Compare/Contrast the worldview of the Religious Right, at the time of its founding, to your current worldview. Your answer must be at least 250 words.
SAMPLE ANSWER
Christian Worldview
With its origin in the early eighties, the Religious Right was initially an amalgam of Evangelical Pentecostals. It initially emerged from the biblical higher criticism in the theological colleges and divinity schools, the teaching of Darwism in public schools system, the existing and or perceived threat of communism. The Religious Right thus includes Catholics, Jews and Mormons who hold very conservative views on politics in addition to the occasional Secularists. This have joined together and taken over the Religious Right. The Religious Right can thus be said to be a the meeting point between the evangelicals with a penchant for politics and were bold enough to politicize the pulpit and the non-evangelicals who saw the opportunity to work with the religious to play politics.
One can thus draw the conclusion that the Religious Right increasingly finds that political goals are the overarching aspects that gel them together. This can be traced to the changes that happened in the early and late 60’s that affected the national psyche – civil rights conflicts, Vietnam protests, the alternative youth culture, the women’s liberation movement, the sexual revolution, and the rise of the new religions (ancient religions emerging from obscurity) (Hansen, 2008). When the glue that joins Religious people together changes from the word of God to politics then society is going down a slippery road – in 1962, the Supreme Court banned prayer and bible reading in schools, legalized first trimester abortion in 1973 and regulated government involvement in private Christian academies.
Presently, the Religious Right is based on four cornerstones; the assumptions, that moral absolutes exists as surely as mathematical or geological absolutes, that metaphysics, morals, politics and mundane customs stand on a continuum, that government’s proper role is to cultivate virtue, and not to obstruct the activities of the marketplace, and that all successful societies need to operate within a framework of common assumptions (Hansen, 2008). This explains why liberals are increasingly major actors in the present Religious Right.
References
Hansen B. S (2008). Religion and Reaction: The Secular Political Challenge to the Religious Right, Rowman & Littlewood Publishers, Inc., Plymouth, UK.
We can write this or a similar paper for you! Simply fill the order form!
Although Canada is contiguous to the United States and has some cultural and historical similarities, Canada’s population enjoys a vastly superior health status. Reasons are many, can be traced historically, and are related to a different view of the role of government. The experience of Canada demonstrates that neither a heterogeneous population, nor a health system that has waiting lines for services, are reasons for poor health. By looking critically at what produces good health in Canada, much can be learned about steps the U.S. might need to take if population health is its goal.
The Canadian Best Practices Portal challenges Canadian public health practitioners and researchers to create upstream interventions aimed at the source of a population health problem or benefit. What is being done to address the influences on population health in Canada?
Search the Internet and scholarly research for examples of Canadian “upstream interventions” that can be put forth as examples of either effective or ineffective efforts to improve population health. This is a 4-5 pages):
The Assignment (4-5 pages):
1. Provide a description of an existing intervention in Canada, intended to improve health inequities. Include an explanation of the inequity and how the intervention targets upstream determinants of health.
2. Describe the organizations involved and/or social policies enacted in the implementation of the intervention.
3.Explain whether or not the intervention was/is successful and what lessons public health practitioners can learn from that experience that might improve population health in the United States.
Articles:
Dinca-Panaitescu, S., Dinca-Panaitescu, M., Bryant, T., Daiski, I., Pilkington, B., & Raphael, D. (2011). Diabetes prevalence and income: Results of the Canadian Community Health Survey. Health Policy, 99(2), 116–123.
Retrieved from the Walden Library databases.
Feeny, D., Kaplan, M. S., Huguet, N., & McFarland, B. H. (2010). Comparing population health in the United States and Canada. Population Health Metrics, 8, 8–18.
Retrieved from the Walden Library databases.
Kirkpatrick, S. I., & McIntyre, L. (2009). The Chief Public Health Officer’s report on health inequalities: What are the implications for public health practitioners and researchers? Canadian Journal of Public Health, 100(2), 93–95.
Retrieved from the Walden Library databases.
Vafaei, A., Rosenberg, M. W. & Pickett, W. (2010). Relationships between income inequality and health: A study on rural and urban regions of Canada. Rural and Remote Health, 10(2), 1430.
Retrieved from the Walden Library databases.
Please apply the Application Assignment Rubric when writing the Paper.
I. Paper should demonstrate an excellent understanding of all of the concepts and key points presented in the texts.
II. Paper provides significant detail including multiple relevant examples, evidence from the readings and other sources, and discerning ideas.
III. Paper should be well organized, uses scholarly tone, follows APA style, uses original writing and proper paraphrasing, contains very few or no writing and/or
spelling errors, and is fully consistent with doctoral level writing style.
IV. Paper should be mostly consistent with doctoral level writing style.
SAMPLE ANSWER
Health inequities are avoidable imbalances that contribute to poor health. Solutions for such inequities may be found in upstream interventions that address social, economic and environmental situations. Social determinants include preventative strategies such as physical activity and proper diet as important ways of preventing chronic diseases and improving overall health (Gore & Kothari, 2012). In Canada, Ontario implements interventions aiming to influence environmental and social factors to address inequities in health.
There is increasing prevalence of chronic disease among certain pockets of the Canadian population. Problems associated with the high cost of treating such diseases necessitate efforts to implement interventions targeting their underlying causes. Canada renewed its commitment to public health in 2003 in a response strategy targeted towards addressing Severe Acute Respiratory Syndrome through healthy living interventions. The associated cost of treating chronic diseases threatens the sustainability of the healthcare system. This realization informs the implementation of a healthy living intervention in Canada through development of chronic diseases prevention guidelines (Gore & Kothari, 2012).
In Canada, low economic social status is measured in terms of literacy and income levels. It determines citizens’ vulnerability to cardiovascular disease, diabetes, asthma and chronic obstructive pulmonary disease (Dinca-Panaitescu, Dinca-Panaitescu, Bryant, Daiski, Pilkington, & Raphael, 2011). Studies show higher prevalence of chronic disease and lower life expectancy in low -income areas as compared to wealthier areas. Research also shows that job insecurity, unemployment, part-time employment and temporary employment negatively affects health as it is associated with elevated levels of chronic diseases such as blood pressure and increased risk of death from cardiovascular diseases. Aborigines, immigrants and people of color also have low incomes and are at higher risks of stress that triggers development of chronic diseases (Gore & Kothari, 2012).
Canada implements health policies aimed at preventing chronic illnesses by addressing upstream causes encompassing lifestyle, socioeconomic and environmental factors. One example of the policies is the 2009 Canadian Cardiovascular Society Guidelines advocating for reduced salt and simple sugars intake. It promotes the replacement of saturated and trans-fats with unsaturated, as well as higher consumption of vegetables and fruits. The guideline also recommends greater attention to weight control to prevent obesity and ensure that more citizens maintain a healthy body weight (Raine, 2010).
Health boards received instructions on the appropriate way to evaluate the population needs and tailor interventions to the groups facing the highest risk. Another policy is the Ontario guidelines for healthy eating and active living that informs various interventions to address health inequities in Ontario (Gore & Kothari, 2012). Aboriginal people and new comers in Canada have a higher prevalence of chronic illness often because of poor nutritional decisions and lack of opportunities for physical exercise. To address inequities among aboriginal people, there is an initiative to provide recreation and fitness equipment and youthful fitness ambassadors in their various locations. Other interventions in the Ontario guidelines for healthy eating and active living include provision for a web and phone based dietitian serving populations in remote areas. It also includes providing fruits and vegetables to schools through partnership with the ministry concerned with agriculture. Efforts to encourage physical activity include collaboration with urban planning designers to ensure that cities promote healthy living and that schools have routes that encourage physical exercise through walking and biking. The local public health units also oversee the compulsory programs and 36 heart health community partnerships to reduce cardiovascular disease (Ministry of Health Promotion, 2006).
The Ontario plan on active and healthy living is also referred to as ACTIVE2010 supports communities to implement community sports and physical activity and nutrition projects (Ministry of Health Promotion, 2006). The plan adopted a multi-sectoral approach targeting the population on a variety of levels. It includes actors from NGOs, private industry, service providers, and communities. Partnership between actors in healthcare is imperative in addressing the wide-ranging impact of social determinants in populations residing in diverse settings (Gore & Kothari, 2012).
The government in Ontario supports the intervention through policies that guide enhanced physical activity in schools, providing access to nutritious foods to children and encouraging hygiene and safety in the environment. Community organizations actively participate through facilitating health promotion trainings to prevent the occurrence of chronic illnesses among at risk individuals. Private companies also participate by creating health and wellness programs for their staff including healthier food choices and exercise. Some companies in the food industry are also keen in providing healthier food selection and creating awareness on the same (Ministry of Health Promotion, 2006).
The physical exercise interventions are tenable and have resulted in substantial benefits to the population. The interventions assist Ontarians to become more physically active through community sports and physical activity projects that are largely supported through the communities in action fund. The implementation of the Ontario’s trail strategy also encourages physical activity through provision of outdoor walking spaces in various areas for all (Ministry of Health Promotion, 2006). In as much as interventions targeting to reduce salt content in packaged and restaurant foods are tenable, the dietary recommendations for preventing chronic diseases remain largely unmet in Canada. Only a few companies have positively responded to the guidelines’ recommendations. The industry progress is underwhelming because many other companies are yet to take voluntary measures to reduce salt in their food products. It shows that regulatory controls are necessary to increase the number of companies acting to reduce sodium levels in processed foods (Raine, 2010).
The Canadian Heart and Health strategy and Action Plan recommends that creating heart friendly environments through education, legislation, and policies aimed at promoting healthy eating and physical activity are efficient interventions in addressing upstream determinants of health. An examination of environment-based interventions to prevent cardiovascular diseases in Ontario and indicates that they failed to address the social causes or determinants of illnesses. Interventions in settings at schools, workplaces, government buildings and communities are insufficient in addressing unfavorable living conditions and factors that create inequity. There is need for greater political will to invest more aggressively in prevention to achieve success (Raine, 2010).
Complete success of the Ontario’s healthy eating and active living plan is dependent upon greater political will to support aggressive implementation including legislative measures. Public health practitioners in the United States must ensure that when adopting such interventions, there is a solid legal foundation to ensure success. The US requires implementing strategies that address health inequities emanating from low-income and racial factors are addressed through population specific measures. A multidisciplinary approach is also imperative in ensuring that communities, government agencies and private sector players coordinate their efforts. There must be enforceable laws on wellness programs, food industry parameters and urban planning. These factors coupled with concerted efforts between public health agencies, education, food and agriculture, companies and the communities provide prime conditions for success.
References
Dinca-Panaitescu, S., Dinca-Panaitescu, M., Bryant, T., Daiski, I., Pilkington, B., & Raphael, D. (2011). Diabetes prevalence and income: Results of the Canadian Community Health Survey. Health Policy, 99(2), 116-123.
Gore, D., & Kothari, A. (2012). Social Determinants of Health in Canada: Are Health Initiatives There Yet? A Policy Analysis. Internatinal Journal for Equity in Health, 11(41), 1-14.
Ministry of Health Promotion. (2006). Ontario’s Action Plan for Healthy Eating and Active Living. Retrieved September 24, 2014, from www.mhp.gov.on.ca: http://www.mhp.gov.on.ca/en/heal/actionplan-EN.pdf
Raine, K. D. (2010). Addressing Poor Nutrition to Promote Heart Health: Moving Upstream. Canadian Journal of Cardiology, 21-24.
We can write this or a similar paper for you! Simply fill the order form!
Identify a theory that can be used to support your proposed solution.
Write a summary (250 words) in which you:
Describe the theory and your rationale for selecting the theory.
Discuss how the theory works to support your proposed solution.
Explain how you will incorporate the theory into your project.
SAMPLE ANSWER
Incorporating Theory
Various theorists have developed different theories to help understand the concept of nursing. The theories aim to add value on nursing to promote quality. One of the theories the paper deliberates on and which supports my proposed solution is Virginia Henderson’s Need Theory.
The theory was developed by Virginia Henderson, who defined nursing as the duty to help individuals, either sick or not, to perform various activities that aids their recovery or helps them to a peaceful death (Wills & McEwen, 2002). These are the activities that the individual may not perform without assistance because the one lacks strength, knowledge, and will. This assistance is essential in helping the patient/individuals to gain independence quickly (Afaf, 1997). Therefore, a nurse has the duty to work with the person, provide needed help, and do some roles for the person to achieve independence.
The reason for choosing this theory is that it expounds the roles of a nurse. Nurses must be able to assist the individuals to enhance recovery, as they require attention to make them strong to stand on their own.
This theory works to support the solution through its various assumptions. One of the assumptions is that nurses provide care to patients until they are in a position to care for themselves (Taylor & Lillis, 2001). The second assumption is that nurses have a desire and are willing to devote themselves night and day to provide care for the patients (Delaune & Ladner, 2002). Therefore, these assumptions and the roles that nurse do jointly enhance the quality of care. Patients must be assisted to make them independent to resume to their normalcy.
One of the reasons why I would incorporate the theory in my practice is that it impacts on the health of the patients. Nurses have a role to help their patients in becoming independent. This is a very important aspect in the field of nursing and nurses must always be committed and dedicated to providing better care to their patients.
References
Afaf, M. (1997). Theoretical Nursing: Development & Progress, 3rd ed. Philadelphia, Lippincott.
Delaune, C., & Ladner, K. (2002). Fundamental of nursing, standard and practice, 2nd edition, Thomson, NY.
Taylor, C., & Lillis, C. (2001). The Art & Science Of Nursing Care, 4th ed. Philadelphia, Lippincott.
Wills, M., & McEwen, M. (2002). Theoretical Basis for Nursing Philadelphia. Lippincott Williams & Wilkins.
We can write this or a similar paper for you! Simply fill the order form!
Consider the population in which the solution is intended, the staff that will participate, and the key contributors that must provide approval and/or support for your project to be implemented. These stakeholders are considered your audience.
Develop an implementation plan (1,500 words). The elements that should be included in your plan are listed below:
Method of obtaining necessary approval(s) and securing support from your organization’s leadership and fellow staff.
Description of current problem, issue, or deficit requiring a change. Hint: If you are proposing a change in current policy, process, or procedure(s) when delivering patient care, describe first the current policy, process, or procedure as a baseline for comparison.
Detailed explanation of proposed solution (new policy, process, procedure, or education to address the problem/deficit).
Rationale for selecting proposed solution.
Evidence from your review of literature in Topic 2 to support your proposed solution and reason for change.
Description of implementation logistics (When and how will the change be integrated into the current organizational structure, culture, and workflow? Who will be responsible for initiating the change, educating staff, and overseeing the implementation process?)
Resources required for implementation: Staff; Educational Materials (pamphlets, handouts, posters, and PowerPoint presentations); Assessment Tools (questionnaires, surveys, pre- and post-tests to assess knowledge of participants at baseline and after intervention); Technology (technology or software needs); Funds (cost of educating staff, printing or producing educational materials, gathering and analyzing data before, during, and following implementation), and staff to initiate, oversee, and evaluate change.
Prepare this assignment according to the APA guidelines found in the APA Style Guide, located in the Student Success Center. An abstract is not required.
SAMPLE ANSWER
Implementation Plan
1.0 Method of obtaining necessary approval and securing support
In essence, for this project to be succeed, support from the key stakeholders including the administration, managers and colleagues at Duke Hospital & Health Center is of great importance. These key stakeholders are important since they have to approve and/or support the project for it to be executed. Together with children patients suffering from Addison’s disease and their parents, the physicians, Registered Nurses (RNs), nurse assistants and the management of the healthcare organization comprise the audiences of this project. Support would be obtained from these key contributors by making clear to them the basis and justification for the proposed solution, as well as the reasons why the proposed change is vital and needed in the health care organization.
The hospital’s managers and leadership, as well as physicians, RNs and assistants would be informed about the value of the change and the way that Duke Hospital & Health Center is going to benefit in consequence of the change. It is of note that the nursing process used in diagnosing and treating patients with Addison’s disease at the hospital has to be reviewed as this will produce results that could be assessed to bring about positive outcomes that will help get rid of the entire condition. The formation of Evidence-Based Practice (EBP) models will help the RNs gain a better understanding of Addison’s disease and recognize how to reduce the continuous stubbornness of the problem (White, 2009). Moreover, engaging the elements of a comprehensive training of RNs will allow them to have an intensive and extensive approach to Addison’s disease. This proposed solution will reduce occurrences of death and/or insanity of the children patients with Addison’s disease since they will be able to contain their stress and depression. Since deaths of children at the hands of the RNs will reduce, the emotional suffering of RNs will also reduce. Besides enlightening the management, RNs, physicians and other healthcare workers of Duke Hospital & Health Center about the potential benefit of the proposed change, they will also be encouraged to express any of their concerns or worries in relation to the proposed change, and these would be addressed in a satisfactory, unequivocal and explicit manner.
Essentially, there would be less likelihood of resistance to the proposed solution when all their concerns regarding the proposed solution are clearly and sufficiently addressed. They are also likely to approve and support it when they are amply involved and consulted, and when they are well informed about the justification for the change (Holcomb, 2006). Consulting and involving all the key stakeholders during the project would actually ensure that they all have the feeling of involvement and ownership of the project. This is crucial since it will increase the likelihood of them being receptive to the proposed the change.
2.0 Description of current problem
The current problem entails how children patients with Addison’s disease are treated. In Addison’s disease, WebMD (2014) stated that the adrenal glands do not produce adequate of cortisone hormone, or less often, aldosterone hormone; hence, it is at times called hypocortisolism or chronic adrenal insufficiency. At my health care organization, which is Duke’s Children Hospital & Health Center, Addison’s disease is one of the very complicated illnesses that Registered Nurses try to treat. An effective solution needs to be developed that would assist with suppressing the complications of this disease to children patients at the health care organization. An Addisonian crisis is one of the most complicated conditions of Addison’s disease and it usually arises whenever the supply of hormones becomes dangerously low, and it crops up when the body of the victim in under intense stress (WebMD, 2014). Nearly all of the strenuous scenarios are experienced after a patient undergoes a surgical operation. Stress impacts adrenal glands to produce more adrenaline to help patient in coping up, but Addison’s disease patients cannot effectively cope up with the added stress. The impacts of the problem are diverse and a patient with this disease can die of heart attack if they are not able to control the stress (Ross et al., 2014).
As RNs, we often suffer emotionally whenever children affected by Addison’s disease die under our care when they are not able to cope up with depression. The stubbornness of this disease questions the quality of care that Registered Nurses deliver to the children patients at Duke Hospital & Health Center. Some relatives of the patients openly condemn us whenever a patient experiences occurrences of insanity or even death. It is worth noting that the impact of the disorder on patient outcomes is diverse given that some patients may either become insane or die, since some of the children are not able to contain depression. In addition, the condition can further complicate the body to cause hormonal imbalance that necessitates homeostatic regulation to bring them to equilibrium (Holcomb, 2006).
3.0 Detailed description of proposed solution
The proposed solution encompasses several methods. One of them is to review the nursing process being used presently in diagnosing and treating patients with Addison’s disease. This will be geared to produce results that could be evaluated to bring outcomes that ensure the entire condition gets eliminated. The proposed solution also requires formation of EBP models that basically try to figure out the underlying reason for the continuous stubbornness of this disorder. Moreover, the proposed solution engages the elements of a comprehensive training of RNs at Duke Hospital & Health Centre to have an extensive and intensive approach to the problem. Nonetheless, this proposed solution does not omit the traditional models of dealing with the problem of substituting the hormones that adrenal glands are producing. Even though Cortisol is replaced orally with hydrocortisone tablets, we as RNs ought to find ways in which it would be administered through injection in order to enhance faster absorption of the drug into the blood system.
The rationale for selecting the proposed solution is that it will allow the RNs at Duke Hospital & Health Center to provide the children patients suffering from Addison’s disease with the best possible and optimal treatment that will reduce the stubbornness of this disorder and help the patients control stress. More importantly, the proposed solution will facilitate better management of the disease and thereby help in reducing the incidences of insanity and death as a result of Addison’s disease.
4.0 Evidence from literature
Ross et al. (2014) noted that Addison’s disease in known to crop up whenever the adrenal gland is not able to produce its contents in an effective manner. It is of note that the proposed solution entails formation of Evidence-Based Practice models aimed at gaining an understanding of the underlying reason for the continuous stubbornness of Addison’s disease. EBP is understood as the judicious, explicit, conscientious usage of existing best evidence in making decisions regarding the care of individual patients (White, 2009). In essence, the practice of evidence-based medicine implies incorporating individual clinical expertise with the finest available external clinical evidence from systematic research. White (2009) stated that EBP is a very helpful approach to enhancing the impact of practice in the management of Addison’s disease, adding that nurses in the care of Addison’s disease patients should always direct significant attention to evidence. They should honor the many dissimilar types of evidence. Those who advocate the use of EBP in the management of Addison’s disease emphasize on the findings of major experimental comparisons in documenting the effectiveness of treatment against untreated control groups, against other treatment, or both. They do this given that properly conceptualized and completed experiments – randomly controlled trials – are great way of showing that a treatment resulted in a specific alter (Brandão Neto & Carvalho, 2014).
The proposed solution also engages the elements of an all-inclusive training of Registered Nurses in the health care organization to have both an extensive and intensive approach to the problem. According to White (2009), nurses should be provided with a comprehensive training that will allow them to deliver both family-centered and patient-focused treatment of Addison’s disease. This comprehensive training will ensure that RNs never lose their sight of the fact that Children with Addison’s disease, are primarily individuals, and not just patients. As such, the patient’s family has to be included at each stage of the treatment process (WebMD, 2014).
5.0 Implementation logistics
The hospital’s administration would integrate the change into the existing structure, workflow and culture of the organization using several ways. The first one entails putting in place principles and standards that would incorporate the change into the existing organizational culture, workflow and structure. The other way is using enticements such as financial rewards that are aimed at encouraging RNs and other health care workers to be amenable and open to the change. Another equally important way is using punitive measures whereby the health care personnel would be compelled to accept the change, and those who try to resist the change are actually demoted or sacked. Two influential people, a Charge Nurse and a Nurse Manager would be responsible for initiating the change process, educating all registered nurses, in addition to supervising the process of implementation. The Charge Nurse would initiate the change process and develop a shared vision for Duke Hospital & Health Center, whereas the Nurse Manager will supervise the process of implementation to make sure that it is conducted effectively.
6.0 Resources required for implementation
Several resources are needed. (i) Human resources – Duke Hospital & Health Center’s workers such as RNs, nurse assistants and physicians would be included in implementing the change process. (ii) Tools for assessment would be required comprising questionnaires, surveys, pretests as well as post-tests. (iii) Educational materials – pamphlets, booklets, posters, and brochures would be required. Computers would also be utilized to create PowerPoint presentations. (iv) Funds – the budget for the project is $61,918 bearing in mind both the project’s scope and size
7.0 References
Brandão Neto, R., & Carvalho, J. (2014). Diagnosis and classification of Addison’s disease (autoimmune adrenalitis). Autoimmunity Reviews, 13(4/5), 408-411. doi:10.1016/j.autrev.2014.01.025
Holcomb, S. S. (2006). Hospital Nursing: Do the Clues Add Up to Addison’s Disease? Nursing, 36(3): 64
Ross, I., Dandara, C., Swart, M., Lacerda, M., Schatz, D., & Blom, D. (2014). 9β Polymorphism of the Glucocorticoid Receptor Gene Appears to Have Limited Impact in Patients with Addison’s Disease. Plos ONE, 9(1), 1-6. doi:10.1371/journal.pone.0086350
The writer has to be very concise when he compose this papers as the complain with most of my papers has been that the are not concise, and also the writer has to focus on the main points and elaborate on them clearly using concrete examples to support the facts. In this paper, they are four main points to discuss , the writer must clearly discuss them and use examples to support the facts.
Personal Branding
The concept of branding is often applied to large corporations such as Pepsi-Cola, Nike, Starbucks, or Toyota. Brands communicate powerful associations to the external stakeholders and hence organizations spend millions of dollars enhancing the equity of their brands.
Some individuals take the idea of branding a step further, extending it to people as well. Consider Tiger Woods, Martha Stewart, or Emeril as prime examples of this personal branding philosophy. Tom Peters, a famous management guru, wrote a seminal article called “The Brand Called You” (Peters, 1997) urging individual professionals to think of themselves as brands and to stand out in the competitive marketplace by differentiating themselves.
The key to long-run success, Peters suggested, is to brand oneself effectively. Companies like Estee Lauder offer an in-house personal branding course. On the other hand, others believe that most individuals are not equipped to become brands because they lack the necessary qualities.
After reviewing the resources below, respond in 2 pages word documents minimum to the following:
• Why is branding important to an organization?
• Should the personal brand concept become a part of the DNA of 21st century professionals? If so, what steps must a person work through to develop an effective personal brand? If not, what are your reasons for thinking so?
• Compare how the process of branding an individual would be similar to branding a product. How would it differ?
• Defend your answer with specific examples
Resources:
Course Text
• Marketing Management
o Chapter 9, “Creating Brand Equity”
This chapter introduces the topic of strategic brand management and how it is used to build, measure, and manage brands to maximize their value.
Chapter 10, “Crafting the Brand Positioning”
This chapter summarizes how companies can effectively position a brand to best reach the target market by using brand differentiation and constant revisions to stay current.
• Articles
• Burnett, J., & Hutton, R. (2007). New consumers need new brands. Journal of Product & Brand Management, 16(5), 342–347. Retrieved from ProQuest Central database.
In this article, the authors propose that there are a considerable number of research studies on branding for products, but that very little exists for the process of branding services. They present a conceptual overview of how this type of branding can be developed.
• Cayla, J., & Arnould, E. (2008). A cultural approach to branding in the global marketplace. Journal of International Marketing, 16(4), 86–112. Retrieved from Business Source Premier database.
This paper outlines some of the challenges that future market managers will face in balancing a global, ethnocentric branding approach with the cultural, historical, polycentric, and symbolic significance of a brand.
One of the new focuses of branding that businesses need to understand is that of personal branding, and the author of this paper introduces this concept.
SAMPLE ANSWER
Personal Branding
Personal branding is a recent invention whereas the trend of people labeling themselves based on status and character is as old as individual relations. One’s personal brand is that dominant, vivid, positive thought that comes to the brain whenever one is thought of, such as the principles, abilities, and dealings that others relate one with. It is designed for the reason of influencing how others perceive one, and turning that view into prospect. For effective personal branding, one’s personal brand should induce the perception that one is different, superior and authentic relative to others already in the market (Burnett & Hutton, 2007). This implies that personal branding is a promise to the customers on what they should expect, for example, it’s an assurance that makes the buyer trust, “By buying this, I will be getting that.” This paper will, with the use of examples, explain the importance of branding, justify why personal branding should become an essential item of the DNA of the 21st century and finally compare and contrast personal branding and product branding.
Personal branding is of much benefit in marketing management. It works for all regardless of circumstances and conditions since all businesses are based on associations. Some of the benefits are that it creates more right kind of clients, it increases earning ability, ensures consistent business flow. It also draws many beneficial people that can benefit an individual, for example, Secretary of State Colin Powell’s straightforward and decent, and leadership won many in 1996. It enables one to get “Top-of-mind” class (Redsang, Peter, & Sanfranc, 2012). Personal branding increases credibility, creates opportunity for one to exercise leadership role, such as Federal Reserve Chairman Alan Greenspan could sustain up Wall Street with very few well-chosen terms. It gets one to achieve desired goals by enhancing prestige since it adds financial value to an individual (Burnett & Hutton, 2007). Additionally, it brings greater recognition of one while within his associates with a trend. These suggest that personal branding is important.
However, there are steps that must be considered during personal branding. These include transforming individual reflection into a personal brand that creates business prospect by taking an active control of the process and cutting and polishing ones brand so that everyone who gets in touch with it forms a similar fundamental set of expressions in their mind when they hear your name (Keller, 1993). Building a brand requires understanding, endurance and perseverance, failure of which results into loses. For example, some Internet firms misused millions on Super Bowl as they thought branding take place overnight (Margaret, 2002). Generally, brands take time to expand, for example, Oprah Winfrey spent time performing, carrying out talk shows and laboring to aid women before becoming universally-famous (Peters & Jeremie, 2027). Secondly, brands undergo organic growth as the best brands increase at the grassroots level since it is enhanced by strong communication, a sense of commitment. And finally, brands are not rational and demand consistency and clarity. For example, in 2001, K-Mart filed for insolvency in a budget that left buyers and sellers in upset state (Keller, 1993). Another aspect of personal branding is the fact that it is already element of individual interaction and is everywhere. Personal branding is in use by celebrities such as Stephen Covey, Meg Ryan, Charles Schwab and Joe Montana, as they try to turn their names into industries.
At the moment, judgments can be made about people with only little information at hand. For example by meeting casually meeting someone, you may get to know certain information about his education, his manners and characters. This is because his individual image has been encountered, as revealed by the DNA of his individual manner (Margaret, 2002). Therefore, personal branding is an organic and natural part of human culture, though the difference today is that we have learnt how to detect how others perceive us (Cayla & Arnould, 2008). This therefore necessitates personal brand concept to become a core element of the DNA of 21st century professionals.
In conclusion, following the importance and illustrations hinted on above, personal branding concept should become part of the DNA of the 21st century professionals. Product branding is in most aspects similar to personal branding, however, while the latter is a natural aspect of human beings, the former is not natural as it has to be done physically.
References
Keller, K. L. (1993). Conceptualizing, measuring and managing customer-based brand equity. Journal of Marketing 57(1), 1-22.
Margaret, C. C. (2002). Building brand equity. International journal of Medical Marketing Journal, 2(3), 1-16.
Burnett, J. & Hutton, R. (2007). New consumers need new brands. Journal of Product and Brand Management, 16(5), 342-347.
Cayla, J. & Arnould, E. (2008). A cultural approach to branding in the global marketplace. Journal of International Marketing, 16(4), 86-112.
Peters, T. & Jeremie, K. (2027). The brand called you. Fast company. International Journal of Medical Marketing, 3(1), 234-239.
Redsang, T, Peter, J. & Sanfranc, K. (2012). Impact of personal brand in the world market. Journal of International Marketing, 45(4), 23-87.
We can write this or a similar paper for you! Simply fill the order form!
Analyze Overstock.coms strategic choices at the corporate level, to include how these strategies follow Porter’s generic strategies. Are they in sync?
Which of the four quadrants of the ‘Grand Strategy Selection Matrix does Overstock.com fit in, and why?
SAMPLE ANSWER
Introduction
O.co is the popular initials of Overstock com Inc, the American Company that operates online businesses that are based in and also outside the US. Its head office is located in Cottonwood heights, Utah near the Salt Lake City.
Michael Porter’s (1996) generic strategies eventually narrow to the two major headings between the cost advantage and the product differentiation strategies. Overstock Company applies the cost advantage in its corporate strategy level to market its products on its online business segment whose cost leadership advantage has earned its differentiated status as a cost efficient and effective products distributor as it strives to be the most economical or the lowest cost provider in the entire business to most customer segments. It was initially known as the D2- Discounts Direct before it rebranded itself to Overstock.Com. It sells all types of domestic equipments, appliances, furniture, jewelry, computers, magazines, DVDs, apparels among other requirements. It offers various discounts on brand names and also non branded products. Overstock operates a large online retailer that primarily supplies the American market with literally anything they would like to purchase including vehicles. It also operates a World stock Fair Trade shows that offers its clients a variety of handcrafted products. The characteristics of Overstock are in sync with porter’s arguments.
Overstock Company has the characteristics displayed in Quadrant 1 below where strong and very competitive companies flourish in markets that are rapidly growing. Overstock strategic position in online sales places it in a strategic market where its products have a wide global market and its development strategy has an excellent opportunity. The company can expand and develop its market in all directions, horizontally, forward or even backwards. Being a company that sells multiple products, its marketing strategy is to offer products that attract more clients because of their discounts and low pricing policies which aid it to penetrate the market. (Porter, 1996)
Weak Competitive
Strong Competitive
1.
Companies in Rapid
Companies In
2. markets
growth Market
with Rapid Growth
1
Market Dev
Market Dev
2
Market Penetration
Market Penetration
3
Product Dev
Product Dev
4
Horizontal Integration
Horizontal Integration
5
Divestiture Liquidation
Related diversification
6
Forward integration
Weak Competitive
Strong Competitive
3.
Companies In markets
4. Companies In Mkt
that have slow Growth
with Slow Growth
1
Retrenchment
Joint venture
2
Related Diversification
Related Diversification
3
Unrelated diversification
Unrelated diversification
4
Liquidation
5
Divestiture Liquidation
Overstock sells its products mostly at the industry’s average prices or at times lower to increase its market share and it subsidizes its costs by applying the economies of scale, outsourcing, process efficiencies and its experience on the curve effect. Its major aim is to achieve a low- cost distribution network that’s relatively economical than its rivals and it’s the main focus of the firm’s strategy. (Hayes, Pisano, Upton and Wheelwright, 2005)
Porter (1996) argues that by utilizing the value chain and the value system and also the linkages a company can improve its efficiency significantly while exploiting the sources of competitive efficiency and other value added strategies.
Reference
Hayes, Pisano, Upton and Wheelwright (2005) Pursuing the Competitive Edge; New York, Wiley and Sons, page 264.
Porter, M.E. (1996) What is Strategy? Harvard Business Review, Boston pp 61-78 Vol.74, No.6 November-December.
We can write this or a similar paper for you! Simply fill the order form!
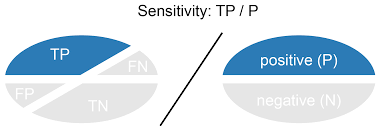
In order for screening to take place, it must be feasible. In other words, it must be economical, highly reliable and valid, free of risk, available to a large number of individuals, and ethical to screen.
For this Application Assignment please download the Sensitivity/Specificity Problem Set and submit your responses.
Sensitivity/Specificity Problem Set
For Week 11’s Application Assignment complete this Sensitivity and Specificity problem set. Make sure to check the Calculation Application Rubric prior to submitting your responses.
Clearly mark your responses for each question.
When you are completed, submit to the Week 11: Application Dropbox using the correct naming convention on the file. See Week 11’s Application page for directions.
1) Sensitivity is:
A. The probability that a test correctly classifies as positive those who have preclinical disease.
B. The probability that a test correctly classifies individuals without preclinical disease as negative
C. The probability that those who test positive have the preclinical disease
D. The probability that those who test negative do not have the preclinical disease
2) Specificity is:
A. The probability that a test correctly classifies as positive those who have preclinical disease.
B. The probability that a test correctly classifies individuals without preclinical disease as negative
C. The probability that those who test positive have the preclinical disease
D. The probability that those who test negative do not have the preclinical disease
A screening examination was performed on 250 persons for Factor X, which is found in disease Y. A definitive diagnosis for disease Y among the 250 persons had been obtained previously. The results are charted below:
RESULTS OF DIAGNOSIS
TEST RESULTS Disease Y Present Disease Y Absent
Positive for Factor X 40 60
Negative for Factor X 10 140
3) The sensitivity of this test is expressed as:
A. 40%
B. 70%
C. 29%
D. 80%
4) The specificity of this test is expressed as:
A. 40%
B. 70%
C. 7%
D. 80%
5) The positive predictive value of this test is:
A. 40%
B. 70%
C. 7%
D. 80%
6) The negative predictive value of this test is:
A. 40%
B. 70%
C. 93%
D. 80%
7) If the same screening test is conducted in two populations, one with a high prevalence of the disease and one with a low prevalence of the disease, assuming the sensitivity and specificity of the screening test are the same, which of the following statements about positive predictive value (PPV) applies:
A. PPV is higher in the screened population with higher prevalence
B. PPV is lower in the screened population with higher prevalence
C. PPV is the same in both populations
D. It cannot be determined
8) Lead time bias can be described as:
A. An apparently lower survival rate among persons screened compared to an unscreened group.
B. A bias that occurs because screening tends to identify cases with less aggressive forms of the disease
C. A similar survival time for persons identified during a screening program relative to persons who are diagnosed by clinical symptoms.
D. An apparently longer survival time among those identified during a screening program because they were identified at an earlier stage of their disease
9) Length-Bias can be described as:
A. An apparently lower survival rate among persons screened compared to an unscreened group.
B. A bias that occurs because screening tends to identify cases with less aggressive forms of the disease
C. A similar survival time for persons identified during a screening program relative to persons who are diagnosed by clinical symptoms.
D. An apparently longer survival time among those identified during a screening program because they were identified at an earlier stage of their disease
A new screening test for a disease is developed for use in the general population. The sensitivity and specificity of the new test are 60% and 70%, respectively. Four hundred (400) people are screened at a clinic during the first year the new test is implemented. (Assume the true prevalence of the disease among clinic attendees is 10%.)
Calculate the following values:
10) The predictive value of a positive test is:
A. 13.3%
B. 18.2%
C. 24%
D. 22.2%
11) The number of false positives is:
A. 108
B. 132
C. 24
D. 252
SAMPLE ANSWER
Sensitivity and Specificity
Sensitivity/Specificity Problem Set
For Week 11’s Application Assignment complete this Sensitivity and Specificity problem set. Make sure to check the Calculation Application Rubric prior to submitting your responses.
Clearly mark your responses for each question.
When you are completed, submit to the Week 11: Application Dropbox using the correct naming convention on the file. See Week 11’s Application page for directions.
Sensitivity is:
The probability that a test correctly classifies as positive those who have preclinical disease.
The probability that a test correctly classifies individuals without preclinical disease as negative
The probability that those who test positive have the preclinical disease
The probability that those who test negative do not have the preclinical disease
Specificity is:
The probability that a test correctly classifies as positive those who have preclinical disease.
The probability that a test correctly classifies individuals without preclinical disease as negative
The probability that those who test positive have the preclinical disease
The probability that those who test negative do not have the preclinical disease
A screening examination was performed on 250 persons for Factor X, which is found in disease Y. A definitive diagnosis for disease Y among the 250 persons had been obtained previously. The results are charted below:
RESULTS OF DIAGNOSIS
TEST RESULTS
Disease Y Present
Disease Y Absent
Positive for Factor X
40
60
Negative for Factor X
10
140
The sensitivity of this test is expressed as:
40%
70%
29%
80%
The specificity of this test is expressed as:
40%
70%
7%
80%
The positive predictive value of this test is:
40%
70%
7%
80%
The negative predictive value of this test is:
40%
70%
93%
80%
If the same screening test is conducted in two populations, one with a high prevalence of the disease and one with a low prevalence of the disease, assuming the sensitivity and specificity of the screening test are the same, which of the following statements about positive predictive value (PPV) applies:
PPV is higher in the screened population with higher prevalence
PPV is lower in the screened population with higher prevalence
PPV is the same in both populations
It cannot be determined
Lead time bias can be described as:
An apparently lower survival rate among persons screened compared to an unscreened group.
A bias that occurs because screening tends to identify cases with less aggressive forms of the disease
A similar survival time for persons identified during a screening program relative to persons who are diagnosed by clinical symptoms.
An apparently longer survival time among those identified during a screening program because they were identified at an earlier stage of their disease
Length-Bias can be described as:
An apparently lower survival rate among persons screened compared to an unscreened group.
A bias that occurs because screening tends to identify cases with less aggressive forms of the disease
A similar survival time for persons identified during a screening program relative to persons who are diagnosed by clinical symptoms.
An apparently longer survival time among those identified during a screening program because they were identified at an earlier stage of their disease
A new screening test for a disease is developed for use in the general population. The sensitivity and specificity of the new test are 60% and 70%, respectively. Four hundred (400) people are screened at a clinic during the first year the new test is implemented. (Assume the true prevalence of the disease among clinic attendees is 10%.)
Calculate the following values:
The predictive value of a positive test is:
3%
2%
24%
2%
The number of false positives is:
108
132
24
252
We can write this or a similar paper for you! Simply fill the order form!
Knowledge Management, Social Networks and Innovation
Knowledge Management, Social Networks and Innovation
Intention and Aims
The individual assignment requires an analysis of the exploitation of innovation within an organisation through a commercially developed SOCIAL NETWORK service. This involves producing an INDIVIDUAL formal report (max 2500 words excluding references). The assignment requires an analysis of a recent IBM initiative relating to ‘Social Business’ ibm.com/socialbusiness/uk
You are required to specifically identify how ANY organisation may ‘learn’ the nature of a SOCIAL MEDIA system which may be adopted to exploit the extent of the organisations ‘knowledge’ leading to enhanced ‘innovation’. For clarity your report should therefore form FOUR elements, ie organisational learning approach, social media development, knowledge management features and the extent of subsequent innovation.
It is expected that an in-depth investigation and analysis is undertaken to determine the extent of the theoretical and practical issues involved in how the
Social Media service was achieved through knowledge and innovation frameworks. Examples should be drawn from other research into well formulated networks currently available, ie; Facebook, Youtube, Twitter, Google, Linkedin, NING, Writeboard, Storybird, etc. Youshould include how your case analysis enabled successful knowledge and innovation within the organization. This should also involve a consideration of developments in the field by providing insightful explanations of current and future potential social media exploitation.
The report should provide an academic analysis by recalling the theories and approaches that are relevant to the topic. You may structure your report to include any relevant tables or diagrams with a suggested format as: features of organisational learning, nature of knowledge and how it may be managed, a contextual description of social networks and issues relating to the exploitation of organisational innovation through the Social Media systems.
The following learning outcomes are assessed through this assignment.
1 To critically discuss the nature and process of knowledge creation and transfer within organisations.
2 To critically evaluate how organisational and social dynamics combine to engender innovation.
3 To analyze the application of concepts and theories related to new ‘social network’ technologies
4 To be able to present theoretical and empirical evidence to address complex problems and practical situations in relation to knowledge management and innovation development
The individual report should reflect:
• Ability to identify diverse and high quality sources of information (a minimum of 40 references are required from different sources). These should include: academic journals/ books/ trade publications, government and industry data, websites, etc.
• Demonstration of clear understanding and synthesise of the available information in order to gain an in-depth knowledge and understanding of the topic(s).
• Ability to discuss complex information clearly and concisely, and to construct coherent and logical arguments. • Ability to present your findings in a
professional and well structured report format, including effective use of figures, tables, appendices
and referencing (Harvard Style is required).
It is essential that your research should include novel, thoughtful analysis and the impact of social networks on innovation through referencing and
incorporation of ideas from multiple sources.
In addition, the opportunity will be taken to enhance ‘employability’ criteria through attention to ‘presentation skills, ‘clarity of analysis’, ‘team
support’, ‘entrepreneurship’, etc
We can write this or a similar paper for you! Simply fill the order form!
The Impact of emotional confidence on purchase behavior
The Impact of emotional confidence on purchase behavior among students in UK
Literature Review:
Summarize the literature in the table format:
Title/ Journal Academics
Research Questions
Key findings
Methodology rationale (qualitative)
Area Literature(Services Marketing)
Areas of Future Research
1)Keep tight
2)Consumer behavior Model
3)Has to be related services Marketing
4)identify key word
5)Context contribution to the knowledge
6)Harvard Style
7)Critical technique
8)That you are aware of what is going on in the field
and thus your credentials
9)that there is a theory base for the work you are proposing to do
10)that your work has significance
11)Literature review starts broad and narrows to show how past research relates to your project
12)each table must be accompanied by an analysis that summarizes interprets and synthesizes the literature that you have charted in the table
13)Avoid global Statements
14)Justify Comments such as no studies were found.
15)if the results of previous studies are inconsistent or widely varying cite them separately
16)Cite all relevant references in the review section of thesis or journal article.
17)Issue is Consumer Purchasing
18)Don’t use compulsive buying
19)UK students aged 18-24
20)to attach an appendix a list of the key authors in the field and the area in which they have conducted research.
21)One Overall 3 key objectives
22)Keep very tight
23)Services Marketing ground
We can write this or a similar paper for you! Simply fill the order form!
Different development models(It just a theme, you can decide the topic)
1. Countries have used different types of development models in East Asia. Identify what these different models are and account for the reasons for this
difference. Although you will need to refer to some descriptive material to illustrate the process of development you are asked to analyse how development models have changed and to use conceptual frameworks to explain this change. (approximately 75% of the report)
2. Explain why it is important for business firms to understand the nature of these different development models. (approximately 25% of the report)
3. An essay is inappropriate for this task and a report format must be adopted. It is also essential that critical assertions and key comments are referenced
and that the referencing system follows the Harvard format. Marks will be deducted in accordance with the School’s conventions for reports which are over the word limit, poorly written or poorly referenced. The word limit applies to the main body of the report only and excludes the contents page, executive
summary, list of references consulted, and appendices. It includes tables, figures, and references in the text. You should only include appendices if you
refer to them in the text and they are essential material for the reader.
4. Must be an original works.
5. Please do not stray from the point. I have ever get the worst of it.
We can write this or a similar paper for you! Simply fill the order form!