use book for reference health and health behaviour 130.please read every question instructions because they are different for every question and choose one model and answer all the questions by taking that model.do not use different model for other questions.i will attach files of questions along with instructions.regards
SAMPLE ANSWER
Health behavior refers to an individual’s personal beliefs as well as activities carried out concerning their health and wellbeing to attain, promote and maintain better health lifestyles. Such health activities involve; not smoking or drinking excess alcohol, doing regular exercises to enhance physical fitness and eating well among others. Risky health behaviors will, therefore, refer to activities that negatively influence an individual’s health lifestyles. I have chosen drinking of alcohol in pregnancy as risk behavior those impacts on the health of the Australian citizens.
Women who happen to take alcohol during their pregnancy incur negative health effects probably to their babies as well as to themselves. Excessive drinking of alcohol at pregnancy period causes miscarriages and premature birth. Alcohol is a toxic substance that will rapidly enter the baby via the placenta into the bloodstream(McCarthy et al,2013).Too much of alcohol can even increase the risks of a new baby to be stillborn.
Heavy drinking of alcohol may tremendously damage the baby’s nervous system. The baby will start developing fetal alcohol spectrum disorders (FASD) having various problems like slow learning or social defects and birth defects. FASD will, therefore, refer to a term that describes the range of impacts that occurs to an individual exposed to alcohol in the uterus. Such impacts will involve mental, physical, behavioral and learning defects for a lifetime(McCarthy et al,2013). Babies born with fetal alcohol syndrome will tend to have facial defects, being small, learning difficulties, poor muscle development, and behavioral problems. It also causes delivery of babies with low birth weights which greatly affects the baby’s chances of survival and to have better health. From national strategy household survey, 1 in 16 lives born babies had less than weighed less than 2500 grams at birth .generally children born to alcoholic mothers tends to have damaged brains, birth defects, poor and slow growth, low intelligence quotient, language, and speech deficit as well as social and behavioral problems(McCarthy et al,2013).
From the various behavioral models, I chose the health belief model (HBM) as a behavioral change model of which I apply as not drinking alcohol during pregnancy. The health belief model will, therefore, refer to a theory that aims in predicting whether an individual can choose to involve in a health activity in order to lower or prevent chances of getting a disease or premature death (Chimied et al 2013). The model comprises of two types of beliefs that influence individuals to take necessary preventive actions; beliefs related to readiness to take actions as well as beliefs related to modifying agents that enable or inhibit an action. .the variables that are used in measuring the readiness to undertake any action is perceived susceptibility to the illness for example FASD disorders affecting babies as a result of alcohol consumption .another component of the model is the benefits, for instance, the perceived impotence of avoiding alcohol during pregnancy to the newly born babies. The barriers e.g the perceived costs and also constraints when women are taking the action of abstinence of alcohol during their pregnancy period. The theory advocates that the individual variables contribute in predicting their health behaviors. The model can be applied to potentially unhealthy behavior specifically drinking alcohol at pregnancy period. This can be achieved by examining the attitudes and beliefs that are related to taking of alcohol at pregnancy using variables; it can be predicted that fetal alcohol spectrum disorders could be avoided(susceptibility) hence discouraging the consumption of alcohol at pregnancy periods.
There are two Australian strategies of changing the risk behavior of taking alcohol during pregnancy. The health promotion champagne and the enactment of policies that covers the use of alcohol in Australia. The first strategy that is the development and implementation of policies that governs the use of alcohol .the government of Australia has laid down policies and guidelines to control the consumption of alcohol effectively. The national health and research council has developed guidelines policies that effectively targets to control women who consume alcohol during pregnancy period to reduce the health risk associated with. The strategy is specifically laid down to control the maternal alcohol consumption rates critically during the pregnancy and breastfeeding (Keith et al, 2014).
The policy recommends that any woman who are pregnant or are planning to become pregnant should significantly refrain from alcoholic drinks through their pregnancy period. Women who have taken any alcohol should be reassured while being given the advice to abstain from any further alcoholic drinks. The policies targeting alcoholic use in pregnancy has been established because of the concerns that are around alcohol usage when breastfeeding and during pregnancy period. The policy came into action in the year 2009.The actions of the strategy involve setting up of strict measures that will compel the women that initially used alcohol to change their behavior and to adopt healthy behaviors through the implementation of such alcoholic laws and also the reinforcement of women who are abstaining(Keith et al,2014). The strategy is complying with the Ottawa chatter of health promotion by advocating to move into the arena of public health policy and to advocate for clear political commitment to health .according to my rationale, the strategy is of great significance and leads to the attainment of the healthy lifestyle.
The second strategy is the role of Australian media as a strategy in championing the campaign for educating and informing the community. The strategy aims at increasing the awareness of alcohol use and promotion of healthy attitude and enhancement of healthy uses of alcohol.The national alcohol campaign was officially launched in the year 2000 and mainly targets the pregnant women or young teenagers who usually encounters early pregnancies(Hildebrand et al,2013). The media strategically creates awareness to the public on the unhealthy effects of consumption of alcohol.It tries to advocate the public to change their attitudes towards consumption of alcohol at pregnancy period through media.
.the strategy utilizes social media such as the use of brochures, magazines, newspapers and internet sites .the national campaign strategy critically tries to change the attitudes, belief and behaviors of the target group. It also facilitates the target group to change into health behavior such as health drinking of alcohol. The strategy tries to change the attitudes of drinking alcohol during pregnancy period hence aiding in resolving the related health problems(Hildebrand et al ,2013). The strategy is complying with the Ottawa chatter for health promotion through mass education on a significance of health behaviors. My rationale towards the strategy is that media will play an effective role in mobilizing the Australian citizens to change into healthy behaviors especially to women at pregnancy period.
References
Hildebrand, J., Maycock, B., Howat, P., Burns, S., Allsop, S., Dhaliwal, S., & Lobo, R. (2013). Investigation of alcohol-related social norms among youth aged 14–17 years in Perth, Western Australia: protocol for a respondent-driven sampling study. BMJ open, 3(10), e003870.
Keith, M. R., & Moore, M. (2014). Public Health Association of Australia (NT Branch) submission to Northern Territory Select Committee on Action to Prevent Foetal Alcohol Spectrum Disorder.
McCarthy, F. P., O’Keeffe, L. M., Khashan, A. S., North, R. A., Poston, L., McCowan, L. M., … & Kenny, L. C. (2013). Association between maternal alcohol consumption in early pregnancy and pregnancy outcomes. Obstetrics & Gynecology, 122(4), 830-837.
Schmied, V., Johnson, M., Naidoo, N., Austin, M. P., Matthey, S., Kemp, L., … & Yeo, A. (2013). Maternal mental health in Australia and New Zealand: A review of longitudinal studies. Women and Birth, 26(3), 167-178.
We can write this or a similar paper for you! Simply fill the order form!
Womens Health and Health Policy Assessment
Policy Topic Search and Selection
Research the Internet for keywords such as “Health” and “Health Policy” and select a policy topic that is of interest to you.
Womens Health and Health Policy
You will use this policy topic
throughout the course for your individual assignments. Review different topics and ideas at The Kaiser Family Foundation, https://kff.org, Health Policy
WEB LINK: https://kff.org
Consider reviewing the tutorials and issues modules when researching your particular topic.
After completing your research and selecting your topic, submit a 300 word APA formatted summary on your selected policy topic and the stakeholders that are
affected by the topic. For example, your stakeholders may be Veterans, the elderly, HIV patients, or the uninsured. A minimum of two references is required.
In effective review analyses and synthesizes material, and it should meet the following requirements: (Caulley, 1992)
Compare and contrast different authors’ views on an issue
Group authors who draw similar conclusions,
Criticise aspects of methodology,
Note areas in which authors are in disagreement,
Highlight exemplary studies,
Identify patterns or trends in the literature
Highlight gaps in and omissions in previous research or questions left unanswered
Show how your study relates to previous studies,
Show how your study relates to the literature in general,
Conclude by summarising what the literature says.
A literature review has a number of purposes. It enables you to :
Define and limit the problem you are working on,
Place your study in a historical perspective,
Avoid unnecessary duplication,
Evaluate promising research methods,
Relate your findings to previous knowledge and suggest further research.
Give your Supervisor a sense of your research interests.
so please write about the below following headings please this is PHD level so I need high quality papers.
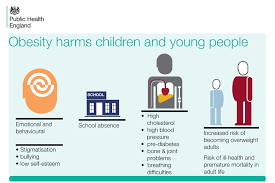
Potential implications of childhood obesity
a. Health implications
You know the medical disease links to obesity please write about it.
b. Social implications
Relation with friends and family you the impact of this
c. Economic implications
You know how much obesity cost
3. Government-focused approach
We need to talks about the role of government in different country and how much government play important role to combat obesity
4. Family-focused approach
The important of parent?s role in order to stop obesity
5. School-focused approach
You the school how much play important role through the school canteen or the curriculum or teach as model for student
6. School nurse-focused approach
Please this is very important so talks about the role of school nurses and the can use health education.
8. Summary
We can write this or a similar paper for you! Simply fill the order form!
See uploaded document in my account. Hampton Roads is a region of Southeast Virginia in the USA. Answer the questions 1 through 11 and write a one (1) page
essay analyzing the impact of the community on the health and welfare of an elderly client in Hampton Roads.
1. Identify the boundaries of Hampton Roads.
2. List 4 – 7 major health services inside the Hampton Roads community.
3. List the 10 most common causes of death in Hampton Roads.
4. List the 10 most common ethnic groups in Hampton Roads.
5. What is the age distribution? The gender distribution? The average educational level?
6. List environmental threats to elders in Hampton Roads.
7. List opportunities for healthy activities for elders in Hampton Roads.
8. Describe the average climate of each season in Hampton Roads.
9. List the possible effects of climate on health status of an elderly client.
10. List where you find information about emergency services/evacuation plans in Hampton Roads.
11. List the flora and fauna found in Hampton Roads.
Essay: Analyze the impact of the community on the health and welfare of an elderly client in Hampton Roads.
A-What are the risks and benefits of living in Hampton Roads as an elderly individual?
B-Discuss services that would enhance the quality of life for the elderly living in Hampton Roads.
C-Do you recommend Hampton Roads as a place for elderly to live?
We can write this or a similar paper for you! Simply fill the order form!
According to Conal Furay and Michael Salevouris in ‘The Methods and Skills of History’, What does it mean to “think like a historian?” Identify three key aspects of “thinking like a historian” and explain why you believe that they are compelling or problematic.
Use at least three (3) quality references Note: Wikipedia and other related websites do not qualify as academic resources.
Your assignment must follow these formatting requirements:
Be typed, double spaced, using Times New Roman font (size 12), with one-inch margins on all sides; citations and references must follow APA or school-specific format. Check with your professor for any additional instructions.
Include a cover page containing the title of the assignment, the student’s name, the professor’s name, the course title, and the date. The cover page and the reference page are not included in the required assignment page length.
We can write this or a similar paper for you! Simply fill the order form!
The Science of Nutrition, Third Edition, Thompson JL, Manore MM, Vaughan LA, 2012, Pearson/Benjamin Cummings (2nd edition is acceptable.)
Part 1(this part is already done by me):
Keep a food record for 4 Days and enter data into the diet analysis program of your choice.Keep written 4-day food record with at least one weekend day. A 4
-day record of food intake will give you an average that is a more accurate reflection of nutrient status than a single day. Keep an accurate food record and include
the foods, the portion sizes, the time of daily meals and snacks are eaten and any other patterns you notice about your eating routine. It would be best
to make your entries at least once a day if not 2 or 3 times a day. Do Not try to improvise!
After you have established a profile you are ready to enter your 4-day food record. Select “Day 1” and enter the data, then “Day 2”, and enter then “Day 3”
etc. and enter. (The Super Tracker asks for dates.) Make sure you enter foods into specific days or dates. Also, be sure to organize them according to breakfast,
lunch etc. Enter your “helping size” by using the portion sizes available to you as you enter the foods (in Tbls, cups, ounces etc.) Enter the
real amount of food that you ate. Be precise to get the most accurate assessment. (Hint: Most students underestimate the amount of food they eat. Be
accurate.) Refresh your memory about portion sizes by reading Chapter 2 from your text book The Science of Food or visit mypyramid.gov for portion size
information.
Part 2:
Use the “Reports” to analyze your dietary intake.
For this assignment you will use a combination of food AND nutrient analysis reports: From MyDietAnalysis you will need the “Actual Intake VS Recommended
Intake”(file:///C:/Users/Adina/Downloads/Actual_Intakes_-vs-_Recommended_Intakes_Report.html), “The Plate”(the USDA plate guideline), “Meal Assessment
Report”(file:///C:/Users/Adina/Downloads/Meal_Assessment_Report.html), “Calorie
Distribution”(file:///C:/Users/Adina/Downloads/Calorie_Assessment_Report.html) and “All Nutrients
Spreadsheet”(file:///C:/Users/Adina/Downloads/All_Nutrients_Spreadsheet_Report.html).
Write a comprehensive assessment of your nutrient intake in narrative form. This section should take up at least 1-2 pages. Do NOT outline information from
the reports but rather comment on the content of the reports. Address the following topics:
Actual VS Recommended for macronutrients: Compares your intake levels to the “Recommended Intake ” (DRIs). You need to report on : calories, protein,
carbohydrate, fat, saturated fat, fiber. You must include examples of the foods that contributed the most of these nutrients to your intake (check the
Nutrient Spreadsheet for these details.) If you choose weight loss address how much lower your caloric recommendation is for your profile.
Actual VS Recommended for micronutrients: Discuss any nutrient that was significantly greater or less than the recommendation according to the DRI’s (25 %
more or less). YOU NEED TO ADDRESS the following nutrients regardless: Vit. A, Vit. C, Vit. D, Vit. E, folate, iron, calcium, sodium and potassium. Refer to
the Nutrient Spreadsheet to determine what foods contribute to these levels. You MUST include examples of the foods that contribute to these nutrient levels.
If levels are low, what foods would increase them? If they are high, address what foods contributed to those levels? Explain any pattern you see.
AMDR (Calorie Distribution, % of calories from fat, carbohydrate and protein): Compare your macronutrient distribution with the AMDR for Carbohydrate,
Protein and Fat. Explain how well your intake falls into these categories. Be careful not to confuse the AMDR with the “Actual VS Recommended” percent
measures. They are different measures.
The Plate Diagram: How does your food intake compare to the USDA Plate guideline? Discuss the food groups in excess and short of the target number of
servings and again use examples from your own dietary intake.
Explain whether the “Plate” is predictable or not based on your nutrient status from the nutrient report. This is a little tricky but helps you understand
that the food pyramid is not always a reliable tool for assessing nutrient levels. Example 1: Your Vitamin C levels exceed the recommendations but your fruit
and vegetable intake were both considerably lower than the target. You notice in the All Nutrient’s Spreadsheet or the Food Details report that the green
peppers in your beef/pepper stir fry gave you all the vitamin C you need for one day. Example 2: If your fiber levels are low according to the nutrient
report you would expect your fruit and vegetable levels to be low in the Plate Report or Food Groups report. If your fruit level is high in this case it may
well be from the excessive amount of juice. You could find this out by using the All Nutrient’s Spreadsheet or the Food Details report.
Meal Assessment : Discuss any patterns you see in nutrient or food intake. What meal gives you the most calories/least calories? How about the most nutrient
density? Explain any other patterns that you noticed from your own notes about your food intake, i.e. did you eat more/less on the weekend day? Did you tend
to eat more regular meals on the weekdays…etc. Analyze why these patterns may exist. This part will depend on how well you took notes about your eating
habits. It will include an explanation about your style of eating (why you make your food choices…convenience, cost, cultural, taste preference,
nutritional, etc….)
Part 3: What will you do with this information?
Based on the above analysis of your food and nutrient intake AND based on what you have learned about nutrition and health, specifically address the changes
you would make to improve your nutrient and food intake. This section should take up close to a full page. Refer back to your assessment and explain how
current nutrient levels may impact your health if continued on a regular basis. Use your textbook and outline the types of health issues you might face if
you don’t make changes. Example: Saturated fat levels are 25% above the recommended. You would describe the health consequences you could face if you
continue to eat and excess of foods high in saturated fat. State the foods that contribute to these levels and what realistic dietary changes you can make to
decrease saturated fat in your diet.
If you choose to lose or gain weight in your profile, explain how your dietary changes will affect caloric intake, what physical activity you will add to
your daily routine, and how those 2 changes together will impact weight. Finally address how this assignment has helped you: Did you gain some practical
information that will be useful to you? What has been most eye-opening for you?
Include examples…include examples…include examples~! What foods you ate; what you will eat or will avoid to better meet your needs…BE SPECIFIC and realistic.
Students miss points only because they do not include real food examples (You need to say more than “ I will eat fruits and vegetables more often”…state
what kind and what nutrients they will provide.
We can write this or a similar paper for you! Simply fill the order form!
This assessment aims to apply the principles of effective leadership and change theory to a change or performance improvement strategy which is professionally relevant to the learner. The assessment needs to consider the implications for workforce development and the ways in which organizational culture may enhance or hinder the capacity to achieve sustainable change outcomes. It is asked to consider the role of the leader in developing workplaces which are able to meet the demands for change.
This is a formal academic essay where it is required to demonstrate a capacity to critically discuss either a change management process or performance improvement strategy. (**Remarks: use Hong Kong health care practice)
Essay topics:
Performance improvement
Choose one area that requires performance improvement within an area of health care practice (clinical- e.g. a skill or clinical process, managerial – e.g. leadership issue or team building, or education- e.g. related program to a particular performance/ activity you would like to see improved.)
Analyze & critically discuss the following key points:
The area of an organizational performance that is of concern and how it relates to the organization’s strategic goals and objectives.
The steps required to implement a process for improving this aspect of organizational performance
The approach best suited to improving performance in this instance.
The type of performance indicators or measures selected.
Strategies for motivating and engaging stakeholder in ongoing performance improvement.
Thanks!
SAMPLE ANSWER
Performance improvement plans or action plans help give struggling employees get the opportunity to succeed and at the same time make them accountable for their past performance. The poor performance of clinicians is not smooth on the presence of it. Various reasons can be brought forward on the reasons for poor performance. This can be whether the clinician received the appropriate training and their knowledge of the expectations of the job. Any unforeseen roadblocks for future achievements also facilitate performance improvement plans (Bonow, et al., 2012).
It is, therefore, critical for the departments of a healthcare practice to give room for an open dialog and feedback directly from employees. This helps in the determination of the extent to which employees are provided with the sufficient resources and tools necessary for their success. Performance improvement can be used to address the failures that are arising to issues related to performance and behavior. The outcome of the performance improvement plan can be improved the performance of the health workers in Hong Kong. Also, training gaps and recognition of skills of employees can be evaluated. Employment related issues that may result can lead to the demotion of individual employees, transfer of some and demotion of underperforming employees.
In Hong Kong health care practice, an employee who does not perform well to meet expectations can be corrected by their supervisors. The performance improvement plan can be used to replace the disciplinary processes. This helps correct workplace behaviors that affect productivity given that any action taken earlier is better compared to waiting for the result. The presence of employee relations staff help in consultation and providing any technical assistance to health supervisors and other clinical employees and services. Training can also be supplied in the course of the performance improvement plan (Ferrer, et al., 2014).
Area of organizational Improvement
People who practice medicine have a high potential in assisting patients to stop smoking. Deficits have been found concerning the amount and type of training these people receive when undertaking smoking cessation counseling whereby they little consider the training. This area ought to be improved in health care facilities so as to improve the levels of service delivery in health systems. Trials should be conducted to examine the relativity of effective Quality improvement. The difference in educational programs of Departments of health care of Hong Kong in teaching smoking cessation skills help in achieving this noble course of improving performance.
Quality improvement works as a systems and processes. To make improvements, the health care and clinical departments need to have a clear understanding of their systems and delivery of services. Quality improvement takes into account the relationship between the resources of the organization and the activities carried out will help achieve improved health care quality. The service delivery in health is typically straightforward, and an example in a dental clinic and on the other hand, a large managed care hospital requires complex systems (Eijkenaar, et al., 2013).
The senior trained medical students and practitioners should demonstrate their efforts in improving the performance through their intervention to reduce smoking. The educational purposes of medical students should expose them to smoking cessation and the efforts to help smoking patients. Specific training should be provided in order to increase the rate of success of the nursing students. Traditional methods will not be effective and embracing teachings of that are appropriate in nature in all levels of education will help the students achieve this noble course.
Focus on patients: This is another area of measuring quality improvement and the level to which smoking cessation is effectively done. Patient’s needs ought to be met in health care, and the society and beneficiaries of the clinical area can be that there should be systems that affect the level of access by patients. Patients do not expect to queue for long due to slow systems. Patients also expect to receive care from the clinics that are based on evidence. The health practitioners can be trained so that they are well conversant with the type of treatment that they provide as per the DOME clinical skills. Evidences on successful cessation can be used. (Hamric, et al., 2013).
Patients also should expect safety at the premises and, therefore, need to assure them of safety by ensuring that medical practitioners observe security in their areas of service. Safety can be both physical and provision of quality medicines. Support for the engagement of patients in the treatment process is critical because patients can be able to express their problems directly. Care is communicated and coordinated with other parts or departments of the health care system. Another measure could be to ensure cultural competence in the assessment of the literacy levels of patients and to ensure that care is linguistically appropriate to ensure client satisfaction.
Focus on being part of the team: Quality improvement is a team process, and thus, knowledge and skills are brought together. Differences in thoughts of individuals are combined to obtain lasting solutions, and this approach is most useful when the process of quality improvement is complicated, and not even one person has the clinical skills or issue at hand. Also, it is useful when the process involves more than one discipline or work area and thus leading to the creation of creativity so as to establish a lasting solution (Nicolay, et al., 2012).
Let us say an organization wishes to reduce smoking cessation by reducing the patient wait time in the health care, the efforts presented by a team will help the health care facility achieve a lasting solution to these problems. All individuals should contribute to the team to ensure proper analysis as per the DOME clinical skills. Members bring in different perspectives on an issue and on how to sustain the improvements. Quality improvement and the participation of the teams highly depend on the availability of infrastructure. These can be team leadership and procedures plus the policies of undertaking each activity (Hermann, et al., 2014).
Focus on use of data: The major activity in quality improvement of services in Healthcare is data because it mainly describes how well the existing systems to reduce smoking are working. It is also an indication of the outcomes of applying a new change and is useful when noting a success in performance. The use of data helps in separating what is happening actually from what people think. For example, the level of attendance of patients to the available number of clinical officers. Data is useful in setting up a baseline whereby performance at that baseline is acceptable and deemed fit. Scoring low at the first episode can be accepted with an anticipated improvement in subsequent results. It also helps in the reduction of solutions not useful from being placed be the supervisors.
Procedural changes can easily be monitored, and this helps make sure that the resulting improvements can be sustained. The clinicians and nurse should be able to cope with the improvements in helping smoking patients and give an indication if the changes affected have shown any improvement in their service delivery. Performance can easily be compared to all the departments, and, therefore, patients and staff satisfaction surveys can easily be conducted (Witter, et al., 2012). Quality improvement will help achieve improved health of patients and efficiency in managerial and clinical processes. It also helps avoid costs that are associated with failure of processes and errors thus leading to a balance of quality in Hong Kong health care services (Unützer, et al., 2012).
Steps to implement the process
The first step is to document the performance issues. The issue being a quality improvement in health care, it is good to develop a format or use existing ones to ensure that consistency of values is observed. This helps protect the clinical heads if any legal claims are made in expectations. The performance plan will include information about the staff. These are their skills and training received to handle patients. Also, the dates should be expected and any performance gap should be indicated. Expected performance is described and compared with the actual performance and the plan of action designed by the team stated clearly.
The second step is to develop an action plan in the process of quality improvement. The quality of service provision is desired to be improved to match the DOME clinical skills and thus need to create a plan that suits those standards. An action plan can be established by the supervisors and request an expression of interests from employees to ensure that everyone agrees to it. Collaborative engagement makes it easy to solve issues and thus, creating database requires employee participation (Murray, et al., 2013). Some of the nursing and clinical tools can be included while others can be excluded depending on the mutual decisions. The consequences of not meeting the objectives are also set.
The third step is reviewing the performance plan in the organization. Quality improvement in the clinical case engages the top management and the supervisors. The director of a department should seek guidance from the senior manager or directors of health on matters documentation of the performance plan. This will help ensure that all the parties to the quality improvement project adhere to the requirements of the program and hence instill disciplinary activities to lazy clinical workers. It should be specific, attainable and relevant (Jha, et al., 2012).
The fourth step is meeting with the employees and, if possible, the other stakeholders including patients. A program might be in the process of its quality improvement, but the patients feel that lack sufficient knowledge of how to use the service. Here, the action plan can be modified to include specifications and proposals from the stakeholders. The nurses and clinical officers can then sign the personal improvement plan forms.
The fifth stage involves making follow ups. Both the employees and the supervisors should be holding meetings on designed basis to evaluate the level of improvement of the quality of service. The meeting should include discussions concerning the objectives and any matters arising are documented. The employees are expected to ask questions and go further to seek guidance on a particular step, for example, the introduction of online medicine payment and the establishment of booking systems. The nurses and clinicians are motivated towards producing the best in quality improvement (Santiago, et al., 2014).
The last step is concluding the process whereby non-performing employees who do not follow the quality improvement plan will experience poor performance. This is because the new system is taking over slowly. This can be a high time for him or her to request for reassignment to other departments of the clinic such as social work or can choose to be transferred. When the goals have been reached, the quality improvement plan can be done periodic reviews to ensure its flexibility in service provision and health care practices.
Approaches to Performance Improvement
Not all quality improvement strategies are successful although health care facilities seek to improve performance. The first approach is through the system view. The best acceptable approach in quality improvement should be taken using Systems Thinking techniques that help in the identification of activities that are reducing the ability of the clinical skills from being achieved. Operations analysis can be used to ensure the maximum improvement of quality all through the performance improvement phases. This will enable focus on development that brings change to the health care departments (Toussaint, et al., 2013, January).
People involvement is an approach because any quality improvement’s success depends on the efforts of people at all the improvement levels. All the employees including the social workers and nurses plus clinical officers should be at the front line and involved in the decision-making process. Most of the failed quality improvements as per DOME clinical skills is as a result of ignorance. The lead supervisors should include other employees in the decisions to undertake quality improvement. This results in failed efforts of the management. Engaged workers will feel the ownership of the quality improvement process and thus enabling them to become owners of the project (Haas, et al., 2013).
Another approach to ensuring quality in health care is improved is to focus on the process involved. Focusing on the process is the best approach compared to building up blames due to lapses. Maybe some of the health workers and clinicians do not come to their jobs on a daily basis which is an indicator of failed implementations. The new process will help promote the operations and patient attendance and achieving the quality improvement goals. The improvements in quality require that people within the health care change their behavior and focus on the process to suit the new quality improvement plans for the clinics.
The purpose of the quality improvement should be evaluated and defined. Here, it is to improve service delivery to the patients while reducing the queuing of these patients. The process involves all the levels of management in Hong Kong health care, and thus, definition of the existing system and the available staff plus patients is important. The value of service offered by the clinic is critical and customer satisfaction should be measured. In a clinical case, the primary customers are patients and therefore there is a need to ensure that the level of services offered to them is satisfactory (DeRenzi, et al., 2012, March).
The value stream is important in the determination of the entity’s value creation to the patients through the existing Value Stream Analysis set aside by the quality improvement team. At a strategic level, the firm is analyzed and compared to the tactical level of individual departments in the clinical case. People performing value stream such as nurses should be included, and this carries a short period.
An improvement plan will be produced by the value stream whereby actions are categorized according to the ability of undertaking. Others can just be done while others will follow the rapid improvement events. The achievement of these goals should include involvement in the process of implementing the quality improvement to people. It values the current ways of job performance while reducing the discrepancies in the process of improving the quality of health care services. The last approach base is to sustain the improvements in the quality of services. Key metrics plus the loops for controlling quality improvement are planned with an aim of ensuring that health workers adapt to the new changes in the system (Källander, et al., 2013).
Performance Indicators
Monitoring the quality improvement is facilitated by the indicators, and they help to create the basis for improving the quality of health care practice and the modified system. The indicators need to be designed and defined so as to enable its implementation in agreement with medical practices. A rate based index will use the data concerning the events unfolding and their occurrence at the same frequency. These are the rates and proportions with which the quality improvement project has satisfied the patients in the hospital. The trends over the years will indicate the speed with which the performance improvement has been active (Kern, et al., 2014).
The sentinel indicators will help in identifying the individual events such as patient waiting time and its improvements. This helps in triggering further alterations to the performance improvement plan of quality. It will show the poor performance as a comparison to the past clinical skills performance. Process indicators will show the actual performances and what has been done while giving and receiving care by patients and clinicians. It helps indicate what the clinicians attended to the patients and the quality it was done. The care that health care provider’s accord to patients and the limits of the stipulated period all through the process according to dome clinical skills are included (Unützer, et al., 2014).
Structural indicators such as health system characteristics and quality improved will affect the quality of the improved system to meet the needs of healthcare of patients. It will help in describing the amount of resources used by the quality improvement system of the organization in delivering the services and programs. These systems are directly related to the health care performance improvement system and are affected by the number of the staff dispatched to the new system. Resources concerning money, the beds in the health care and the supplies plus the wards or buildings for in-patients are analyzed (Jha, et al., 2012). This will help in judging the quality of care provision under conducive to the quality of health provision in Hong Kong.
Outcome indicators assist in showing the health states and events that follow the quality improvement program in the health care system. This includes the possible effects of the new system on both patients and the health workers. It captures the potential impact of the policy on the health improvement and performance of patients. The worst outcome of the quality improvement is death. This results from untimely or naive implementation. Another outcome is the possibility of disease outbreak and its symptoms and abnormalities. Discomfort can result from the quality improvement process, and these may include nausea and dyspnea. Disability is another possible outcome, and it can present itself in the form of impaired recreation. The patients can also be dissatisfied with the quality of service and can lead to persistent complaints.
Adjusting to these indicators can involve the factors that are contributing to the survival of patients in the clinical process and the outcomes of the health quality improvement. The results of the quality improvement can be adjusted in comparison to other factors not within the health care system through quality assessment and other factors or components that are about quality health care. Demographic factors of the patients such as age and sex are considered. The lifestyle of the patients and psychosocial factors plus compliance to the prescribed medication can affect the quality of outcome. The severity of the illness and its comorbidity should be considered in the outcome evaluation (Groves, et al., 2013). The quality of treatment and the competence plus technical equipment available and the evidence-based treatment can affect quality. Adherence to using the clinical guidance available and cooperation from the top medical stakeholders is essential.
Strategies for Motivating and Engaging Stakeholders
Despite the advances in the quality improvement through healthcare in performance improvement, there is a failure in reliability from the customers as a result of health care. The systematic increase in health workers’ complexity and hard work does not guarantee efficiency in health care provision. Fixing these problems require transformations in systems to a team-based services aimed at satisfying the customers.
Engagement in the shared purpose of the quality improvement in clinical skills involves leaders’ shift of conversation to achieving the articulated visions and improved patient care. The need for sacrifice should be embraced because the performance improvement process can reduce autonomy and income levels of physicians. Leaders should encourage health workers to change the mentality of maintaining the status quo to advanced medical services (Friedberg, et al.,2014). The needs of the patients need to be prioritized, and doctors cannot be shielded from this.
Consensus needs to be built to allow the views that are varied to be articulated. An appeal to self-interest is essential given that physicians need to be motivated through financial incentives. The measures of performance should be realistic and non-biased o reinforce engagement of the health workers. The compensation can be pledged depending on the quality of improvements per individual. The successful health workers can be communicated to through earning them respect from their duties. Role play is appreciated through the positive feedback from the top management as no employee yearns to lose respect from colleagues.
The tradition of the health care and clinical practice of the physicians should be valued as a member of the health care system. They are given motivation so that they can adhere to the standards and traditions of the organization. Dome clinical skills tradition has been followed by doctors, and they are required to wear hosiery for female physicians and neckties for male medical practitioners (Reeves, et al., 2013). The patients can be engaged by the provision of training on the ease of access to certain technological improvements. Mass education can be carried out and the patients given sessions to express their levels of satisfaction. With this, the entire process of quality improvement in performance improvement of health care can be achieved.
References
Bonow, R. O., Ganiats, T. G., Beam, C. T., Blake, K., Casey, D. E., Goodlin, S. J., … & Masoudi, F. A. (2012). ACCF/AHA/AMA-PCPI 2011 Performance Measures for Adults With Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures and the American Medical Association–Physician Consortium for Performance Improvement. Journal of the American College of Cardiology, 59(20), 1812-1832.
Ferrer, R., Martin-Loeches, I., Phillips, G., Osborn, T. M., Townsend, S., Dellinger, R. P., … & Levy, M. M. (2014). Empiric Antibiotic Treatment Reduces Mortality in Severe Sepsis and Septic Shock From the First Hour: Results From a Guideline-Based Performance Improvement Program*. Critical care medicine, 42(8), 1749-1755.
Eijkenaar, F., Emmert, M., Scheppach, M., & Schöffski, O. (2013). Effects of pay for performance in health care: a systematic review of systematic reviews. Health policy, 110(2), 115-130.
Hamric, A. B., Hanson, C. M., Tracy, M. F., & O’Grady, E. T. (2013).Advanced practice nursing: An integrative approach. Elsevier Health Sciences.
Nicolay, C. R., Purkayastha, S., Greenhalgh, A., Benn, J., Chaturvedi, S., Phillips, N., & Darzi, A. (2012). Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. British Journal of Surgery, 99(3), 324-335.
Hermann, R. C., & Palmer, R. H. (2014). Common ground: a framework for selecting core quality measures for mental health and substance abuse care.Psychiatric Services.
Witter, S., Fretheim, A., Kessy, F. L., & Lindahl, A. K. (2012). Paying for performance to improve the delivery of health interventions in low-and middle-income countries. Cochrane Database Syst Rev, 2(2), CD007899.
Unützer, J., Chan, Y. F., Hafer, E., Knaster, J., Shields, A., Powers, D., & Veith, R. C. (2012). Quality improvement with pay-for-performance incentives in integrated behavioral health care. American Journal of Public Health,102(6), e41-e45.
Murray, C. J., Richards, M. A., Newton, J. N., Fenton, K. A., Anderson, H. R., Atkinson, C., … & Braithwaite, T. (2013). UK health performance: findings of the Global Burden of Disease Study 2010. The lancet, 381(9871), 997-1020.
Jha, A. K., Joynt, K. E., Orav, E. J., & Epstein, A. M. (2012). The long-term effect of premier pay for performance on patient outcomes. New England Journal of Medicine, 366(17), 1606-1615.
Santiago, J. M. (2014). Use of the balanced scorecard to improve the quality of behavioral health care. Psychiatric Services.
Toussaint, J. S., & Berry, L. L. (2013, January). The promise of Lean in health care. In Mayo Clinic Proceedings (Vol. 88, No. 1, pp. 74-82). Elsevier.
Haas, L., Maryniuk, M., Beck, J., Cox, C. E., Duker, P., Edwards, L., … & McLaughlin, S. (2013). National standards for diabetes self-management education and support. Diabetes care, 36(Supplement 1), S100-S108.
DeRenzi, B., Findlater, L., Payne, J., Birnbaum, B., Mangilima, J., Parikh, T., … & Lesh, N. (2012, March). Improving community health worker performance through automated SMS. In Proceedings of the Fifth International Conference on Information and Communication Technologies and Development (pp. 25-34). ACM.
Källander, K., Tibenderana, J. K., Akpogheneta, O. J., Strachan, D. L., Hill, Z., ten Asbroek, A. H., … & Meek, S. R. (2013). Mobile health (mHealth) approaches and lessons for increased performance and retention of community health workers in low-and middle-income countries: a review.Journal of medical Internet research, 15(1).
Kern, R. S., Liberman, R. P., Kopelowicz, A., Mintz, J., & Green, M. F. (2014). Applications of errorless learning for improving work performance in persons with schizophrenia. American Journal of Psychiatry.
Unützer, J., Schoenbaum, M., Druss, B. G., & Katon, W. J. (2014). Transforming mental health care at the interface with general medicine: report for the presidents commission. Psychiatric Services.
Groves, P., Kayyali, B., Knott, D., & Van Kuiken, S. (2013). The ‘big data’revolution in healthcare. McKinsey Quarterly.
Reeves, S., Perrier, L., Goldman, J., Freeth, D., & Zwarenstein, M. (2013). Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev, 3.
We can write this or a similar paper for you! Simply fill the order form!
A patient has been admitted to the mental health unit with a diagnosis of bi-polar disorder. During a meeting the family inquires about the use of alternative therapies. Based on your readings and knowledge discuss what the RN would teach the patient and family and incorporate modalities, usefulness, effectiveness and how to increase compliance with therapeutic modalities
Alzheimer’s is a condition that is increasing in incidence in our population. There is no differential diagnosis so the start of the disease may go unnoticed. Once the manifestations become more apparent it often places a tremendous strain on the caregiver. Caregiver role strain is a nursing diagnosis that is frequently applied in the situation. Since patient wandering and confusion are common for the patient with Alzheimer’s disease what would the RN teach the family about maintaining a safe environment? Discuss the support systems that are available to families
SAMPLE ANSWER
Mental Health: Alzheimer’s Disease
Memory loss is a critical manifestation of Alzheimer’s syndrome. The condition places patient at the risk of harm from the environment. For instance, impaired memory would predispose people to practices such as leaving their electrical appliances running and unattended. Teaching care givers on approaches of protecting their patients would be a necessary health management plan.
Registered nurses should teach families of Alzheimer’s patients to keep abreast with their loved ones. Families should know their role on monitoring their patients so that they do not hurt themselves when performing basic duties such as cooking and driving. Also, families would be advised to promote the safety of their patients’ environment by installing appliances that can shut automatically when left unattended (US National Institute of Health, 2010, Pg. 14). The nurses would also advise patient families to limit the exposure of their loved ones to wandering as the practice would place them at the dangers of getting lost or encountering accidents. Families would do so by providing the needs that would motivate patients to wander.
Caring for Alzheimer’s disease patients is often challenging for families. It is therefore necessary for them to seek support systems for the activity. Available support systems include voluntary groups and friends who would offer to help for services such as cleaning and shopping for the patients (Robinson, Wayne, & Segal, 2015). Healthcare professionals would also be of substantial support as they would help families to monitor the progress of their patients. In addition, families could exploit support systems such as workshops that train people on care giving skills (Robinson, Wayne, & Segal, 2015). Other approaches include exploring online materials and books that address the management of Alzheimer’s disease.
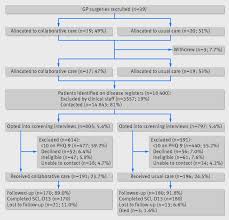
linked item M6A3: The comparison of collaborative care for a patient with a mental health disorder versus a patient with a medical disorder in the acute care setting Paper
Using APA format, write a six (6) to ten (7) page paper (excludes cover and reference page) that addresses the comparison of collaborative care for a patient with a mental health disorder versus a patient with a medical disorder in the acute care setting. The paper consists of three (3) parts and must be submitted by the close of week six. Each part must be a minimum of two (2) pages in length.
A minimum of three (3) current professional references must be provided. Current references include professional publications or valid and current websites dated within five (5) years. Additionally, a textbook that is no more than one (1) edition old may be used.
The following topics may be used for this paper:
Mental Health Disorders
Post traumatic stress disorder (PTSD)
Bipolar
Depression
Paranoid Schizophrenia
Anorexia
Attention deficit hyperactivity disorder (ADHD)
Alzheimer’s disease
Medical Disorders
Hypothyroidism
Addison’s Disease
Cirrhosis
Acute Pancreatitis
Chronic Renal Failure
Pylelonephritis
Type 1 Diabetes Mellitus
Part 1
Select one (1) mental health disorder and one (1) medical disorder covered within the modules of NUR212 as a basis for your paper. (It must be a disorder that is covered in the content of this course. Other disorders will not be graded.) Compare the two (2) disorders demonstrating similarities and differences.
Discuss how the efforts and resources required to manage the disorders compare to one another. Is the burden a patient with a mental health disorder endures comparable to the burden experienced by a patient with a medical disorder? Explain your response.
Identify two (2) issues that may arise for the patient and/or family when caring for the patients with the identified disorders. Provide two (2) descriptive examples.
Part 2
Identify ethical and legal implications the RN considers when caring for patients with a mental health disorder and medical disorder.
Discuss similarities and differences in the RN’s approach to address the identified implications.
Part 3
Based on the disorders chosen above, adress the following:
Provide an example of how the interprofessional team members can provide collaborative and continuous care in the acute care setting.
Discuss the role of the professional nurse within the team and provide three (3) examples.
Describe how to ensure adherence to medication regimen and follow-up visits – Provide three (3) examples.
What measures would evaluate the effectiveness of the interprofessional plan of care?
How does the RN evaluate the interprofessional team efforts and identify modifications that might be necessary?
Any topic chosen that is not covered within the context of this course, will not be accepted.
Compose your work using a word processor (or other software as appropriate) and save it frequently to your computer. Use a 12 font size, double space your work and use APA format for citations, references, and overall format. Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page. Assistance with APA format, grammar, and avoiding plagiarism is available for free through the
SAMPLE ANSWER
Part One
Diabetes mellitus is a lifelong condition that affects the patient ability to regulate glucose levels. When a person ingests food, the body breaks down the food into carbohydrates and glucose. The glucose is used to fuel the cell activity. This process requires the use of insulin in order for a cell to convert glucose into energy. With diabetes mellitus, the body does not secrete enough insulin or the receptors become faulty and are unable to absorb the insulin. This causes glucose to build up in the blood, which causes damage to the other parts of the body including kidney, eyes, heart and the nervous systems (Standards of Medical Care in Diabetes—2014, 2013). The signs and symptoms of diabetes mellitus include reduced appetite, increase urine output and general body weakness or fatigue. The diagnosis of this disease is done using glucose tolerance test and also testing of the glycosylated hemoglobin (Standards of Medical Care in Diabetes—2014, 2013).
According to NICE, patients diagnosed with diabetic are three fold likely to be diagnosed with depression. Depression is a mental disorder that affects a person’s health and their ability to self manages their healthcare condition. Research indicates that depression have great risk to suffering from episodes of diabetic burnout, which can effect their health adversely. Depression is the medical term that is used to describe people with the following symptoms. To start with, they have persistent anxiety, sadness and a prolonged feeling of hollowness. The patient feels helpless, powerless and hopeless. This makes them lose interests of activities that they perceived, insomnia, memory problems and weight changes (Ennis & Bunting, 2013).
The relationship between depression and other health complications is not fully understood. However, the rigors of managing the disease is not easy and could cause the condition to get worse, leading to more health complications. Depression can cause poor management of lifestyle decisions resulting to less exercise, drug use and binge eating. This affects the person abilities to perform their duties or even to perform their tasks as they used to. The non-therapeutic resources used to manage diabetes mellitus and depressions are similar. For instance the programs used to manage the two conditions include activities that will improve lifestyles, such as increase of fitness, weight management strategies, nutrition balance and exercises. These programs help the patient remain in good shape, which improves their self esteem and the patient diabetic condition (Ennis & Bunting, 2013).
The major difference is in therapeutic management process. This is because diabetes mellitus is managed using glycemic control including drugs such as Biguanides, Thiazolidinediones (TZDs), Meglitinide derivatives and insulin’s among others. The management of depression takes time but it can effectively be managed. The common treatments includes the Cognitive behavioral Therapy (CBT), a type of psychotherapy that helps change the negative mentality, as well as lifestyles that contribute to depression. The use of Selective serotonin reuptake inhibitor (SSRI) is a therapeutic management that involves the use of antidepressants including the Celxa, Sertraline (Zoloft) and Prozac. Other types of antidepressants that can be used include the Serotonin and norepinephrine reuptake inhibitor (SNRI) among others (Ennis & Bunting, 2013).
Generally, mental health is more debilitating than the acute diseases. Research indicates that person diagnosed with depression is 50% likely to become disable than patients suffering from the chronic diseases angina, arthritis or even diabetes mellitus. This is because mental pain is real that and more severe than the physical pain. The hustle for mental illness is real as most of the mentally ill patients are not accessing care as compared to those with medical conditions. Approximately, three quarters of these individuals are not able to access care. This is especially so, because the NHS commissioners have not commissioned mental health appropriately. For instance, when people suffering from physical condition undergo treatment, their treatment usually include the treatment psychological therapy. Psychological therapy in physical treatment especially in chronic diseases is emphasized than in the mental disorders treatment (Standards of Medical Care in Diabetes—2014, 2013).
The main issues that arise during the management of these health disorders are financial burden. This is because diabetes and depression are long term diseases that require a lot of resources including attending of the lifestyle modification programs. This is a challenge considering that chronic disease and mental disorders are inadequately covered by the public medical covers. This could be costly to both the patient and the family (Ennis & Bunting, 2013). The other issue that could arise is lack of effective training on how to handle the patients. In most of the public hospitals, patients and the care givers are not trained on how to manage the transition from the healthcare facility. There are not told about what is available for their management of care and what is not. This miscommunication between the patients, caregivers/ families and healthcare providers is a huge challenge that must be addressed (Barr, 2010).
Part 2 Registered Nurse Ethical and legal implications
In these healths setting, the registered nurses have ethical and legal guidelines used during their practices. There are six ethical principles applied by RN when making ethical decisions about their care. These include respect for the patient. RN is expected to support the patient. This includes empowerment and respecting patient’s choice (Autonomy) (Perreault, 2011).
The decision made by the registered nurses must be with the aim of improving patient’s condition by doing well (beneficence) and with the aim of avoiding harm (nonmaleficence). The ethical decision must be made with fairness, truthfulness and equitably (justice). The registered nurse must remain veracious and faithful to their commitment. The registered nurse is expected to make their decisions during care as indicated by the American Nurses Association’s nurse’s code of ethics. These standards are delineated registered nurses across the settings (Barr, 2010).
Some of the ethical concerns that arises these care is balancing the nursing attitude care with compassion, and simultaneously recognizing as well as sustaining the patient-healthcare boundaries. Another ethical concern for registered nurses is to ensure that these patients can access care. The registered nurses have the responsibility of acting as patients advocates, especially in ensuring that their care directives are respected and also in elimination of the healthcare hindrances (Barr, 2010).
End of life care is also an ethical concern for the registered nurses. The registered nurses have the responsibility of ensuring that their patients die with dignity.
The legal implications of nursing include the issues of licensure as stipulated by the federal and states laws. These licensures have delineated registered nurse scope of practice as well as the public expectations. The nurse level of education and the licensure gives the framework by which the registered nurse is expected to practice. These frameworks are to ensure that their practice does not fall below the accepted and expected standards of nurse care, which could expose the RN to litigation (Perreault, 2011).
There are no differences in the ethical and legal implication for RN for the physical disorder (diabetes mellitus) and the mental disorders (depression). The basis for RN litigation is if the patient can prove that the nurse’s actions were due to negligence to perform what is expected of them by the ANA code of ethics and nurse practitioners standards. These includes acts of omission and commission could subject the RN to have their licensure reviewed and to litigation (Perreault, 2011). Regardless of the method or approach of care, the RN has legal as well as ethical obligation to respond to patient’s demands. This implies that the RN should attend to the patient, assess the patient’s demands and the magnitude of care demands. The RN should conduct the family health assessment and cultural health assessment to ensure that the care provided is culturally sensitive. Based on the data generated from the assessment of the patient, then the RN can determine the level as well as the type of interventions are required, develop a care plan and implement it. The RN should contact higher level of healthcare where necessary, including offering referrals (Barr, 2010).
Part 3
The inter-professional teams refer to the collaborations between the various healthcare staffs, with the aim of attaining the common goals of delivering quality and safe care. This is beneficial as the healthcare staffs divide their chores according to the scope of their practice. This reduced the events that the healthcare staffs become burnout. Additionally, inter-professional team facilitates the sharing of information. This coordination and supports ensures that the interventions proposed are ethical and legitimate (Axon et al., 2008).
Inter- professional team faces many barriers. This includes lack of understanding of the major roles, which reduces respect between the healthcare team. The nurses have a key role in collaborating between the healthcare inter-professional team. They are required to possess facilitation skills to ensure that they work collaboratively with the patients and the healthcare staff. This is to ensure that the teams have updated information about the patient and their preferences. For example, the nurses are the healthcare professionals who spend most time with the patients. Therefore, the nurses are expected to deliver around the clock care and record the observations (Pope & Casarett, n.d.).
The nurses are also responsible in ensuring that the physician’s directives are implemented. These include administering of medications and assessment of patients responses to the treatment plan. The nurses is also responsible for the evaluation of the patients medical plan efficiency and safety. They should interpret patient’s information to help the healthcare providers to make the appropriate decisions. Therefore, the nurses roles in the inter-professional team is to assess patient psychological, social, cognitive as well as spiritual needs , and to advocate for the patients wellness as well as facilitating optimal health for the patient. They are also responsible for patient education (Axon et al., 2008).
Through patient education, the patient understands the importance of adherence. There are five interacting factors if medication adherence that have been described by the World Health Organization (WHO). These include factors related to therapy, patient’s behaviors, socioeconomic factors and medical condition factor. Evidence based research identifies strategies to improve the medication adherence. The social and economic factors that can be addresses include lack of health literacy, communication barriers, low socioeconomic status and lack of medical cover. The nurse must learn the cultural beliefs to ensure that they can assist the patients (Axon et al., 2008).
Therapy related factors include complexity in therapy such as mastery of various techniques such as use of inhalers or injections. The unpleasant benefits, prolonged use and interferences are other causes of poor medication adherence. The patient related factors include the cognitive impairment and swallowing difficulties. The nurses need to address psychological issues such as confidence in following treatment, as well as making the patient understand the benefits of medication. Empowering the patient improves their confidence as well as the ability to follow their treatments despite the perceived risks (Pope & Casarett, n.d.).
Evidently, team effectiveness questionnaire is a tool that can be used to evaluate the effectiveness of working as a team. This tool consists of about 25 items which evaluates the effectiveness of the interprofessional team I relation to four main dimension including communication, organizational efficiency, healthcare practices such as staff development, EBP and patient centered care. The interprofessional collaboration scale may also be used to assess the interprofessional’s perceptions including the nurses, physicians and the other relevant healthcare professionals. This tool is a 13 item scale that is adapted from the Nurses Opinion Questionnaire. Other evaluative techniques include the evaluation of quality healthcare indicators such as readmission rates, patient’s falls, hospital acquired infections and the length of hospitalizations. These strategies will help identify the gap in inter-professional team, leading to effective interaction between the healthcare staff (Axon et al., 2008).
References
Axon, A., Hassan, M., Niv, Y., Beglinger, C., & Rokkas, T. (2008). Ethical and Legal Implications in Seeking and Providing a Second Medical Opinion. Dig Dis, 26(1), 11-17. http://dx.doi.org/10.1159/000109379
Barr, H. (2010). Understanding Interprofessional Working in Health and Social Care. J Interprof Care, 24(4), 470-471. http://dx.doi.org/10.3109/13561821003761465
Ennis, E., & Bunting, B. (2013). Family burden, family health and personal mental health. BMC Public Health, 13(1), 255. http://dx.doi.org/10.1186/1471-2458-13-255
Perreault, K. (2011). BOOK REVIEW Interprofessional Teamwork for Health and Social Care. Scott Reeves, Simon Lewin, Sherry Espin and Merrick Zwarenstein, Wiley-Blackwell (2010), 191 p. Physiotherapy Theory And Practice, 27(8), 595-596. http://dx.doi.org/10.3109/09593985.2011.599052
Pope, T., & Casarett, D.(n.d.). Ethical and Legal Obligations of Hospice Staff When Their Patients Receive Aid in Dying. SSRN Electronic Journal. http://dx.doi.org/10.2139/ssrn.2338095
Standards of Medical Care in Diabetes–2014. (2013). Diabetes Care, 37(Supplement_1), S14-S80. http://dx.doi.org/10.2337/dc14-s014
We can write this or a similar paper for you! Simply fill the order form!
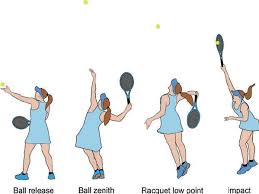
Paper instruction : Tennis serve
Descrition of the Motor skill : Beginning Phase, Middle Phase, Final Phase( Anatomical analysis:Muscle participation and form of contractions. )
*NO Websites and online database (wikipedia) are accepted; Google scholar web search preferred.
*No Instruction No conclusion needed. Just directly talk about the subject in detail.
SAMPLE ANSWER
Anatomical Analysis of Tennis Serve
The Beginning Phase
The stage involves player’s preparation for the serve. Different muscle activities take place in four phases. At the initial phase, there is minimal involvement of the shoulder and scapular muscles (Kovacs & Ellenbecker, 2011, Pg. 506). The player proceeds to the release phase where there is little activation of the left erector spinae but increasing participation of the right erector spinae muscles. Trunk stabilization is crucial at the stage and lower trunk muscles are activated to stabilize the lumbar spine. Muscles activated include rectus abdominis and internal and external oblique muscles. In the third phase, the player generates potential energy by properly positioning the feet. The foot-up and foot-back techniques are the commonest techniques, and they involve knee joint extensor muscles to a significant extent. In the foot-up technique, the posterior compartment of lower limb muscles offers upward and forward drive for the player. On the other hand, the anterior compartment offers stability for rotational momentum (Kovacs & Ellenbecker, 2011, Pg. 506). The same events occur in the foot-back technique, but there is more contraction of the knee joint extensors than in the foot-up technique. The third phase also involves a lateral rear tilt of the pelvis and the shoulder. The activity generates angular momentum for lateral flexion of the trunk. For right-handed servers, the ipsilateral erector spinae muscle activation is higher than that of contralateral erector spinae (Kovacs & Ellenbecker, 2011, Pg. 506). The left lateral erector spinae plays significantly in lateral flexion of the trunk during the third phase. Iliocostalis and longisimus dorsi are also active during the phase. They contract unilaterally to flex the lumbar vertebral laterally. The fourth phase begins with the activation of serratus anterior (Kibler, Chandler, Shapilo, & Conuel, 2010, Pg. 747). The upper trapezius muscle is then activated resulting in acromion elevation and stabilization of the scapular. The activation of the lower trapezius later enhances scapular stabilization and elevation of the acromion (Kibler et al., 2010, Pg. 747). The deltoid and supraspinatus are also activated to depress the head of the humerus and control external rotation.
The Middle Phase
The phase involves acceleration, and muscle activity exceeds the one in the beginning phase (Kibler et al., 2010, Pg. 747). For the internal humeral rotation, activated muscles include the serratus anterior, latissimus dorsi, subscapularis, and pectoralis major (Kovacs & Ellenbecker, 2011, Pg. 507). The first phase of the middle phase ends with the activation of the gastrocnemius, vastus medialis, and vastus lateralis. Both the trunk and legs coordinate to generate the greatest kinetic energy for the middle phase. The last stage of the middle phase involves minimal extension of the knee, wrist, and elbow joints. Rectus abdominis participates actively during this phase (Chow, Park, & Tillman, 2009). The phase also involves increased activation of rectus abdominis and external oblique muscles that are mostly involved in trunk flexion. Internal oblique is mostly activated during twisting of the trunk.
The Final Phase
The stage involves deceleration and follow-through. The infraspinatus is activated, and it contributes as an assistive muscle for humeral deceleration and distraction of the shoulder joint (Kibler et al., 2010, Pg. 747). The posterior rotator cuff is also activated together with biceps brachii, serratus anterior, latissimus dorsi and deltoid. The right erector spinae is also more active than the left erector spinae during deceleration. Deactivation of the anterior deltoid precedes that of other muscles. During the final phase, internal rotation and horizontal adduction are not needed. The serratus anterior and upper trapezius muscles are the next on the trend and their deactivation occurs as the acromial elevation decreases (Kibler et al., 2010, Pg. 747). The deactivation of infraspinatus occurs as humeral rotation decreases. Complete restoration of posture results following the activity of the lower trapezius for the scapular, supraspinatus and teres minor for the humeral head, and posterior deltoid for the upper arm (Kibler et al., 2010, Pg. 747).
References
Chow, J. W., Park, S.-A., & Tillman, M. D. (2009). Lower trunk kinematics and muscle activity during different types of tennis serves. Sports Medicine, Arthroscopy, Rehabilitation, Therapy, and Technology : SMARTT, 1, 24. http://doi.org/10.1186/1758-2555-1-24
Kibler, W. B., Chandler, T. J., Shapilo, R., & Conuel, M. (2010). Muscle activation in coupled scapulohumeral motions in the high performance tennis serve. British Journal of Sports Medicine, 41(7), 745-749.
Kovacs, M., & Ellenbecker, T. (2011). An 8-Stage Model for Evaluating the Tennis Serve: Implications for Performance Enhancement and Injury Prevention. Sports Health, 3(6), 504–513. http://doi.org/10.1177/1941738111414175
We can write this or a similar paper for you! Simply fill the order form!