversation. Among other things, this support service can be helpful in consoling the patient if he or she gets emotional during the conversation and breaks down.
Who should be involved in the discussion?
An advanced care planning discussion usually involves a patient and it also advisable for very close family member to be present although the consent of the patient will have to be sought first. In the case of Mr. Mario, his close family member is his wife Rosa, so it would be appropriate to involve his wife in the discussion. Both the participants will be required to participate in the discussion through sharing their opinions concerning the advance care plan. Mr. Mario could also choose for his attorney to be present especially if he is interested in transferring his power of attorney to a different person such as Rosa who would be required by the power of attorney to make decisions for his husband when the husband is not in a capacity to do so. Whatever is discussed in the advance care plan is then documented which will make it easy to use for future references. The wishes are then legalized through filling out legal forms entailing all your wishes. This can be done with the help of an attorney although it is not necessary. (Noogle, 2012, pg 57)
Information to be included in the advance care plan
There are issues that should be included in an advance care plan. For an effective outcome, this should mostly be in the form of questions. The issues to be addressed should be as follows;
Firstly, there should be goals, advantages and disadvantages of any interventions that might be required when taking care of the patient. These goals may include decisions of emergency treatments to keep the patient alive such cardiopulmonary resuscitation (CPR) which is meant to restore the heartbeat if it stops, comfort care which involves relieving pain, artificial nutrition or artificial hydration which are meant to provide nutrition to the patient through a tube when the patient is unable eat or drink. This is meant to ensure that Mr. Mario fully understands the consequences of any method before preferring for it to be used in the advance care plan. (Thomas & Lobo, 2011, pg 239)
Secondly, the plan should be able to address the patients preferred place for receiving future care and this is meant to ensure that the patient is comfortable in receiving this care for example; this could be asked as ‘where would you prefer to receive future care?’
Although not necessary, the patient should be given the opportunity to decide whether he would like to donate any organ or tissue in case of death and the question asked could be; ‘incase of death, would you like to donate any of your body organ or tissue? If so where or to whom would you want the above stated organ or tissue donated?’ (Vadivelu, Kaye & Berger, 2013, pg 100).
The advance care plan should be able to make sure that the patient and his wife are aware of the extent of seriousness and risk of his pancreatic cancer. This is one of the means of ensuring that the participants are in the right mental capacity to get involved in the discussion. For example, this could be asked in the form; ‘are you aware of the extent of risk of your level four pancreatic cancer? If so what do you think are the risks involved?’
The care plan should be able to inquire from the patient the people he would like to make decisions for them in case they are unable to make these decisions. The care plan should still be able to inquire if the patient has shared his wishes with his family or friends. This could be in the form; ‘Incase your are not able to make any decision, whom would you like to act in your capacity in making these decisions? Apart from your wife, have you informed any other family member or friend of your wishes?’
The plan should be able to diagnose Mr. Mario’s gravest and deepest fears concerning his pancreatic cancer. The same should also be inquired from his wife, Rosa. For example this could be asked as ‘what are your deepest fears concerning this disease?’
Lastly, the advance care plan should give Mr. Mario or his wife the opportunity to ask any question related to Mr. Mario’s health that might have not been addressed in the care plan. This could be asked as ‘Is there any other issue concerning the disease that you would want addressed here?’
Reviewing of the advance care plan
This involves the revisiting of the advance care plan discussions and at times the decisions set out in the advance care plan can be changed. It is usually advisable for the reviewing to be done regularly due to a number of reasons which can apply in Mr. Mario’s case. The following are the main reasons for reviewing the plan or circumstances that might trigger the reviewing process
Firstly, Mr. Mario or his wife could request for the reviewing or change their mind about a decision that they had made earlier this might for example, be triggered by the infeasibility of an option that they had recommended maybe due financial constraints or a number of other issues.
Secondly, there could be a change in circumstances that might require the reviewing of the plan. For example, change in medical conditions whereby a new disease or condition is discovered in the patient. The same could also be triggered by change of individual conditions for example incase Rosa, Mr. Mario’s wife, dies or any other person mentioned in the advance care plan and whose death affects the plan.
Thirdly, the reviewing can be done when Mr. Mario returns to the hospital for example when he is going back for a checkup or when the health care professional visits Mr. Mario at his home. Usually, the reviewing of the plans is usually set to be done constantly and in such cases the reviewing is done when the patient visits the hospital or when the health care professional visits the patient at home. (Hartmann, Loprinzi & Mayo Clinic, 2012, pg 45)
Fourthly, the reviewing can be done if the medical options that are present in the advanced care plan changes the needs of Mr. Mario in regards to the plan for example in the discovering of a co morbidity.
Fifthly, Mr. Mario can revoke the advance care plan any time and this will require the preparation of a new advance care plan. In such a scenario Mr. Mario might view the earlier on plan as not been appropriate due to a number of reasons and this will require him to revoke the care plan and request for the drafting of a new one.
Lastly, during the making of the advance care plan, Mr. Mario can state a review interval of which after the interval time lapses, the making of a new advance care plan will be required. For example, Mr. Mario could state that he would require reviewing the care plan after every two months. After the lapse of these two months, Mr. Mario will then be required to review the care plan.
Activation of the advance care plan
This involves the point and time at which the discussion in the plan will be implemented. In Mr. Mario’s scenario this will take place under the following circumstances.
Firstly, activation can occur if Mr. Mario enters into a comma for example, after he collapses at the shopping centre and becomes non responsive and is taken to the hospital. If he completely fails to respond, then implementation of the care plan will be deemed necessary.
Secondly, the activation can occur in case of Mr. Mario deaths. In this case the advance care plan will be activated in that, if he had requested in the care plan for his body tissue or organ to be donated, then his wish will have to be fulfilled. (Barnsteiner, Disch, Walton & Sigma Theta Tau International, 2014, pg 107)
Thirdly, the activation maybe triggered by the person who has the power of attorney. This involves transferring your rights to make decisions concerning certain issues to another person who is required by law to make decisions that will be in your best personal interests if you are not in a capacity to make these decisions. In this case Mr. Mario could have given this power to his wife Rosa so if by any chance Rosa feels that Mr. Mario is not in a capacity to make decisions then she can ask for the implementation of the advance care plan.
Fourthly, the activation of the care plan can be triggered if Mr. Mario experiences dementia. This is a condition whereby the patient’s mental ability is impaired and cannot make decisions as a reasonable man. In such a case the patient will not be in the right mental capacity to make a reasonable decision so this will require the fulfilling of his wishes as he had earlier on stated in the care plan. (Leah & Susana 2013)
Lastly, the activation can be triggered by a medical condition which will make it impossible for Mr. Mario to communicate his decisions such as stroke or paralysis. In such a condition, the patient might be in good mental capacity to make decisions for himself but the communication of this decision might be difficult hence necessitating the use of his wishes as stated in the advance care plan
In conclusion, an advance care plan plays a very crucial role since it betters the quality of life of the patients, provides medical care which is less aggressive, helps families prepare for the death of a loved one and also helps in resolving family conflicts. (Thomas & Lobo, 2011, pg 78)
References
Oliver, D. (2013). End of life care in neurological disease. London: Springer
Yeung, S.-C. J., Escalante, C. P., & Gagel, R. F. (2009). Medical care of cancer patients. Shelton, Conn: People’s Medical Publishing House.
Goldstein, N. E., & Morrison, R.S. (2013). Evidence-based practice of palliative medicine. Philadelphia: Elsevier/Saunders.
Hartmann, L. C., Loprinzi, C. L., & Mayo Clinic. (2012). The Mayo Clinic breast cancer book. Intercourse, PA: Good Books.
Weis, J,. & Horneber, M. (2014). Cancer related fatigue
Noogle, C. A. (2012). Neuropsychology of cancer and oncology. New York: Springer Pub.
Chambers, E. J., Germain, M., & Brown, E. A. (2010). Supportivecare for the renal patient. Oxford: Oxford University press.
Fischer, S., Gozansky W., Sauaia A., Min S.,Kutner J., Kramer A. (2006). A practical tool to identify patients who may benefit from a palliative approach: the caring criteria Shrewsbury, UK: NHS 285
Thomas, K., & Lobo, B. (2011). Advance care planning in end of life care. Oxford: Oxford University Press.
In Vadivelu, N., In Kaye, A. D., & In Berger, J. M. (2013). Essentials of palliative care.
Melnyk , B. M., & Fineout-Overhault, E. (2011). Evidence based practice in nursing & healthcare: A guide to best practice. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
In Christensen, A. J., In Martin, R., & In Smyth, J. M. (2014). Encyclopedia of health psychology.
In LoBiondo-Wood, G., & In Haber, J. (2014). Nursing research: Methods and criticsl appraisal for evidence-based practice.
Barnsteiner, J. H., Disch, J.M., Walton, M. K., & Sigma Theta Tau International, (2014). Person and family centered care.
Leah, R., & Susana L. M. (2013). Advance care planning: communicating about matters of life and death. New York: Springer Pub.
Jessica has been feeling unwell for the last 2 days with cold like symptoms, clear discharge from her nose, low grade fever and occassional coughing at night. The following nigh Jessica woke short of breath. Jessica’s mother, Anne , also noticed that Jessica’s breathing was quite noisy.
Anne, Jessica’s mother sat Jessica upright, found her salbutamol puffer and spacer which was on her bedside table and administered six puffs via her spacer as instructed by the asthma nurse at her local GP practice. Jessica’s breathing appeared to settle not long after the puffer and she then went back to sleep.
Anne woke with a start 2 hrs later and rushed to Jessica’s room and found her becoming increasingly short of breath and coughing continuously. Anne gave Jessica a further 6 puffs of salbutamol through her spacer. Jessica’s breathing did not appear to be improving, so Anne decided that they should go to the hospital.
One of Jessica’s cousin is a second year student nurse. He tells you he doesn’t understand the pathophysiology of asthma and how it affects the respiratory system. Jessica’s mother Anne asks you to explain to him the pathophysiology of asthma and how it affects the respiratory system using the correct medical and nursing terminology. You are also to explain two signs and symptoms that the patient Jessica has presented, therefore, shortness of breath and wheezing/coughing and explain why they manifested as part of the illness/disease.
SAMPLE ANSWER
Pathophysiology of Asthma
Asthma is a long-lasting inflammatory ailment of the breathing systems. It can be classified in different ways; physiologically, pathologically and bronchoconstriction. Physiologically it can be observed as an adjustable. It can also be partly reversible by blocking of airflow just as in the case of Jessica. Your aunt Anne, following doctor’s instructions used salbutamol puffer and as pacer to reverse the blocked air.
Pathologically it comes with overdeveloped mucus glands and airway thickens due to scarring inflammation and bronchoconstriction and thinning of the respiratory system in the lungs due to the tightening of adjoining soft muscles.It has many symptoms and among them is feeling extreme cold, clear discharge from the nose, low-grade fever and frequently coughing at night. These symptoms of asthma have implications for the diagnosis, management, and potential prevention of the disease (Murphy, 2011, Pg. 78).
Pathophysiology or physiopathology is a word that is formed by the combination of two words;pathology and physiology. Pathology is a medical discipline that is used to explain conditions that are initially seen during a disease and in this case, Jessica’s ailment, On the other hand, physiology is the biological word for defining procedures or methods which operate within a person. Pathology has always been used to describe the irregular or undesired disorder. On the other hand, pathophysiology tries to explain the physiological processes or mechanisms in which such a condition grows and advances. (Marthan., R, et al. 2014, pg. 153)
Pathophysiology is also used to mean the functional variations related with or resulting from illness or injury. Lastly, it can also be defined as the practical changes that accompany a specific disease.
How it affects the respiratory system
During an asthma incident, swollen breathing system react to environmental activates such as smoke, dust, or pollen. The airways become narrow due to excess mucus, these makes breathing difficult. In essence, asthma is the result of a resilient response in the bronchial airways (Loo, 2009, Pg. 67). The airways of asthma patients are oversensitive to certain activates, also known as stimuli. In response to exposure to these triggers, the bronchi having large airways contract into spasm that is an attack by asthma. Further Inflammation leads to further narrowing of the breathing system due to excessive mucus that is produced. This causes coughing and other breathing difficulties. Bronchospasm may resolve impulsively in a period of two hours, or in about half of the subjects, may become part of a delayed response.
This initial insult is followed three to twelve hours later with further bronchoconstriction and inflammation.The normal ability of the bronchus is usually maintained by a stable operative found in the autonomic anxious system. Both of them function involuntarily. The parasympathetic impulse circle having afferent nerve finales that originates underneath the inner linings of the bronchus. Whenever these afferent nerve endings are stimulated by different things such as dust, cold air or fumes, impulses travel to the brain-stem called the vagal center, and then it moves down the vagal efferent pathway up to the bronchial small breathing system (Harver & Kotses, 2010, pg. 585). When it reaches here acetylcholine is released from the afferent nerve endings which results in the extreme creation of inositol one, four and 5-trisphosphate (IP3) in the bronchial smooth muscle cells which lead to muscle shortening and this initiates bronchoconstriction that brings the chest problems of difficulty in breathing that is called asthma (Murphy, 2011, pg. 46).
Shortness of breath in asthma and its manifestation
Asthma is a lifetime ailment that makes someone’s lungs hypersensitive and hard to breathe. It is an incurable disease, but with right treatment, people with asthma can lead healthy, active lives. Shortness of breath is a feeling whereby you get a dyspnea. Dyspnea is having a difficulty in breathing. If one has asthma, their breathing passages are highly sensitive. Some things can thereby make their respiratory system encounter some problems. One of the problems faced is swollen and blocked airways. This is as a result of excessive mucus. The swelling and mucus make the respiratory system narrow. This causes difficulty in breathing. This is one of the primary signs of an asthma patient even before diagnosis is carried out (Wolfson & Montgomery-Downs, 2013, Pg. 751). Other symptoms of asthma include wheezing, chest tightness and chronic cough as in the case of Jessica.There is no medical terminology for shortness of breath. Asthma patients will frequently describe this trouble of breathing in different ways. While others call it unable to catch my breath, others call it gasping for breath. (WebMD. 2015)
Wheezing and in asthma and its manifestation
These are some of the most common asthma symptoms and are often the purpose why many people look out for care. Wheezing makes a patient produce a high-pitched sound during respiration. Mostly, it occurs when he patient breaths out but can also be heard when they breath in. The narrowing of the respiratory passages due to inflammation is the primary cause of wheezing.
References
Marthan., R, et al. 2014. Pathophysiology of asthma. Europe Pub Med CenteMorris., J, et al.2015. Asthma. Medscape
WebMD. 2015. Symptoms of Asthma. Medical Health Center.Viewed at www.webmd.com 25/05/2015
Murphy, W. B. (2011). Asthma. Minneapolis, MN: Twenty-First Century Books.
Wolfson, A. R., & Montgomery-Downs, H. (2013). The Oxford handbook of infant, child, and adolescent sleep and behavior.
Loo, M. (2009). Integrative medicine for children. St. Louis, Mo: Saunders/Elsevier.
Harver, A., & Kotses, H. (2010). Asthma, health, and society: A public health perspective. New York: Springer.
We can write this or a similar paper for you! Simply fill the order form!
Guidelines : Only Text Referencing at the last page but make sure in APA 6th Edition Format
No Wikipedia or better health reference……….. only books journal and govt. web pages referencing
SAMPLE ANSWER
Dissociative Disorders
Dissociative is the adjective of the noun dissociation and the verb dissociate. From the medical perspective, Merriam Webster Dictionary defined dissociation as separation of personalities. Dissociation could occur at the level of character segments or specific mental processes from the current state of consciousness or behavior (2015, “Dissociation”). If something is dissociative, it has the characteristic of disconnection from other parts.
National Alliance for Mental Illnesses (NAMI) explained that patients of dissociative disorder disconnect from the reality. They lose their thoughts and identity, as well as consciousness and memory (2015). The abnormalities incapacitate the mental abilities of the affected. They are prevalent in all populations regardless of ethnicity, geographical regions, socioeconomic status or any other variations. NAMI pointed out that approximately 2% of the States’ population experiences the disorder. However, mild episodes of the diseases affect half of the Americans at least once in their lives. Gender influences the occurrence of the illnesses, and females are more prone to them than males (2015).Dissociativedisorder accounts for a significant percentage of the few psychiatric problems among the American population.
Signs and Symptom
In most cases, signs of dissociative disorder appear after exposure to physical or mental trauma. War and accidents are major inducers of the symptoms. Victims progressively exhibit deteriorating mental health characterized by stressful moments. Though signs and symptom vary with the specific type of the disorders, stress is a common characteristic of all types. Other common signs and symptoms as NAMI outlined include out-of-body feelings, where patients fail to understand themselves. Patients also fail to develop self-identity, emotional availability, and reliable memories.Usually, people develop anxiety and depression, and they are likely to contemplate suicide (2015).Generally, mental torture is the predominant symptom of the disorder.
Types of Dissociative Disorders
In its DSM-5 manual, the American Psychiatric Association split dissociative disorder into three categories. The three are Dissociative Identity Disorder (DID), Dissociative Amnesia, and Depersonalization Disorder. Some psychiatrists, however, identify two more types of the disorder. The additional two are Dissociative Fugue and the unspecified Dissociative Disorder.Since Dissociative Fugue has most properties seen in Dissociative Amnesia, psychiatrists often classify it under the latter (Spiegel, Fernandez, Lanius, Vermetten, Simeon, & Friedman, 2013, Pg. 299). Different types of the disorder have varied severity of symptoms, as well as thenature of their stressors (Steinberg, 2015).
Dissociative Identity Disorder
DID was commonly referred to as multiple personality disorderuntil recently. The disease mainly traces origin from childhood exposure to physical, sexual or emotional abuse. People exhibit more than one distinctive character. The affected people can assume different behavior and thoughts with time. They easily lose memories about self and experience severe mood swings. Also, patients could have attention deficit disorder impairing their ability to learn.
Diagnoses and Intervention for DID
DID is the severest of the five types of dissociative disorder. Its detection and diagnosis require specialized tests and examinations. As Steinberg explained, hidden symptoms characterize DID, and anxiety, depression or substance abuse could mask the symptoms. Again it is hard to describe the symptomatic disconnection feeling that occur with the disease (2015). The nature of the disease, therefore, makes it hard to diagnose. Psychotherapy is the first-line treatment for the disorder though medication could as well be used.
Dissociative Amnesia
Patients with dissociative amnesia suffer severe inability to recall their personal information. The brain does not have to be necessarily damaged for the condition to occur (Kikuchi, Fujii, Abe, Suzuki, Takaqi, Mukiqura, & Mori, 2010, Pg. 602) In most cases as Steinberg wrote, a single traumatic event is sufficient to cause the disorder. Experiences of disasters, violence and war are the major inducers of the disease (2015).
Diagnoses and intervention of Dissociative Amnesia
When signs of the disorder are present, the examiner would perform physical tests to close out other possible causes of the symptoms, and zero into dissociative amnesia. Treatment is crucial to help individuals restore their memories. Psychotherapy, cognitive therapy as well as medication are the commonest approaches to the problem (Goldberg, 2014, Pg. 2).
Depersonalization Disorder
Patients of depersonalization disorder experience unreal sensations. Their mind seems out of touch with their bodies. The ill cannot connect to the reality and feel as though they are dreaming. Complications of the condition are accompanied by moments of derealization. Again, depersonalization traces origin from trauma and stress.
Diagnoses and intervention of depersonalization disorder
To diagnose depersonalization, physicians perform examinations such as blood tests. Though highly prevalent, the condition is often misdiagnosed (Reutens, Nielsen, &Sachdev, 2010, Pg. 278). Drugs used with psychological counseling to manage depersonalization include clonazepam, fluoxetine and clomipramine (Mayo Clinic Staff, 2014, Pg. 8).
Support for Dissociative Disorder Patients
Patients require assistant to cope with mental instabilities created by dissociative disorder. As Halter and Varcarolis pointed out, victims of the disorder require education on best ways of managing their situation. Nurses could for instance explain to the patients that the diseases result as an adaptive means to experiences (2013, Pg. 319). People associating with the sick should treat them with care to avoid inducing more emotional stress. The patients are emotionally delicate, and they can react strangely to unfriendly stimuli. Nurses and other care givers should offer emotional availability, especially when patients recall the events that traumatized them (Varcarolis& Halter, 2012, Pg. 205).
Spiegel, D, Loewenstein, R. J., Fernandez, R., Sar, V., Simeon, D., Vermetten, E., . . .Dell, P. F. (2011). Dissociative Disorders in DSM-5. NCBI, 28(2011), 824-852
Select an advanced professional or advanced practice nursing specialty. How has past and current regulation/legislation affected the role and scope of this nursing role? What, if any, discussions are currently underway relative to the scope and role of this specialty? What resources are available to assist nurses in advocating for these roles?
Select a professional or specialty nursing association. What impact has this organization had on health care legislation in the past 2 years?
This task is due 22nd may 2015\
SAMPLE ANSWER
Health Care: Ambulatory Care Nursing
This case focuses on ambulatory nursing, which significantly differs from other nursing specialties at the level of the scope of practice. Patient care demands change with time and adjustment in various practices in ambulatory nursing are vital. In most cases, the changes require allocation of more roles to nurses. As such, the scope of ambulatory nursing has expanded to improve patient care.
Both past and current regulations have affected ambulatory nursing from different perspectives. As Stokowski (2011) noted, the current views on ambulatory nursing are different from what used to be the understanding ten years ago. The earlier regulation allowed only a narrow scope for ambulatory nursing. Policy makers have made changes in the scope of the field to suit the current patient care requirements. Differences in health care setting have necessitated most of the changes. For instance, there are differences in the occurrence of chronic diseases, lengths of hospitalization, as well as the complexity of procedures performed on patients (Stokowski, 2011). With the new regulations, nurses can attend patients from other more different settings. They can attend patients from offices, community health facilities, homes, schools, and gastrointestinal laboratories among others (Stokowski, 2011).
There are discussions on ambulatory nursing that aim at defining the practice, and describing it in a comprehensive manner. In addition, there are discussions on relating the specialty to general practice as well as those on framework expansion. Stakeholders also address the standards of performance expected from the ambulatory nursing specialists.
To advocate for their roles, nurses use general practice as well as specialty associations. For instance, the American Academy of Ambulatory Care Nurses (AAACN) offers a platform on which nurses in the ambulatory field can discuss and express their opinions. Within the last two years, the AAACN has expressed that ambulatory nurses have a rich background in nursing and that they employ their knowledge to offer quality ambulatory services. In so doing, the association backs nurses in their practice.