I am writing to apply for Operation Manager Job in relation to the advertisement made in the local job website due for a career in this successful Microfinance institution.
I am a focused and highly industrious citizen in Business Management. As outlined in the job specification, I will focus on all the details that revolve around micro finance. Part of the subjects that I will deal with is Relationship oversightwhich includes the effect of the technology and economic trends on consumption, savings and wealth.
It would beagreat opportunity to work in your company as it will help nurture my skills in the market, am available any time for interrogation or verification.
I appreciate your time and hope to hear from you soon.
Yours Sincerely.
RESUME
CAREER DESCRIPTION
I am an ambitious, organized, focused and ready to learn and goal oriented young professional eager to overcome stiff competition to achieve the best possible results in my work.
I am also committed to continuouspersonal development, am creative and innovative with strong personal integrity and work ethics. I have excellent communication and interpersonal skills and also leadership and team work skills.
ACADEMIC QUALIFICATIONS
I am currently pursuing my degree certificate in Business. Besides, I have pursued studies in financial management and public leadership.
WORK EXPERIENCE
Worked with financial institutions where I dealt with
Growing high quality small micro enterprise portfolio.
Managing all client financial relations.
Referees
Principle
School of business
Interview questions
What are your short-range goals?
I am passionate about continuous human interaction and the satisfaction that comes as a result of offering help. I love serving people and therefore I want to part of this company in serving people since I think you guys are doing a great job.
Where do you want to be five years from now?
I am not sure about what the future holds for me. However, am certain that this position will offer me an opportunity and experience in guiding me to make an informed decision.
What special skills do you have?
I have financial skills besides management skills which I believe will help me become more productive in this position.
What kind of job are you most interested in?
I am interested in a job that directly impacts on the lives of other people. Consequently, this will help me work diligently knowing very well that am touching someone’s life somewhere.
What characteristics do you feel are most important for this job?
Leadership
Good leadership will ensure respect and results from both within and outside the business fraternity.
Hard work
So as to realize profits, the position requires dedication.
What is your greatest strength?
Performing well under pressure
I work well under pressure so as to satisfy needsof customers who are the first priority.
What is your major weakness?
I am a perfectionist. I always want to achieve the best in everything that I do.
8. What were your most important achievements in your last position?
I managed to reform performance of the organisation I worked for from a loss making institution into a high profit making institution.
9. Tell me about yourself.
I am pursuing a degree in financial accounting. In addition, I have managed to study business management and leadership.
10. Why do you want to work for this company?
This company stands out as the best financial institution. Over the last five years, it has attracted public interest because of its good customer care relation and service delivery.
11. What kind of recommendation do you think you’ll get from your previous
employer?a very successful leader in my leadership capacity. This is because, over my tenure as an employee in this company, I increased its annual turnover.
12. How do you feel about overtime?
Overtime is one way of encouraging and motivating employees work even within extra hours. It is therefore a good way of increasing production in a company.
13. How long would you stay with us?
I think this is the peak of my career and the beginning of good things. I am here to stay and deliver services to the people.
Why should we hire you?
I am a qualified accountant with a lot of passion in delivering service. My hard work record speaks for itself. If you hire me, I believe I will propel this company to greater heights.
15. Define the following:
Cooperation
Cooperation is the process by which a group of people work together in harmony so as to achieve a common objective.
Responsibility
Responsibility is a situation whereby people within a given organization or institution is answerable in whatever thing they engage in.
Challenging
Challenging is the process by which someone engages in new fields with the main aim of exploring new ways of doing things(Yate & Yate,2012.14).
Your papers needs to highlight specific arguments and ideas in your choose of topic By highlighting these , you need to show the a) the epidemiological data b) the current literature in the field chosen .
Questions you should address
Asking questions such as the following will help you sift through your sources and organize your essay.
What’s been done in this topic area to date? What is the research and population based s, recent key trends ?
What are the gaps and / or weaknesses in the health services provided? Are there new/novel ways of at the issue?
The Marking Criteria for this Assignment
Present a synopsis of the epidemiological background over time ?
What are the key social determinates?
Critically examine the key aspects of primary health care delivery of this health issue
What might be the future healthcare directions?
SAMPLE ANSWER
Global Health
Introduction
This essay explores diabetes as a highly prevalent disease among Indian seniors. Diabetes mellitus is usually more common than insipidus and the essay emphasizes on the former. Two subtypes of diabetes mellitus earn most attention in the study. They are diabetes type 1 and diabetes type 2, also referred to as insulin-dependent and insulin-independent respectively (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 524). In Indian population, diabetes type 2 is more common and severer than type 1.With the characteristic change of livelihood in the recent years, the old in India get higher risk to diabetes than in the earlier days. Some primary care measures in the management of the situation are in place, and there is prospective to better the practice.
Epidemiological Background of Diabetes in India
Diabetes has affected a large population in India, and it still remains a major health issue. The disease accounts for a large percentage of deaths in the country especially among the aged. Currently, 62 million Indians have the condition according to research (Kaveeshwar & Cornwall, 2014, Pg. 45). Studies indicate India as among the nations most affected by diabetes. In 2000, investigations indicated the country as the most hit by diabetes. While India had a diabetic population of 31.7 million, America, the second placed had 20.8 million. China was third with 17.7 million people being diabetic (Kaveeshwar & Cornwall, 2014, Pg. 45). There is likelihood that when global diabetic population increases, India will have contributed the largest population. Factors predisposing Indians to diabetes are many and the situation creates uncertainties for the nation regarding the issue. Though some factors are easily identifiable, others are complicated and stakeholders in healthcare face the challenge of understanding them. Issues that hinder researchers from understanding risk factors include the population’s heterogeneity in relation to ethnicity, culture and socioeconomics (Kaveeshwar & Cornwall, 2014, Pg. 46). Factors currently identified include genetics and the Indian environment. As an environmental factor, livelihood in India predisposes people to obesity, which in turn makes them prone to diabetes.Regional variations are also identified as risk determinants, whereby Indians in rural areas are less exposed to diabetes than their counterparts in towns. The Indian Council of Medical Research (ICMR) found that Maharashtra and Tamil regions have higher statistics of affected people than Chandigarh and Jharkhand, which are to the north of the state (Kaveeshwar & Cornwall, 2014, Pg. 46). Such disparities are also common in other countries such as Australia (Sukala, Page, Rowlands, Lys, Krebs, Leikis, & Cheema, 2012, Pg. 432). Research is yet to prove whether the fact of most people in northern India being migrants while those in south are host could influence the variations. Geographical locations in India also influence diabetes management as access to screening and necessary medication is limited in the rural areas. People who suffer from diabetes in poor regions are more likely to die of the same compared to those in developed regions. In impoverished regions, there is higher likelihood of inadequacy of education offered to people. The aged, for example, may not access education on preventive practices and could face greater risk of diabetes than their educated counterparts (Khalil, Tan, & George, 2012, Pg. 577). The prevalence of diabetes in India is peculiar in that the population is not as much exposed to obesity like in some western countries, yet it records higher cases of diabetes than them. Obesity is not more common in India than these countries, yet it is usually the lead causal factor (Rao, Kamath, Shetty & Kamath, 2011, Pg. 54). In the recent, diabetic complications have increased among the older Indians. A large diabetic population in India expresses inability to control blood sugar level, and ends up developing abnormalities in their vascular structures.
Challenges in the management of diabetes in India include unavailability of HbA1c tests to most Indians (Kumar, 2010, Pg. 128). Insulin therapies are also hard to administer following decreased clinical activeness. Indian guidelines also fail to sufficiently address issues with insulin use therefore making it hard to practice the clinical role (Unnikrishnan, Anjana, & Mohan, 2011, Pg. 10). Managing the current status of diabetes in India requires efforts from the, government as well as other involved parties (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 530). The Indian government has made efforts toward the control the illness. Efforts by the government include the establishment of National Diabetes Control Program (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 524). Healthcare practitioners require helping the population with strategies that address early detection, prevention, and management of diabetes (Kaveeshwar & Cornwall, 2014, Pg. 47). Generally, issues addressed on management of diabetes in India include increasing access to services, increasing the affordability of medicines, improving service quality as well as conducting more studies to develop helpful initiatives (Kumar, Goel, Jain, Khanna, & Chaudhary, 2013, Pg. 525).
Social Determinants in the Management of Diabetes in India
Management of diabetes is subject to several social factors. Stakeholders need to pay attention to such factors in their strategies to improve outcomes in diabetic patients. There is the necessity of research to test outcomes based on social determinants. To curb the increased prevalence of diabetes in India, such research studies are mandatory. Social factors also entail environmental issues, in addition to cultural ones. Diabetes is prevalent among the poor, middle-earning as well as rich populations. India is generally a middle-earning country, and diabetes is more prevalent among the poorer people. Environmental influences in diabetes include feeding habits and physical activities. Intake of food that is highly calorific has increased among Indians causing development of obesity and hence diabetes. Measures in diabetes management include monitoring of one’s diet to lower the risk of taking too much fats and sugar. Asif wrote that people aim at maintaining the safest concentration of sugar and lipids in blood (2014). Health professionals advocate for increased uptake of fruits, whole grains, vegetables, low-fat dairy products and food high in unsaturated fats (Asif, 2014). On the other hand, diabetes management requires reduced intake of red meat, legumes, fish and nuts (Asif, 2014).The International Expert Committee provided dietary guidelines for management of diabetes. In the guidelines, experts advise patients to take carbohydrates as starch. While patients should avoid refined sugars, they may take non-nutritive sweeteners. In addition, people should avoid animal fats, salt, and tobacco smoking (2009, Pg. 1328). Again, failure to engage in physical strains as is the common situation with advanced technology, places people at the risk of diabetes. Given that India has realized substantial developments in technology, the aged in the country are unlikely to take manual activities. For instance, the old would prefer driving to walking even when covering short distances. Failure to exercise leads to too much fat deposits in the body and individuals are likely to become obese. Since the old have machines at their disposal, management of diabetes could be difficult as it requires them to forego machines for manual actions. As a measure to manage diabetes, care providers educate patients on matters relating to the disease. As Larranaga, Docet and Garcia-Mayor wrote, teams concerned with the management of diabetes should monitor insulin regimens, while still educating patients (2011, Pg. 190). Psychosocial approaches are also important in the management of diabetes in India. Kalra, Sridhar, Balhara, Sahay, Bantwal, Baruah, and Kumar addressed psychosocial influences in diabetes management. The researchers indicated that optimal outcome in managing the disease entails physical, social as well as psychological fitness (2013, Pg. 380). Psychological status, particularly, affect administration of self-care in diabetic patients. Kalra et al. noted that psychological factors affecting patients in India differ significantly from those associated with patients elsewhere (2013, Pg. 380). Economic factors are also crucial in the management of diabetes. A significant part of the Indian population is poor, and may not meet the financial costs of insulin treatment. In addition, culture and religion as social practices determine the level of diabetes management. Generally, these practices interact with healthcare provision, hence influencing it. Some attitudes developed with culture, combined with illiteracy may hinder care for diabetic patients. Some uneducated people are unlikely to understand the complexity of issues associated with diabetes management. Use of traditional medicine, a relatively common practice in India, also influences diabetes management from a societal perspective. 14% of Indians use herbal medication and some people in the population may not readily accept convectional medicine that most care providers offer (Kalra, et al. 2013, Pg. 379).
Primary Healthcare Delivery in the Management of Diabetes among the Aged in India
Milat, O’hara and Develin explained that primary care usually focuses on disease prevention (2009, Pg. 87). As such, campaigns characterize the type of care. If properly conducted, primary care can reduce the occurrence of diabetes. In people who are already diagnosed with the disease, elderly Indians for this case, primary care aims at attaining a normal concentration of sugar in their blood. (Ramachandran, Das, Joshi, Yajnik, Shah, & Kumar, 2010, Pg. 8). There is need for clinicians to offer quality care to patients as complications of diabetes could result into other life-threatening illnesses. Ramachandran et al. noted hat more than half of diabetic patients in India possess poor ability to control their blood sugar, and their vascular structures have abnormalities (2010, Pg. 8). Clinicians also require awareness on high standards of care especially with newly developed therapeutic agents. United Kingdom Prospective Diabetes Study (UKPDS) offered recommendations that 53% of diabetes patients receive insulin therapy for six years, while 75% should take more than one treatment strategies for approximately nine years. When offering primary care, practitioners should understand that too much insulin could induce obesity, worsening the situations of patients resistant to it (Ramachandran et al., 2010, Pg. 8). In primary care, clinicians can attend large populations of patients and establish follow-ups. When attending aged people with diabetes, practitioners in India should establish links with their patients to facilitate the process of care delivery. Nurses should lead in implementation of strategies that educate patients on diabetes. In addition, primary care providers need to be optimistic, and encourage their patients to increase their chances of recovery. Though diabetes is a chronic disease, patients can still lead an enjoyable lifestyle if they receive high quality primary care. Since nurses have intensive expertise in counseling, they assume the most effective position in primary care for diabetic patients. In addition to offering primary care, nurses should develop strategies to improve their services to patients. Nurses require being creative and initiative as professional virtues. When combined with their caring character, the two traits would enable nurses make essential transformations in diabetes management.It is also advisable that since the occurrence of diabetes varies with genetics, culture, social practices and geographical locations, nurses and other practitioners should be sensitive of the variations. Generally, primary care should see to it that preventive measures are fully exploited just as the ones addressing diabetes treatment. In primary care for instance, clinicians should encourage patients to engage into healthy livelihood. Dietary and exercise intervention are essential at the primary level of care for old people with diabetes. Other parties involved in primary care for diabetic patients include dieticians, pharmacists, physicians and psychologists. Professionals from various fields should cooperate to facilitate primary care. Team work as seen in interdisciplinary teams could offer the best outcomes in diabetes management. Patient care is often complex but can be promoted if stakeholders associate appropriately. Practitioners should ensure that the care they offer is patient-centered, and that it constitutes healthy communications with patients, partnerships and focuses beyond the situation at hand. Practitioners require explaining essential concepts of the disease to patients. In addition, they should be able to assess the feelings, expectations as well as beliefs of their patients. Generally, care providers need developing common grounds with their patients. When primary care is patient centered, there are higher chances that satisfaction will be obtained for both the providers and receivers of services.
Future Healthcare Directions in the Management of Diabetes among the Aged in India
Currently, the occurrence of diabetes among the aged in India is alarming. There should be long-term strategies to help overcome the situation. There are, therefore, rapid changes in the management of diabetes as approaches are unlimited (Universit5y of Melbourne, 2011). Researches are carrying out studies to develop better means of addressing diabetes among all populations. For instance, there are moves to develop new drugs that can be more effective than the current regimens. Ramachandran et al. explored possible drugs that may help fight diabetes in the future. The researchers indicated that analogues of glucagon as well as those of dipeptidyl peptidase-4 could offer better therapeutic agents in the future (2010, Pg. 8). Researchers are carrying out clinical studies on new drugs and in the near future, there could be drugs that would change the common regimens applied for diabetes. Drugs in advanced developmental stages include DPP-4 inhibitors, which include vidagliptin and sitagliptin (Ramachandran et al., 2010, Pg. 8). As Ramachandran et al. expressed, the two drugs improve the sensitivity of beta cells to insulin, and could be useful for diabetes mellitus type 2 (2010, Pg. 8). Measures that address livelihood seem to offer the best approach on management of diabetes. Dietary modifications and engagement in exercise can lead to high performance in minimization of diabetes cases in India, especially among old people. Oral drugs, which currently are the most used in diabetes, may not be the first-line choices as times goes by. Better means of managing diabetes will be developed to ease the burden of having to take medications on daily basis.Drugs that would be more preferred in the future, should not only manage diabetes, but also its comorbidities. Again, their use should guarantee optimal safety while still being effective. Since insulin is the central hormone in diabetes, researchers are likely to develop its receptor agonists as therapeutic agents (Sanofi Diabetes, 2012). There are also moves to develop long-acting drug compounds that would have great effect in management of diabetes.Usually, challenges with the current diabetes therapies necessitate the development of new therapies.
Conclusion
India has the highest cases of diabetes mellitus in the world. Diabetes mellitus is more prevalent among the old than it is with the young. Indian population faces several risk factors that predispose them to the disease. These factors include genetics as well as social and cultural factors. Social practices and cultural beliefs often influence health care provision. In most cases, cultural beliefs work against care provision for the aged diabetic patients in India. To address the high occurrence of diabetes in India, clinicians and the government take a central position. It is upon clinicians to ensure that they offer quality care to diabetic patients in the move to manage the disease.
References
Asif, M. (2014). The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. Journal of Education and Health Promotion, 3, 1. https://www.doi:10.4103/2277-9531.127541
Kalra, S., Sridhar, G. R., Balhara, Y. P. S., Sahay, R. K., Bantwal, G., Baruah, M. P., … Prasanna Kumar, K. M. (2013). National recommendations: Psychosocial management of diabetes in India. Indian Journal of Endocrinology and Metabolism, 17(3), 376–395. https://www.doi:10.4103/2230-8210.111608
Kaveeshwar, S. A., & Cornwall, J. (2014). The current state of diabetes mellitus in India. The Australasian Medical Journal, 7(1), 45–48. https://www.doi:10.4066/AMJ.2013.1979
Khalil, H., Tan, A., & George, J. (2012). Diabetes management in Australian rural aged care facilities: A cross-sectional audit. Australas Med J, 5(11), 575–80
Kumar, A., Goel, M. K., Jain, R. B., Khanna, P., & Chaudhary, V. (2013). India towards diabetes control: Key issues. Australas Med J, 6(10), 524–531.
Larrañaga, A., Docet, M. F., & García-Mayor, R. V. (2011). Disordered eating behaviors in type 1 diabetic patients. World Journal of Diabetes, 2(11), 189–195. https://www.doi:10.4239/wjd.v2.i11.189
Mkilat, A. J., O’Hara, B., & Develin, E. (2009). Concepts and new frontiers for development – What role should health promoters play in lifestyle-based diabetes prevention programs in Australia? Health Promotion Journal of Australia, 20(2), 86-94
Ramachandran, A., Das, A. K., Joshi, S. R., Yajnik, C. S., Shah, S., & Kumar, K. M. (2010). Current Status of Diabetes in India: Need for Novel Therapeutic Agents. JAPI, 58, 7-10
Rao, C. R., Kamath, V. G., Shetty, A., Kamath, A. (2011). A cross-sectional analysis of obesity among a rural population in coastal southern Karnataka, India. Australas Med J, 4(1), 53–57.
Sukala, W. R., Page, R. A., Rowlands, D. S., Lys, I., Krebs, J. D., Leikis, M. J., & Cheema, B. S. (2012). Exercise intervention in New Zealand Polynesian peoples with type 2 diabetes: Cultural considerations and clinical trial recommendations. Australas Med J,5(8), 429–35
The International Expert Committee. (2009). International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care, 32, 1327–34
Unnikrishnan, R. I., Anjana, R. M., &Mohan, V. (2011). Importance of Controlling Diabetes Early–The Concept of Metabolic Memory, Legacy Effect and the Case for Early Insulinisation. JAPI, 50, 8–12.
We can write this or a similar paper for you! Simply fill the order form!
Guidelines attached….. APA Referencing and Turnitin Report required
SAMPLE ANSWER
An advance care plan is a structured and ongoing communication or discussion between a patient and a professional health caregiver which is meant to communicate the future wishes of the patient in matters concerning treatment and care options should they not be able to communicate these wishes at that particular time. (Oliver, 2013, pg 135) The discussion might also involve a third party such as the patients close family member. Mr. Mario who lives with his wife, Rosa, is a 46 year old man with stage 4 pancreatic cancer who has just been told by his oncologist that the chemotherapy treatment he was receiving is no longer effective. Over the past few days, Mr. Mario has been experiencing symptoms such as nausea. The following is an essay concerning Mr. Mario’s advance care plan.
Initiating the conversation on advanced care planning
This conversation is meant to discuss with a patient the method and means he would like to be treated or taken care with once he or she falls seriously ill and he is not able to make such decisions then. Usually, this conversation is started when it is clear that a patient’s health risk is very high and so is the case with Mario. The conversation on advanced care planning with Mario should have been initiated after being told by the oncologist that the chemotherapy was unlikely to be ineffective and that is the same period when he decided that he would focus on the time he has with his family. During the initiating of the conversation, it is important to explain to Mr. Mario what the conversation is all about and the importance. It is after this that he should then be asked if there is anyone who he thinks should be present during the conversation. This should then be followed by the deliberate allowing of time so as to provide the patient with an opportunity to reflect. (Yeung, Escalante & Gagel, 2009, pg.46)
After that, the conversation can then begin and this must be done by using words not too insensitive to the patient for example, ‘I would like to discuss with you about your wishes of future care in case you get very sick which might not happen but just in case it does you will not be able to express your wishes and at that point it would be very important to know what you would have wanted’, ‘Have you considered about the place or type of care you would want to have in case you became too sick to take care of yourself?’ or ‘most people usually think about what they may want in the future and they usually have their wishes drafted in a document called Advance Health Directive. Would you like to know more about this Advance Health Directive?’
Preparing for the conversation
There are some very important issues that should be taken into consideration in preparation of the advance care planning discussion and this is mostly so as to protect and maintain the welfare of the patient and this are as follows
Firstly, one should review all medical files notes or files of the patient. This is meant to ensure that all that all the relevant and critical clinical information concerning the patient are available. The same can still be achieved through consulting other medical care experts involved with the patient. (Goldstein & Morrison, 2013, pg 273)
Secondly, the health care professional should also ensure that he or she has a private and comfortable area to carry out the discussion. This area should be free from interruptions from anyone. This will help in boosting concentration while collecting all the necessary information. In addition to finding a private area, one should determine if there is a family member who can participate in the discussion. This family member should be a very close family member. This can be determined through scrutinizing the patients’ health and personal documents.
Moreover, it should be made sure that the patient is in a mental capacity to participate in the discussion. This is so because the patient, if not in the capacity to discuss these matters, can easily fall into a depression. If there is a family member participating in the discussion, the same should also be made sure to avoid any cases of afterwards depression. Chambers, Germain & Brown, 2010, pg55)
One should ensure that he or she has drafted a structure that will be used during the advanced care planning process. This can be achieved for example, through having a structure that contains leading question. The draft structure should be able to contain the following components;
it should lead one in identifying the goals, advantages and disadvantages of the methods and interventions that the patient would want sought
it should be able to ensure that the patient knows the level of seriousness of his stage four pancreatic cancer.
It should be able to lead the patient in knowing that his disease is palliative.
It should also be able to identify the patient’s fears or greatest concerns.
It should be able to determine what the patient thinks about the advance care planning.
One should have an understanding and be well conversant with all local laws that concern the drafting and implementation of such critical documentation. One should also ensure that he or she has adequate knowledge on how to access the necessary documents.
Lastly, arrangements for the appropriate support services should be made prior to the initiating of the conversation. Among other things, this support service can be helpful in consoling the patient if he or she gets emotional during the conversation and breaks down.
Who should be involved in the discussion?
An advanced care planning discussion usually involves a patient and it also advisable for very close family member to be present although the consent of the patient will have to be sought first. In the case of Mr. Mario, his close family member is his wife Rosa, so it would be appropriate to involve his wife in the discussion. Both the participants will be required to participate in the discussion through sharing their opinions concerning the advance care plan. Mr. Mario could also choose for his attorney to be present especially if he is interested in transferring his power of attorney to a different person such as Rosa who would be required by the power of attorney to make decisions for his husband when the husband is not in a capacity to do so. Whatever is discussed in the advance care plan is then documented which will make it easy to use for future references. The wishes are then legalized through filling out legal forms entailing all your wishes. This can be done with the help of an attorney although it is not necessary. (Noogle, 2012, pg 57)
Information to be included in the advance care plan
There are issues that should be included in an advance care plan. For an effective outcome, this should mostly be in the form of questions. The issues to be addressed should be as follows;
Firstly, there should be goals, advantages and disadvantages of any interventions that might be required when taking care of the patient. These goals may include decisions of emergency treatments to keep the patient alive such cardiopulmonary resuscitation (CPR) which is meant to restore the heartbeat if it stops, comfort care which involves relieving pain, artificial nutrition or artificial hydration which are meant to provide nutrition to the patient through a tube when the patient is unable eat or drink. This is meant to ensure that Mr. Mario fully understands the consequences of any method before preferring for it to be used in the advance care plan. (Thomas & Lobo, 2011, pg 239)
Secondly, the plan should be able to address the patients preferred place for receiving future care and this is meant to ensure that the patient is comfortable in receiving this care for example; this could be asked as ‘where would you prefer to receive future care?’
Although not necessary, the patient should be given the opportunity to decide whether he would like to donate any organ or tissue in case of death and the question asked could be; ‘incase of death, would you like to donate any of your body organ or tissue? If so where or to whom would you want the above stated organ or tissue donated?’ (Vadivelu, Kaye & Berger, 2013, pg 100).
The advance care plan should be able to make sure that the patient and his wife are aware of the extent of seriousness and risk of his pancreatic cancer. This is one of the means of ensuring that the participants are in the right mental capacity to get involved in the discussion. For example, this could be asked in the form; ‘are you aware of the extent of risk of your level four pancreatic cancer? If so what do you think are the risks involved?’
The care plan should be able to inquire from the patient the people he would like to make decisions for them in case they are unable to make these decisions. The care plan should still be able to inquire if the patient has shared his wishes with his family or friends. This could be in the form; ‘Incase your are not able to make any decision, whom would you like to act in your capacity in making these decisions? Apart from your wife, have you informed any other family member or friend of your wishes?’
The plan should be able to diagnose Mr. Mario’s gravest and deepest fears concerning his pancreatic cancer. The same should also be inquired from his wife, Rosa. For example this could be asked as ‘what are your deepest fears concerning this disease?’
Lastly, the advance care plan should give Mr. Mario or his wife the opportunity to ask any question related to Mr. Mario’s health that might have not been addressed in the care plan. This could be asked as ‘Is there any other issue concerning the disease that you would want addressed here?’
Reviewing of the advance care plan
This involves the revisiting of the advance care plan discussions and at times the decisions set out in the advance care plan can be changed. It is usually advisable for the reviewing to be done regularly due to a number of reasons which can apply in Mr. Mario’s case. The following are the main reasons for reviewing the plan or circumstances that might trigger the reviewing process
Firstly, Mr. Mario or his wife could request for the reviewing or change their mind about a decision that they had made earlier this might for example, be triggered by the infeasibility of an option that they had recommended maybe due financial constraints or a number of other issues.
Secondly, there could be a change in circumstances that might require the reviewing of the plan. For example, change in medical conditions whereby a new disease or condition is discovered in the patient. The same could also be triggered by change of individual conditions for example incase Rosa, Mr. Mario’s wife, dies or any other person mentioned in the advance care plan and whose death affects the plan.
Thirdly, the reviewing can be done when Mr. Mario returns to the hospital for example when he is going back for a checkup or when the health care professional visits Mr. Mario at his home. Usually, the reviewing of the plans is usually set to be done constantly and in such cases the reviewing is done when the patient visits the hospital or when the health care professional visits the patient at home. (Hartmann, Loprinzi & Mayo Clinic, 2012, pg 45)
Fourthly, the reviewing can be done if the medical options that are present in the advanced care plan changes the needs of Mr. Mario in regards to the plan for example in the discovering of a co morbidity.
Fifthly, Mr. Mario can revoke the advance care plan any time and this will require the preparation of a new advance care plan. In such a scenario Mr. Mario might view the earlier on plan as not been appropriate due to a number of reasons and this will require him to revoke the care plan and request for the drafting of a new one.
Lastly, during the making of the advance care plan, Mr. Mario can state a review interval of which after the interval time lapses, the making of a new advance care plan will be required. For example, Mr. Mario could state that he would require reviewing the care plan after every two months. After the lapse of these two months, Mr. Mario will then be required to review the care plan.
Activation of the advance care plan
This involves the point and time at which the discussion in the plan will be implemented. In Mr. Mario’s scenario this will take place under the following circumstances.
Firstly, activation can occur if Mr. Mario enters into a comma for example, after he collapses at the shopping centre and becomes non responsive and is taken to the hospital. If he completely fails to respond, then implementation of the care plan will be deemed necessary.
Secondly, the activation can occur in case of Mr. Mario deaths. In this case the advance care plan will be activated in that, if he had requested in the care plan for his body tissue or organ to be donated, then his wish will have to be fulfilled. (Barnsteiner, Disch, Walton & Sigma Theta Tau International, 2014, pg 107)
Thirdly, the activation maybe triggered by the person who has the power of attorney. This involves transferring your rights to make decisions concerning certain issues to another person who is required by law to make decisions that will be in your best personal interests if you are not in a capacity to make these decisions. In this case Mr. Mario could have given this power to his wife Rosa so if by any chance Rosa feels that Mr. Mario is not in a capacity to make decisions then she can ask for the implementation of the advance care plan.
Fourthly, the activation of the care plan can be triggered if Mr. Mario experiences dementia. This is a condition whereby the patient’s mental ability is impaired and cannot make decisions as a reasonable man. In such a case the patient will not be in the right mental capacity to make a reasonable decision so this will require the fulfilling of his wishes as he had earlier on stated in the care plan. (Leah & Susana 2013)
Lastly, the activation can be triggered by a medical condition which will make it impossible for Mr. Mario to communicate his decisions such as stroke or paralysis. In such a condition, the patient might be in good mental capacity to make decisions for himself but the communication of this decision might be difficult hence necessitating the use of his wishes as stated in the advance care plan
In conclusion, an advance care plan plays a very crucial role since it betters the quality of life of the patients, provides medical care which is less aggressive, helps families prepare for the death of a loved one and also helps in resolving family conflicts. (Thomas & Lobo, 2011, pg 78)
References
Oliver, D. (2013). End of life care in neurological disease. London: Springer
Yeung, S.-C. J., Escalante, C. P., & Gagel, R. F. (2009). Medical care of cancer patients. Shelton, Conn: People’s Medical Publishing House.
Goldstein, N. E., & Morrison, R.S. (2013). Evidence-based practice of palliative medicine. Philadelphia: Elsevier/Saunders.
Hartmann, L. C., Loprinzi, C. L., & Mayo Clinic. (2012). The Mayo Clinic breast cancer book. Intercourse, PA: Good Books.
Weis, J,. & Horneber, M. (2014). Cancer related fatigue
Noogle, C. A. (2012). Neuropsychology of cancer and oncology. New York: Springer Pub.
Chambers, E. J., Germain, M., & Brown, E. A. (2010). Supportivecare for the renal patient. Oxford: Oxford University press.
Fischer, S., Gozansky W., Sauaia A., Min S.,Kutner J., Kramer A. (2006). A practical tool to identify patients who may benefit from a palliative approach: the caring criteria Shrewsbury, UK: NHS 285
Thomas, K., & Lobo, B. (2011). Advance care planning in end of life care. Oxford: Oxford University Press.
In Vadivelu, N., In Kaye, A. D., & In Berger, J. M. (2013). Essentials of palliative care.
Melnyk , B. M., & Fineout-Overhault, E. (2011). Evidence based practice in nursing & healthcare: A guide to best practice. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
In Christensen, A. J., In Martin, R., & In Smyth, J. M. (2014). Encyclopedia of health psychology.
In LoBiondo-Wood, G., & In Haber, J. (2014). Nursing research: Methods and criticsl appraisal for evidence-based practice.
Barnsteiner, J. H., Disch, J.M., Walton, M. K., & Sigma Theta Tau International, (2014). Person and family centered care.
Leah, R., & Susana L. M. (2013). Advance care planning: communicating about matters of life and death. New York: Springer Pub.
NOTE: each paragraph is a different question on its own
Paragraph 1 (please provide a minimum of 300 words with 2-in-text APA style reference)
Think of a recent boss you have had. Were they more of a manager or a leader? Was this appropriate for their role? And how did it impact you as a follower?
Paragraph 2 (please provide a minimum of 300 words with 2-in-text APA style reference)
Identify and discuss the six trait characteristics in the trait approach to leadership. If one does not have these traits, can he or she still be a leader? Explain your position.
SAMPLE ANSWER
Paragraph 1
My recent boss, who was the senior health officer in a private health facility, was more of leader and a very effective one and this is because of the traits he possessed such as integrity as was evidenced by the way he was able to account for every cent given to him, intelligence as evidenced by the wise and strategic decisions he used to make concerning the running of the facility, self confidence as was evidenced by the way he used to implement his policies despite receiving criticism from a few people, determination as was evidenced by the way he used to extend his working hours for at least two hours daily and his punctuality in keeping time and finally sociability as was evidenced by the way he used to interact with his subordinates (Ledlow & Coppola, 2011, pg 62).
This was very important in the role he played as the senior officer whose main work was to oversee that the day-to-day operations of the health facility were carried out as required. At the end of the year, the facility was able to get more patients compared to the previous years and most of them commended the facility for its quality services. This had a great impact on me since it helped me appreciate the need of possessing the same traits that is determination, self-confidence and integrity. The appreciation of these traits is what helped me gain the ‘Employee of the Year’ award at the end of the year. (Wiseman & McKeown, 2010, pg 15)
Paragraph 2
For a leader to be effective according to the trait approach should posses some traits and this is as follows;
Intelligence
Research done has shown that leaders have a relatively higher intelligence compared to non-leaders. Intelligence is what boosts communication skills, problem solving skills and reasoning skills of these leaders. However, it has been shown that the intelligence quotient of leaders and their subordinates should not differ much since this can make it difficult for the subordinates to comprehend ideas from their leaders and also hinder the communication between the two. (Northhouse, 2004, pg 20)
Self confidence
Self confidence in leaders is important since it boosts one’s self-esteem and this acts as a motivation of aiming at productivity in whatever one does.
Determination
This is very important especially during the times when one is faced with challenges. A determined leader is able to overcome any hurdles or obstacles. Determination also ensures that a project or assignment given is performed to its maximum and such leaders do not settle for mediocrity. This is very important when it comes to producing quality work. (Northhouse, 2004, pg 20)
Integrity
Integrity involves being trustworthy. Leaders with this trait are able to motivate their subordinates to posses the same trait. Research has shown that most of the successful organizations in the world are run by integral leaders compared to some organizations which have collapsed as a result of leaders lacking integrity. Such organizations are usually faced with issues such as corruption. (Northhouse, 2004, pg 21)
Initiative
This is the quality of being able to come up with new ideas. (Gordon, 2002, pg 56) Most of the successful leaders in the world such as Steve Jobs came up with new ideas and this uniqueness is what made them successful.
Sociability
This is the quality of being interactive with other people. This trait usually enhances communication between leaders and their subordinates which is very important in the operation of an organization. (Northhouse, 2004, pg 21)
In conclusion, if one does not possess these traits, he cannot be a leader since leadership is a skill that requires principles to be adhered to so as to ensure that the interests of the people are served. The failure to adhere to these principals will definitely lead to the lack of mutual interest between the leaders and the individuals that are been led and the person leading will no longer be viewed as a leader.
References
Ledlow, G. R., & Coppola, M. N. (2011). Leadership for health professionals: Theory, skills, and applications. Sudbury, Mass: Jones and Barlett.
Wiseman, L., & McKeown, G. (2010). Multipliers: How the best leaders make everyone smarter. New York: HarperBusiness
Gordon, J. R., (2002). Organizational behavior: A diagnostic approach. Upper Saddle River, NJ: Prentice Hall.
Jessica has been feeling unwell for the last 2 days with cold like symptoms, clear discharge from her nose, low grade fever and occassional coughing at night. The following nigh Jessica woke short of breath. Jessica’s mother, Anne , also noticed that Jessica’s breathing was quite noisy.
Anne, Jessica’s mother sat Jessica upright, found her salbutamol puffer and spacer which was on her bedside table and administered six puffs via her spacer as instructed by the asthma nurse at her local GP practice. Jessica’s breathing appeared to settle not long after the puffer and she then went back to sleep.
Anne woke with a start 2 hrs later and rushed to Jessica’s room and found her becoming increasingly short of breath and coughing continuously. Anne gave Jessica a further 6 puffs of salbutamol through her spacer. Jessica’s breathing did not appear to be improving, so Anne decided that they should go to the hospital.
One of Jessica’s cousin is a second year student nurse. He tells you he doesn’t understand the pathophysiology of asthma and how it affects the respiratory system. Jessica’s mother Anne asks you to explain to him the pathophysiology of asthma and how it affects the respiratory system using the correct medical and nursing terminology. You are also to explain two signs and symptoms that the patient Jessica has presented, therefore, shortness of breath and wheezing/coughing and explain why they manifested as part of the illness/disease.
SAMPLE ANSWER
Pathophysiology of Asthma
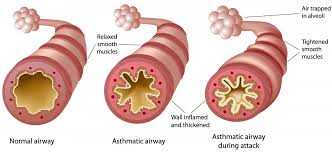
Asthma is a long-lasting inflammatory ailment of the breathing systems. It can be classified in different ways; physiologically, pathologically and bronchoconstriction. Physiologically it can be observed as an adjustable. It can also be partly reversible by blocking of airflow just as in the case of Jessica. Your aunt Anne, following doctor’s instructions used salbutamol puffer and as pacer to reverse the blocked air.
Pathologically it comes with overdeveloped mucus glands and airway thickens due to scarring inflammation and bronchoconstriction and thinning of the respiratory system in the lungs due to the tightening of adjoining soft muscles.It has many symptoms and among them is feeling extreme cold, clear discharge from the nose, low-grade fever and frequently coughing at night. These symptoms of asthma have implications for the diagnosis, management, and potential prevention of the disease (Murphy, 2011, Pg. 78).
Pathophysiology or physiopathology is a word that is formed by the combination of two words;pathology and physiology. Pathology is a medical discipline that is used to explain conditions that are initially seen during a disease and in this case, Jessica’s ailment, On the other hand, physiology is the biological word for defining procedures or methods which operate within a person. Pathology has always been used to describe the irregular or undesired disorder. On the other hand, pathophysiology tries to explain the physiological processes or mechanisms in which such a condition grows and advances. (Marthan., R, et al. 2014, pg. 153)
Pathophysiology is also used to mean the functional variations related with or resulting from illness or injury. Lastly, it can also be defined as the practical changes that accompany a specific disease.
How it affects the respiratory system
During an asthma incident, swollen breathing system react to environmental activates such as smoke, dust, or pollen. The airways become narrow due to excess mucus, these makes breathing difficult. In essence, asthma is the result of a resilient response in the bronchial airways (Loo, 2009, Pg. 67). The airways of asthma patients are oversensitive to certain activates, also known as stimuli. In response to exposure to these triggers, the bronchi having large airways contract into spasm that is an attack by asthma. Further Inflammation leads to further narrowing of the breathing system due to excessive mucus that is produced. This causes coughing and other breathing difficulties. Bronchospasm may resolve impulsively in a period of two hours, or in about half of the subjects, may become part of a delayed response.
This initial insult is followed three to twelve hours later with further bronchoconstriction and inflammation.The normal ability of the bronchus is usually maintained by a stable operative found in the autonomic anxious system. Both of them function involuntarily. The parasympathetic impulse circle having afferent nerve finales that originates underneath the inner linings of the bronchus. Whenever these afferent nerve endings are stimulated by different things such as dust, cold air or fumes, impulses travel to the brain-stem called the vagal center, and then it moves down the vagal efferent pathway up to the bronchial small breathing system (Harver & Kotses, 2010, pg. 585). When it reaches here acetylcholine is released from the afferent nerve endings which results in the extreme creation of inositol one, four and 5-trisphosphate (IP3) in the bronchial smooth muscle cells which lead to muscle shortening and this initiates bronchoconstriction that brings the chest problems of difficulty in breathing that is called asthma (Murphy, 2011, pg. 46).
Shortness of breath in asthma and its manifestation
Asthma is a lifetime ailment that makes someone’s lungs hypersensitive and hard to breathe. It is an incurable disease, but with right treatment, people with asthma can lead healthy, active lives. Shortness of breath is a feeling whereby you get a dyspnea. Dyspnea is having a difficulty in breathing. If one has asthma, their breathing passages are highly sensitive. Some things can thereby make their respiratory system encounter some problems. One of the problems faced is swollen and blocked airways. This is as a result of excessive mucus. The swelling and mucus make the respiratory system narrow. This causes difficulty in breathing. This is one of the primary signs of an asthma patient even before diagnosis is carried out (Wolfson & Montgomery-Downs, 2013, Pg. 751). Other symptoms of asthma include wheezing, chest tightness and chronic cough as in the case of Jessica.There is no medical terminology for shortness of breath. Asthma patients will frequently describe this trouble of breathing in different ways. While others call it unable to catch my breath, others call it gasping for breath. (WebMD. 2015)
Wheezing and in asthma and its manifestation
These are some of the most common asthma symptoms and are often the purpose why many people look out for care. Wheezing makes a patient produce a high-pitched sound during respiration. Mostly, it occurs when he patient breaths out but can also be heard when they breath in. The narrowing of the respiratory passages due to inflammation is the primary cause of wheezing.
References
Marthan., R, et al. 2014. Pathophysiology of asthma. Europe Pub Med CenteMorris., J, et al.2015. Asthma. Medscape
WebMD. 2015. Symptoms of Asthma. Medical Health Center.Viewed at www.webmd.com 25/05/2015
Murphy, W. B. (2011). Asthma. Minneapolis, MN: Twenty-First Century Books.
Wolfson, A. R., & Montgomery-Downs, H. (2013). The Oxford handbook of infant, child, and adolescent sleep and behavior.
Loo, M. (2009). Integrative medicine for children. St. Louis, Mo: Saunders/Elsevier.
Harver, A., & Kotses, H. (2010). Asthma, health, and society: A public health perspective. New York: Springer.
We can write this or a similar paper for you! Simply fill the order form!
Situational Approach and Contingency Model of Leadership
Situational Approach and Contingency Model of Leadership: A Tale of Two Coaches
Order Instructions:
Write a 500-750-word paper that analyzes the two leadership case studies found in topic materials for this module, “Coach Knight: A Will to Win” and “Coach K: A Matter of the Heart.”
Address the following questions and concepts:
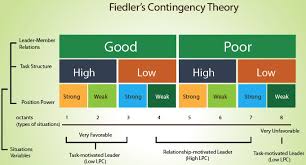
Through your review of Fiedler’s contingency model, would you say that the coaches are matched to their situation? Why or why not? Has this had an impact on their effectiveness?
Provide evidence from the cases that show whether or not there is usage of the leadership styles by the two coaches, and adopt a position on whether or not you think the coaches are effective from this theoretical perspective.
Prepare this assignment according to the APA guidelines found in the APA Style Guide
SAMPLE ANSWER
Situational Approach and Contingency Model of Leadership: A Tale of Two Coaches
The contingency theory proposes that leaders base their style on prevailing situations. The theory classifies leaders into two classes. In the first category, leaders focus on task completion while in the second, they aim at building relationships with their subjects. The theory suggests that the best approach that leaders should take must fit their situations (Advise America, 2015). In his theory, Fiedler expressed leadership as fixed and measurable. Leaders can assess their qualities by evaluating their preference for both relationships and task completion (Schriesheim& Neider, 2012, Pg. 451).
Considering the contingency theory, the two managers adopted different leadership styles to fit their situations. Coach Knight for instance had to intimidate his players and push them to work harder, as he wanted to grab quick wins. By using dictatorial means, the coach made his players work hard and give no room to defeat. Though the method was not favorable for the players, the team was successful in most cases. Coach Knight was focused on winning, rather than enhancing his relationship with the players. He ensured that his players were disciplined through intimidation. The players adapted to his method by pursuing perfection, making them always determined to win. While his subjects could have disliked him for his dictatorship, they ended up liking him as he helped them achieve. In addition, the coach earned respect from the players through his style.
Coach K on the other hand focused on relationships with his players. His method was no less effective as he still registered high scores with his team. Coach K took an approach most preferred by managers in organizations. By pursuing relationships, the manager allowed his subjects to exercise self-drive, and ended up winning in most cases.Just like Coach Knight, his method was effective and appropriate for his situation.
According to the theory of contingency, leaders can either focus on relationship or task completion. Coach K focused on relationship, and hence exercised his leadership role. Coach Knight on the other hand focused on task completion, and just like Coach K, he performed his leadership duties.Coach K, for instance, associated with his players to strengthen his bond with them. He could even join them in activities outside the pitch, hence creating an interactive environment. He made his player free to express their views so that they could developed their own common goal. As a leader, he gained more influence by winning the trust of his subjects. The players could feel that he was part of them even when they were playing. The structure he created in his team was strong and players could automatically focus on winning.
On his side, Coach Knight maintained a power-oriented position in his team. Relationships were never his considerations, and he directly approached the core objective of his career; winning. when leaders adopt power, workers are likely to comply as followers (Wart, 2014, Pg. 160). By assuming a dictatorial approach, the coach forced the players to pursue excellence. It is an important responsibility for leaders to guide their subjects. In the authoritative mode of governance, leaders expect that employees work within the provided guidelines.
Conclusion
The theory of situational leadership significantly describes the styles taken by the two coaches. Though the two vectored in most situations, Coach K used a better style. While his counterpart’s style hurt the players’ emotions in some situations, Coach K’s method was encouraging and friendly. He not only attained victory, but also maintained good interactions with the players. With his strategies, Coach Knight achieved at the expense of relationship with his players.
The advancement of leadership and the development of leaders seem to concentrate more on training through investigation of theory or literature.
According to the attached article, why is this ineffective?
Evaluate the appropriateness of such a training focus.
Based on your other readings, what other elements may be included to increase the self-knowledge and effectiveness of leadership?
Each of the following conditions must meet the essay:
1)The answer must raise appropriate critical questions.
2)The answer must include examples from aviation experience or the web with references from relevant examples from real aviation companies. I prefer example from Qatar Airways, Etihad airline, Emirates airline, Al Arabia Airline.
3)Do include all your references, as per the Harvard Referencing System.
4)Please don’t use Wikipedia web site.
5)I need examples from peer reviewed articles or researches.
Note: To prepare for this essay please read the required articles that is attached
Best regards
SAMPLE ANSWER
Effective leadership
Introduction
There has been a tendency of advancement of leadership and the development of leaders concentrating more on training through investigation of theory or literature. This approach is associated with certain drawbacks which altogether fail to produce effective leaders. The following discussion will engage in reviewing some of the limitations on this form of training. In addition, the paper will examine how self-knowledge and effective leadership can be pronounced in a company.
Discussion
The advancement of leadership and the improvement of leaders seem to concentrate more on training through investigation of theory or literature. This is ineffective due to a number of reasons. One of the explanations is that assortment of aspirants to join training is mostly uncertain. This is because most firm targets the familiar aspirations of those employees who chase to rise to leadership situation. Therefore, getting a suitable sample of candidates to train to be converted into leaders is ineffective as every employee wants to become a leader as that status has power, reputation, and increased income (Taylor 2012). At Etihad Airline, for instance, CEOs find it hard to pick up prospective aspirants to be future leaders at the company when they step down. The training has also some elements of ineffectiveness as it mainly covers on reinforcing self esteem of candidates. However, in doing so, it does not give long-term adjustments in their consciousness or conduct. This is witnessed by the actions of the graduates retreating back to their old ways of doing things as rudimentary behavioral transformation lack due to the training unable to provide the graduates an environment and time required to reshape behavior.
Another noted reason why this form of training is ineffective is because it is mainly grounded in teaching the candidates about leadership, providing them cognitive experience, and infusing new leadership models to them. This is quite similar to a teaching guide (O’ Connell 2011, p.339). Therefore, it calls for experimentation and learning, followed by simultaneous recurrence of a dedicated practice. The training also lacks a metric for evaluating leadership appropriateness. This form of training fails to give consensus on who a leader is or what are responsibilities of a leader (Bérard 2013). There is loss of connection between empirical correlation and leadership performance with leadership outcomes and qualities. It is being found that the case histories only try to buttress current mythologies. At Qatar Airways, for instance, line managers find it difficult to deal with the leadership wrangles at the Gulf area in dealing with high competition due to the action of clinging to traditional methodologies of dealing with HR emerging problems. .
It is also noted that despite many ineffectiveness of training though investigation of theory or literature, there is a number of appropriateness derived from that form of training. Notably, candidates in the training program do buff up specific skills, particularly in communication networks (Adle, Kwon & Heckscher 2008, p. 361). Effectiveness resulting from such program is that that training may challenge the candidates or reinforces their self esteem. For instance, Emirates Airline working with its subsidiaries provides a platform where various leaders of the subsidiaries meet to share experiences (Connell 2011). This is mainly by intensifying candidates’ awareness of the behavioral inclinations in their ways and psyche. Consequently, candidates are given cognitive experience by these training programs, that is, the hopeful leaders are taught about leadership, latest leadership paradigms, offered with historical consideration on leadership theory, and being offered with a record of leadership desirable qualities.
There are some factors that may be included to enhance self-knowledge and effectiveness of leadership. Empathy is one of the critical fundamentals that should be embraced to enlarge self-knowledge and effectiveness of leadership. Empathy emphasizes the leadership with the ability to improve juniors, challenge those who act unfairly in a firm, and provision of constructive feedback. Social skills also come under components to electrify self-knowledge. An effective leader should be oriented to mechanisms to which he or she can learn how to not sit back and make their juniors do the work Grimme 2011, p.482). This factor can be continual actions of a leader to congratulate employees to inspire the loyalty of the team. Leaders at Emirates Airways engage in giving their subordinates gift and bonuses to boost their urge in fulfilling the objectives of this respective airline. Learning conflict resolution skills is also important under the elements of social skills as the leader will be able to be trained to arbitrate wide-ranging conflicts occurring in the line of duty. To develop self-knowledge and effective leadership it can be done through learning challenges. Trial and error makes leaders better in their roles through learning from their failures and successes.
Selecting the right candidate for the leadership position is one of the crucial factors for an effective leadership. Through strong motivation, a leader develops his or her self knowledge by being motivated by a strong embebbled urge for the sake of achievement. The type of leaders oriented to this element is able to explore new approaches to their duties. It is interesting to find out that these types of leaders keep score by tracking such complicated measures as market share, for instance, money manager at Qatar Airways gauge the performance of his stock fund aligned with Etihad airline, Emirates airline, Al Arabia
Airline (O’ Connell 2011, p.340). Even when the score is against them, highly motivated leaders will continue to remain optimistic. In such process another element of self-regulation comes in to merge with achievement motivation to enable frustrations and agony that can be felt from such failures. It is being observed that at Etihad Airways, portfolio managers are not fired when a failure occurs at their line of duty. Rather, the company elevates them to senior position where they will be given an opportunity to prove that they can lead a turnaround (O’ Connell 2011). Self-regulation makes effective leaders abandon the habit of attacking others verbally, stereotyping others, and to compromise their values. This form of self-knowledge is brought in by the tendency of the leader to know his or her values and hold him/herself accountable incase of mistakes. Leader’s own reflection falls under some of the elements to be included to increase leadership effectiveness and self-knowledge. Most of the managers at Etihad Airline meet severally in a year to discus what each of them encountered during that financial period, and the mechanism as well as strategies to handle the situation (Grimme 2011, p.487). Through this reflection, a leader is supposed to learn from the mistakes of other leaders. Learning from experience of peers who face analogous leadership problems can be an important factor to effective leadership and self-knowledge development.
Conclusion
In summary, effective leadership is derived if leaders are oriented to harsh crucible organizational experience. Training through investigation of theory or literature is pragmatically teaching of which it should be learned. Upon making better leaders, they should be given an environment where they will acquire self-knowledge to enable them run the operations of a company efficiently.
Reference list
ADLER, P.S., KWON, S-W. AND HECKSCHER, C. (2008). Professional work: the emergence of collaborative community. Organization Science, March–April, 19(2): 359–76
ANDERSON, R., & BRAUD, W. (2011). Transforming self and others through research: transpersonal research methods and skills for the human sciences and humanities. Albany, State University of New York Press.
BÉRARD, J. (2013). Accelerating leadership development: practical solutions for building your organization’s potential. http://site.ebrary.com/id/10740165.
GRIMME, W. (2011). The Growth of ailine global alliances: an empirical assessment of the perceptions of business travelers. Transportation Research part A, 37,479-497.
O’ CONNELL, J. (2011). The rise of the Arabian Gulf carriers: An insight into the business model of Emirates Airline. Journal of Air Transport Management, 17, 339-346.
ODONI, A. (2009). The international institutional and Regulatory Environment 9Chaoter @). In P. Belobaba, A. Odoni, & C. Barnhart, The Global Airline Industry. John Wilesy & Sons, Ltd. ISBN: 978-0-470-74077-4.
Write a 500-750-word paper that analyzes the two leadership case studies found in the topic materials for this module, “Coach Knight: A Will to Win” and “Coach K: A Matter of the Heart.”
Address the following questions and concepts:
1.Which of the leadership perspectives discussed in Week 1 do you think is manifested in both coaches? What are the power bases both coaches rely upon? Whose actions are more aligned with a managerial role and whose actions are more aligned with a leadership role?
2.How significant were their respective traits in influencing their leadership? The textbook provides a list of traits and links these with the five-factor personality model. Is there an agreement between the traits you have identified and those presented in your text? In what ways has this affected the performance effectiveness of the coaches?
Prepare this assignment according to the APA guidelines found in the APA Style Guide
SAMPLE ANSWER
Leadership as a Process: A Tale of Two Coaches
Leadership often determines the success attained by managers and their organizations at large. The most suitable style of leadership is subjective and varies with situations. There are many leadership strategies, all of which could lead to achievement of goals. Coaches Bobby Knight and Mike Krzyzewski (Coach K) were both successful basketball managers. While Krzyzewski was an assistant to Knight at one time of his career, he never adopted Knight’s leadership style. He took a perspective that differed completely from that of his former senior. The effectiveness of either of the two coaches as a leader is a subject of interest when studying leadership in organizations. Studying the two coaches reveal that two different ways can lead to the same outcome. However, it is important to evaluate the extent of success each achieved, to understand which style is most appropriate.
Coach K was soft on his players and made mainly exploited peaceful means of interactions. He exercised his powers in a democratic way. His players could link with him emotionally and hence the parties could relate harmoniously. The players could talk to him freely and in most cases they participated in decision making. He natured strong bonds with his juniors and was eventually successful. By exercising an interactive leadership style, Coach K was an authentic manager. From a managerial perspective, his leadership was mostly unquestionable. Focusing on management rather than leadership as manifested by Coach K, can create healthy relationships between the seniors and their juniors. People feel motivated when they associate with their leaders (Bednarz, 2012). In most cases, the type of leadership is more successful than other types where employees keep distance from their employers. With a friendly relationship, problems are easy to identify and solve. Again, the coordination is likely to develop and the challenges could be solved in the most appropriate ways. However, leaders should be keen to ensure that being too soft on employees does not make them lazy. Naturally, when workers feel too secure from their leaders, they are unlikely to be aggressive with their duties.
Coach Knight, on the other hand, used his position to exercise power as a leader. He dictated what he wanted his players to do and no room was there for discussions. By setting objectives and forcing his players to work toward them, Knight made great achievements. His style was more of a leader than that of a manager. Though he valued advisors, he made most decisions alone (Conner, 2014). His players had little to say regarding his management and he could not cultivate a cordial relationship with them. Though the leadership style is effective in some situations, it has high chances of failing. Dictatorship often discourages self-drive and workers are likely to feel uncomfortable. However, the method can be the most appropriate for results that are realized within a short period of time. For Coach Knight, it was most effective as he focused mainly on the then current games. As time goes by, the players could get less productive as they lacked positive motivation from the leadership.
For both, coaches, their styles suited their situations. Coach K could associate with his players and win while Coach Knight could dissociate from his players and still realize good results. Though they used different styles, both coaches were great leaders. On the 5-factor Personality Model, both were outgoing for extravasation, efficient for conscientiousness, and inventive for openness. However, while Coach K is compassionate, Coach Knight is detached. Again, Coach K is confident but Coach Knight is insecure. From a leadership perspective, Coach knight was more successful than Coach K. on the other hand, Coach K was more successful as a manager than Coach Knight. Performance for the two coaches was affected by their personalities. While Coach K could attain results with ease, Coach Knight had to use too much energy. In his managerial position, the former was more relaxed than the latter.
Guidelines : Only Text Referencing at the last page but make sure in APA 6th Edition Format
No Wikipedia or better health reference……….. only books journal and govt. web pages referencing
SAMPLE ANSWER
Dissociative Disorders
Dissociative is the adjective of the noun dissociation and the verb dissociate. From the medical perspective, Merriam Webster Dictionary defined dissociation as separation of personalities. Dissociation could occur at the level of character segments or specific mental processes from the current state of consciousness or behavior (2015, “Dissociation”). If something is dissociative, it has the characteristic of disconnection from other parts.
National Alliance for Mental Illnesses (NAMI) explained that patients of dissociative disorder disconnect from the reality. They lose their thoughts and identity, as well as consciousness and memory (2015). The abnormalities incapacitate the mental abilities of the affected. They are prevalent in all populations regardless of ethnicity, geographical regions, socioeconomic status or any other variations. NAMI pointed out that approximately 2% of the States’ population experiences the disorder. However, mild episodes of the diseases affect half of the Americans at least once in their lives. Gender influences the occurrence of the illnesses, and females are more prone to them than males (2015).Dissociativedisorder accounts for a significant percentage of the few psychiatric problems among the American population.
Signs and Symptom
In most cases, signs of dissociative disorder appear after exposure to physical or mental trauma. War and accidents are major inducers of the symptoms. Victims progressively exhibit deteriorating mental health characterized by stressful moments. Though signs and symptom vary with the specific type of the disorders, stress is a common characteristic of all types. Other common signs and symptoms as NAMI outlined include out-of-body feelings, where patients fail to understand themselves. Patients also fail to develop self-identity, emotional availability, and reliable memories.Usually, people develop anxiety and depression, and they are likely to contemplate suicide (2015).Generally, mental torture is the predominant symptom of the disorder.
Types of Dissociative Disorders
In its DSM-5 manual, the American Psychiatric Association split dissociative disorder into three categories. The three are Dissociative Identity Disorder (DID), Dissociative Amnesia, and Depersonalization Disorder. Some psychiatrists, however, identify two more types of the disorder. The additional two are Dissociative Fugue and the unspecified Dissociative Disorder.Since Dissociative Fugue has most properties seen in Dissociative Amnesia, psychiatrists often classify it under the latter (Spiegel, Fernandez, Lanius, Vermetten, Simeon, & Friedman, 2013, Pg. 299). Different types of the disorder have varied severity of symptoms, as well as thenature of their stressors (Steinberg, 2015).
Dissociative Identity Disorder
DID was commonly referred to as multiple personality disorderuntil recently. The disease mainly traces origin from childhood exposure to physical, sexual or emotional abuse. People exhibit more than one distinctive character. The affected people can assume different behavior and thoughts with time. They easily lose memories about self and experience severe mood swings. Also, patients could have attention deficit disorder impairing their ability to learn.
Diagnoses and Intervention for DID
DID is the severest of the five types of dissociative disorder. Its detection and diagnosis require specialized tests and examinations. As Steinberg explained, hidden symptoms characterize DID, and anxiety, depression or substance abuse could mask the symptoms. Again it is hard to describe the symptomatic disconnection feeling that occur with the disease (2015). The nature of the disease, therefore, makes it hard to diagnose. Psychotherapy is the first-line treatment for the disorder though medication could as well be used.
Dissociative Amnesia
Patients with dissociative amnesia suffer severe inability to recall their personal information. The brain does not have to be necessarily damaged for the condition to occur (Kikuchi, Fujii, Abe, Suzuki, Takaqi, Mukiqura, & Mori, 2010, Pg. 602) In most cases as Steinberg wrote, a single traumatic event is sufficient to cause the disorder. Experiences of disasters, violence and war are the major inducers of the disease (2015).
Diagnoses and intervention of Dissociative Amnesia
When signs of the disorder are present, the examiner would perform physical tests to close out other possible causes of the symptoms, and zero into dissociative amnesia. Treatment is crucial to help individuals restore their memories. Psychotherapy, cognitive therapy as well as medication are the commonest approaches to the problem (Goldberg, 2014, Pg. 2).
Depersonalization Disorder
Patients of depersonalization disorder experience unreal sensations. Their mind seems out of touch with their bodies. The ill cannot connect to the reality and feel as though they are dreaming. Complications of the condition are accompanied by moments of derealization. Again, depersonalization traces origin from trauma and stress.
Diagnoses and intervention of depersonalization disorder
To diagnose depersonalization, physicians perform examinations such as blood tests. Though highly prevalent, the condition is often misdiagnosed (Reutens, Nielsen, &Sachdev, 2010, Pg. 278). Drugs used with psychological counseling to manage depersonalization include clonazepam, fluoxetine and clomipramine (Mayo Clinic Staff, 2014, Pg. 8).
Support for Dissociative Disorder Patients
Patients require assistant to cope with mental instabilities created by dissociative disorder. As Halter and Varcarolis pointed out, victims of the disorder require education on best ways of managing their situation. Nurses could for instance explain to the patients that the diseases result as an adaptive means to experiences (2013, Pg. 319). People associating with the sick should treat them with care to avoid inducing more emotional stress. The patients are emotionally delicate, and they can react strangely to unfriendly stimuli. Nurses and other care givers should offer emotional availability, especially when patients recall the events that traumatized them (Varcarolis& Halter, 2012, Pg. 205).
Spiegel, D, Loewenstein, R. J., Fernandez, R., Sar, V., Simeon, D., Vermetten, E., . . .Dell, P. F. (2011). Dissociative Disorders in DSM-5. NCBI, 28(2011), 824-852
Main Assignment Questions (90% of unit weighting)
AR 50345
The objective of the course work is to demonstrate an understanding of the acoustic principles discussed during the unit week. This can be done in the form of mathematical analysis, an essay style answer or as bullet points. Marks against each section are
indicated as are word lengths, as appropriate.
Q1 a) Please outline your understanding of the following acoustic terms, (using 50 to 100 words each). Credit will be given for each key requirement or unique feature included. Additionally, please indicate where each of these terms are used in the field of acoustics: (10 marks)
Free field
Diffused field
dB
dBA
NR
W-weighting
Rw
R
0
w
(apparent sound reduction)
Dw
Dn
T
w
b) Please provide both a hand calculation and excel spread sheet
calculating the following.
(15 marks)
dBA for the following spectra:
32Hz 64Hz 125Hz 250Hz 500Hz 1kHz 2kHz 4kHz 8kHz
30 30 30 – – – – – — – – 30 35 36 50 36 35
65 83 90 75 43 35 – – — 10 10 10 10 10 10 10 -NR:
32Hz 64Hz 125Hz 250Hz 500Hz 1kHz 2kHz 4kHz 8kHz
30 30 30 – – – – – — – – 30 35 36 50 36 35
65 83 90 75 43 35 – – — 10 10 10 10 10 10 10 -Rw
(spread sheet only) for the following spectra:
125Hz 250Hz 500Hz 1kHz 2kHz
16 24 33 42 43
39 44 56 67 74
38 37 48 64 78
34 39 51 60 68
2 of 4 AR50345
Q2 a) Please explain, or undertake mathematically, how one determines
the composite sound reduction of the following two elements. The area of element 1 should be taken as 9m 2 with an Rw of 40dB.
The second element has an area of 2m 2 and an R w of 30dB.
(5 marks)
b) Use the above explanation to show how the 10dB rule works, i.e.
“There is no benefit in increasing the sound reduction of the larger element more than 10 dB over the smaller element which has a lesser sound reduction.” (5 marks)
Q3 a) Calculate the sound reduction of a facade comprising of: (6 marks)
10m 2 of glass/windows 20m 2 of brickwork and a 5m
2 spandrel panel
The area of the room should be taken as 200m 2
. The reverberation time in this room is equal to 0.7 seconds. Please state the sound reduction used for each element making up the facade and the source of this information.
b) Repeat this exercise but now include a plot of the combined sound reduction when an open window is placed in the facade.
This window has an effective open area of 1m by 0.01m; this window is then further opened in increments to a final effective open area of 1mby 0.25m. The area of the window should be taken out of the glazed element within the facade. (4 marks)
Q4 Sustainability and Acoustics. (20 marks)
Acoustics and sustainability are not often referred to in tandem. On the other hand, it has been shown that there are many links between these two subjects. Please provide your thoughts with respect to the links between acoustics and sustainable building
design.
Please also provide a review of products which are available to enhance the acoustic performance of a vented facade. This information can also be complemented with acoustics details relating to cross ventilation. (500 words) 3 of 4 AR50345
Q5 Reverberation time calculation. (15 marks)
Compose an Excel spreadsheet that calculates the absorption coefficient of the sound absorbing panels in the East Building classroom from 125 Hz to 4000 Hz (octave bands). To do this you should use the test data from the practical session for the empty room (with tables and chairs removed). This data is as follows:
Octave Band Centre Frequency, Hz
125 250 500 1000 2000 4000
Measured Average RT Empty
(Seconds)
0.9 0.8 0.9 0.7 0.7 0.6
The room dimensions may be taken as 13.2W x 5.2D x 3.2H.
There are 65 absorptive panels each with an area of 0.45mx 0.6m. You will need to estimate the absorption coefficients for the other surfaces (e.g. carpet, concrete soffit, glass facade, studwork
walls and doors and use these to calculate the absorption coefficient of the panels. What effect would distributing the panels throughout the room have compared with locating the panels in one large area?
Q6 A building has two items of plant on the roof, (a kitchen extract fan and a kitchen supply fan). The sound power levels of the units are as follows: (20 marks)
Frequency 63Hz 125Hz 250Hz 500Hz 1kHz 2kHz 4kHz
Kitchen Extract 84 85 83 80 78 76 72
Kitchen Supply 76 78 78 75 73 70 68
Calculate the A-weighted sound pressure level (dBA) at the nearest house, which is approximately 25m from the plant. You may assume that the kitchen extract fan is screened by a parapet that just obscures the line of sight. The kitchen supply fan is un-screened. You should clearly identify each step in your calculation or submit a spreadsheet.
SAMPLE ANSWER
Question 1: Part B
dBA for the following spectra:
32 Hz
64 Hz
125 Hz
250 Hz
500 Hz
1 kHz
2 kHz
4 kHz
8 kHz
30
30
30
45
20
30
20
25
25
35
53
60
30
35
30
50
36
35
65
83
90
75
43
35
30
45
55
10
10
10
10
10
10
10
10
10
NR for the following spectra:
32 Hz
64 Hz
125 Hz
250 Hz
500 Hz
1 kHz
2 kHz
4 kHz
8 kHz
30
30
25
35
30
45
20
35
30
30
50
65
30
35
30
50
36
35
65
83
90
75
43
35
25
40
50
10
10
10
10
10
10
10
10
10
Question 2: Part A
The composite sound reduction of two elements can be used using the weighted sound reduction index formula given below:
Where;
D = Level difference
S = Area of the test element through which the noise is transmitted
A = Total sound absorption by the element
Therefore, the composite sound reduction of the two elements can be determined by using the above formulae which can be used to the absorption factors of the two elements given by [ ]. With the absorption factors of the two elements and the average sound pressure of the source and receiving area, the composite sound reduction can be determined for the two elements.
Question 2: Part B
Using the explanation given above it is possible to show that the 10 dB rule works, i.e. “There is no benefit in increasing the sound reduction of the larger element more that 10 dB over the smaller element which has a lesser sound reduction.”
Let’s now consider the parameters of the two elements;
Element 1: Area = 9 m2 and Rw = 40 dB
Element 2: Area = 2 m2 and Rw = 30 dB
The composite sound reduction equation provided above can be used to proof that the 10 dB rule works, by computing the absorption factors for each element, which in the case of these two elements can be calculated from the given details of the two elements. The calculations for absorption factors for the two elements are shown below:
Element 1
Element 2
The above results for the absorption factors of both elements proves the 10 dB rule since their values are close despite the difference of 10 dB between the two elements.
Question 3: Part A
Sound Reduction is given by the formula shown below:
Glass/windows
Brick wall
Spandrel panels
Question 3: Part B
The plot is shown below:
Question 4
Acoustics and sustainability are the two key considerations when designing sustainable or green buildings mainly because both are positively related in terms of the selected specifications, where those of one aspect of a building i.e. acoustics are dependent of the specifications of the building’s sustainability. This is highly attributable to the fact that, acoustics which are majorly concerned with sound insulation have become a very important factor when designing sustainable buildings as our environments continue to become noisier. The reason why acoustic has become a highly influential factor is because sound insulation has a significant impact on the extents of embodied energy in a particular building, which makes it essential to clearly understand the effect of sound insulation on embodied energy levels right from the beginning of the designing of sustainable buildings.
The close connection between acoustic (sound insulation) and sustainability is how the former influences the latter on basis of embodied energy, especially because embodied energy in a particular building can be effectively reduced by re-using an existing building through refurbishments that enables acoustic specifications are fulfilled in a manner that is very cost effective. This is in most cases achieved through timely up front acoustic testing of an existing building to understand its performance prior to refurbishment. Hence, upon establishing the acoustic performance of an existing building as well as understanding its restrictions and limitations, the sustainability of the building can be significantly improved by alleviating these restrictions or limitations.
When designing sustainable buildings, acoustics have become a very significant consideration because it determines the type of materials used in the construction of the sustainable building which is an indication of how the two components i.e. sustainability and acoustics are interrelated. Therefore, early acoustic testing is in most cases carried out as an effective an method to make sure that designs of sustainable buildings are sufficient, and that there is high quality construction in which sustainability is given priority. As a result, the architects usually make decisions of the construction materials to be used in a sustainable building either lightweight or heavyweight materials based of the intended quality of acoustics (sound insulation) as well as its subsequent sustainability. For instance, high/heavy weight materials are in most cases favored for enhanced acoustics; however lightweight materials such as timber often offer better or equal acoustic performance. This means that sustainability of buildings can be improved by using lightweight construction due to their less embodied energy compared to heavyweight construction materials apart from achieving higher levels of acoustic performance do not lead to desired sustainability.
Therefore, as it is theoretically know, a ±6 dB change in acoustic performance or sound insulation is equivalent to a doubling or halving of mass of construction materials for a particular building. This implies that, from the perspective of sustainability when acoustic parameters are over specified there will be an eventual significant impact on the created waste. This indicates that acoustic performance considerations or specifications or parameters in a particular building have a direct impact on its sustainability, hence necessitating the need to always make sure that a balance has been achieved between acoustic and sustainability at the design level of a building.
Furthermore, there are various products that are used for the enhancement of the acoustic of a vented façade. For instance, glass fiber reinforced concrete (GFRC) acoustic panels are one of the products often used in constructing vented facades for enhanced acoustic performance because they not only lead to sound insulation, but also improves sustainability of the building. Mineral wool is the other product used within partitions of vented facades for the purpose of acoustic dampening within stud walls, and it results to significant enhancement in acoustic performance in addition to being sustainable and cost effective method.
Question 5
A copy of the Excel spreadsheet is attached below:
When the absorptive panels are spread throughout the room more sound will be absorbed because they will be in proximity to the source of sound leading to significant sound reduction; however when they are placed in one big area there will be less sound reduction since they will be overlying each other.