SLP: Second Part
Many healthcare programs have modified their operational design and culture to one of being patient-centered while being fiscally viable. As part of your interview of a healthcare manager or executive selected for module 1 discuss how the program was or will be transformed to be patient-centered.
In your discussion please address the following questions.
1. How was the program restructured or re-engineered to adapt to internal and external factors impacting it?
2. What internal and external factors were considered in the transformation?
3. What were the barriers or obstacles were encountered (e.g. internal politics, economics, resource limitations, time constraints, etc.).
4. What is the potential impact on the program of technology, legislation, etc on the services provided on the program.
We can write this or a similar paper for you! Simply fill the order form!
The scenario based on the topic is: Houston Methodist St. John Hospital patient satisfaction scores have decreased over the past year.
A general description of the training topic.
Why this training is needed.
Who is to be trained.
How many are being trained.
Develop a training needs analysis for your topic (3–4 pages). For the purposes of this project, you are not expected to actually conduct the training needs analysis (TNA). Instead, create the following information as if it is based on a TNA.
Identify what the trainees should know or be able to do after they have completed the training program. Research your topic to determine what you want your trainees to learn. Your sources might be anything from an Internet search for data, to a meeting with subject matter experts (SMEs) who are good at the task involved. For example, if you training topic is how to tile a wall, you might search the Internet for do-it-yourself instructions, or you might consult with a specialist at a home improvement store.
Summarize the results of your research or provide a set of the questions you would ask SMEs if you were to meet with them.
Identify what the trainees know or what they can do before the training.
Create a sample survey, a questionnaire, a set of interview questions, or an observation checklist. Include this in your assignment submission as a separate attachment.
Develop training objectives for your training program (1–2 pages). Create 3–5 specific training objectives for your topic.
Create your objectives based on what you have determined the trainees should know (or be able to do) after attending the training program.
Design a training program for your topic (3–4 pages). Define each of the following aspects and explain why you made the choices you did.
How long will the training program be?
Will there be one or more training sessions?
Will those who facilitate the training be internal or external instructors?
Where will the training program be held?
How will learners be motivated to learn?
Who is the intended audience for the training?
SAMPLE ANSWER
Introduction
Patient satisfaction remains a significant and commonly used indicator that many medical facilities incorporate in measuring the quality of health care services they offer to patients. It is imperative to realize that patient satisfaction has the capacity to affect the retention of patients, medical malpractice complaints, and clinical outcomes (Hall, Shirey, & Waggoner, 2013). It also impacts the efficiency, timely, and patient-centered delivery of quality health care plan.
The Houston Methodist St. John Hospital in its delivery of services to the community has realized a decrease in patient satisfaction scores over the past years, a factor that has reduced the retention levels of patients in the medical facility (Hall, et.al). In order to address the issue, the management of the hospital embarks on a mission to develop a training program aimed at targeting the analytical needs that are designed to identify the background, motivations and expertise that can be employed by the learners to improve the condition of the hospital.
General description of the training topic
Houston Methodist St. John Hospital has realized the need to improve the quality of health delivery. The hospital in solving this issue is striving to define and measure the quality of healthcare provision in order to improve patient satisfaction scores. This comprehensive training program is therefore aimed at educating the medical practitioners within the institution in sound methodologies that can be employed in improving patient satisfaction (Hall, et.al).
The training program is therefore based on the concepts of practical improvements that require sound local evidence that determines the nature of the existing problem and risks and also considering the possible solutions. Inclusive of the training program is the systematic analysis of the specific interventions that can be employed and that fit within the medical facilities context.
The need for Training
It is essential to note that this training program is a vital element for Houston Methodist St. John Hospital. The essence of the program is on improving patient-physician communication. It has been discovered that patient-physician communication is a primary contributor to reduced patient satisfaction. Patient-physician communication has been a challenge, and if improved, a tremendous opportunity for improvement is likely to be noticed (Hall, et.al).
Studies have determined that when in patients are asked to identify the physicians who are in charge of their care during their times of discharge, close to 90% of the patients are unable to identify and correctly name the doctors responsible (Hall, et.al). When it turns to orthopedic patients, challenges are even more intense since these patients are mostly admitted to the emergency departments and are identified as unable to identify their treating physicians.
It is important to notice that the acuity of some orthopedic injuries may not allow some patients and their surgeons to establish a concise and strong patient-physician relationship prior to surgeries (Otani, Herrmann, & Kurz, 2011). In such a setting, it may be difficult to address patient concerns and priorities as a result of the differences that exist between surgeons and patients, a factor that results in low patient satisfaction. However, when there is an active inbound relationship between a physician and a patient, the patients are more likely to be satisfied, a factor that results in better outcomes.
The other need for this training is on finding better approaches geared towards improving the satisfaction of patients in the medical facility. The Houston Methodist St. John Hospital is therefore working out on the sound modules that can be employed in training to enhance patient satisfaction among their patient population by ensuring that medical practitioners are trained on effectuating their communication approaches on patients (Otani, et.al). It is anticipated that after training, there will be improved physician recognition and enhanced communication between the patients and their physicians, a factor that will increase the patient satisfaction scores.
The management of patient expectations and psychosocial factors such as depression and pain that have the capacity to drive patient satisfaction may prove to be challenging. However, through an individualized patient preoperative counseling approach and a shared decision-making, medical practitioners are likely to identify the specific factors that affect patients such as chronic pains that may negatively impact their satisfaction scores (Otani, et.al). Through the management of depression and pain including setting up an appropriate preoperative expectation, physicians are able to attain good outcomes. This training is therefore developed for all the medical employees and the RN within the Houston Methodist St. John Medical facility including support staff members in the facility. The number of patients and employees to be trained amounts to one hundred
Training Needs Analysis
The training and development of the medical practitioners and other support staff members within this medical facility is pivotal to the overall vision of the medical fraternities aimed at improving patient satisfaction through an improved quality of the care of patients. In order to achieve this, it is essential that the learning and development resources are appropriately aimed at ensuring the efficiency of training programs (Otani, et.al). The management fraternity of the Houston Methodist St. John Hospital is committed to ensuring that it’s skilled workforce is motivated by providing quality services aimed at improving the satisfaction of patients.
The hospital is therefore articulating approaches of training all the relevant staff members on the provision of better care. Through the training needs analysis (TNA), an outline is provided that ensures appropriate, and relevant training needs to the staff groups are comprehensively covered. The TNA, therefore, focuses on the specific training requirements that are mandatory in meeting the institution’s needs.
Houston Methodist St. John Hospital is a comprehensive surgical and medical hospital with 121 beds. The hospital according to sources records visits that amount to 24,940 patients in the emergency room. The total admissions of the hospital also amount to 6, 628 with its physicians performing 2,062 inpatients, and 2995 outpatient surgeries. The hospital specializes in the treatment of Cancer, heart and vascular diseases, gastroenterology, and GI surgeries, neurological and neurosurgeries, orthopedic and sports medicine, transplants among other services.
With these facts, it is significant to notice that the hospital attends to a broad range of individuals who have varied health needs and require special care that satisfies their needs. The staff members in this facility, therefore, have the responsibility to maintain professional standards through a fulfilled training initiative (Otani, et.al). The training needs analysis TNA will, therefore, ensure that compliance is monitored carefully, and the results of the training are noticeable in practice. Find the training needs analysis attached on the appendix.
Summary of the Research Results
After carrying out a research on the need for training in order to address the low levels of patient satisfaction; it has been determined that there are certain factors such as noise levels and the doctors’ bedside manner. In addition, whether patients are in position to recommend the hospital to friends or family is also part of the areas that need to be observed in order to improve patient satisfaction.
These factors, therefore, hold a key in the future of the hospital (Otani, Chumbler, Judy, Herrmann, & Kurz, 2015). The research determined that patient satisfaction remains the main key to a new marketing tool for many hospitals, considering the fact that many patients are now involved in choosing hospitals. It is, therefore, significant to note that the findings of the study determined the fact that patients liking of the doctors has much to do with their getting better.
A patient’s expectation when they visit a medical facility is in receiving good services. It has come to realization that these expectations are determined by the gender, age, nature of illness, and the attitudes towards the circumstances of a patient. Patients also expect doctors to keep time, communicate in a simple language that is understandable, and behave cordially (Otani, et. al). They also expect care, courtesy, concern and in addition to this, professionalism. In summary, the study revealed that patient satisfaction is the key driver of patient outcomes and plays an important aspect of the pay-for –performance metrics. This therefore translates to the fact that an improved patient-physician communication has the capacity to improve patient satisfaction.
Before the training program commenced, it was discovered that the trainees had an idea from past experiences on how to improve patient satisfaction. However, their knowledge was not applicable in the context of Houston Methodist St. John Hospital since the approaches they had in mind were used in different medical organizations. This, therefore, called for the need to derive a contextualized approach that is particularly formulated to meet the needs of this medical facility (Otani, et. al). The trainees were therefore expected to prepare for the training through availing themselves and making sure that they complete the process. The trainees are also expected to incorporate the learned ideas in their practice in order to promote patient satisfaction in the health facility.
Training Objectives for the Training Program
Table 1.1
OBJECTIVE
OUTCOME
Patient Satisfaction/Quality Outcomes
1. Reduction of medical errors.
2. Eliminated instances of bad communication.
3. Increased relationship with patients.
4. Elimination of wrong surgeries.
5. Patients are well cared for in the facility.
Team Work and Communication
1. An Improved employee satisfaction score.
2. An Improved patient satisfaction score.
3. An Improved physician satisfaction score.
4. Deceased staff turnovers.
5. Increased patient turnover.
Efficiency
1. Improved provision of quality health services.
2. Improved response time to patients.
3. Increased attendance to patients with pain and depression.
Reliability
1. Decreased levels of medical errors.
2. Compliance with the Medical regulations in caring for patients
3. Increased staff-patient relationship.
Specific Training Objectives
The specific training objectives include;
Improving the patient-physician communication
Developing personal relationships with patients through showing care and compassion.
Improving the quality of services.
Training Program
In order to develop the competencies among the trainees, it is significant that time is clearly factored in order to allow the exploration of the subject in depth and detail. Through this, the trainees are able to acquire more details and get opportunities to demonstrate their newly acquired skills through practice (Otani, et. al). The training program will, therefore, take a period of 4 days spread over a period of one year in order instill the developed learning needs.
The training will be organized on an annual basis as a result of the costs associated in developing such programs. The facilitators of the training will be external instructors who have the knowledge on the subject. The trainings will be carried out within the organizations facilities and the learners will be motivated to learn through an approach aimed at waiving the training costs and fees.
The learners who show absolute commitment to the training will also be awarded (Otani, et. al). The intended audiences for the training include medical personnel’s from other health organization. The registered nurses and other medical employees within Houston Methodist St. John Hospital will be among the audience attending the training.
Table 1.2
DAY
TIME
TOPIC
TRAINING METHOD
COMPETENCY
Day 1
0800-0900 am
Introduction to the Training Program.
08.00-09.00 09.00-
11.00 11.00-12.00
12.00-13.00 13.00-
14.00 14.00-15.00
15.00-16.00 16.00-
17.00
What is Patient Satisfaction
The Results of Unsatisfied Patients.
Causes of Unsatisfaction in a health facility
LUNCH
Global priorities in reduced patient satisfaction research
Understanding the need for improving patient satisfaction.
Lecture
Lecture
Small Group discussion
Lecture
Hands on practice
1.1
1.2
1.3
1.3
2.1
Day 2
0800-0900 am
Understanding the causes of decreased patient satisfaction
Lecture
1.6
08.00-09.00 09.00-
11.00 11.00-12.00
12.00-13.00
13.00-
13;00-14;00
14.00 14.00-15.00
15.00-16.00 16.00-
Understanding the things that affect patients; The system approach
Understanding the things that affect patients; Human factors
Understanding the things that affect patients; Organizational Level
LUNCH
Research Findings on the things that affect patients and impact their satisfaction
Review of the Discussions of the Day
Discussions among Groups
Lecture
Lecture
Lecture & Discussion
Lecture and Small Group Discussion
Group Discussion
1.6
1.6
1,6
1,6
1.7
Day 3
0800-0900 am
Case analysis of a Hospital
Hands on Practice
1.6
08.00-09.00 09.00-
11.00 11.00-12.00
12.00-13.00 13.00-
13;00-14;00
14.00 14.00-15.00
15.00-16.00 16.00-
Research methods on measuring the success levels of a health institution.
Research findings on measuring the success levels of a health institution. Qualitative approach, Interviews.
Approaches of improving patient satisfaction in Medical Organization
LUNCH
Improving patient satisfaction in Medical facilities
Patient roles in ensuring they are satisfied with the provision of health services
Lecture
Lecture
Lecture
Lecture
Lecture
1.6
1.6
1.6
1.6
1.6
Day 4
0800-0900 am
Group Presentations of Research plan
Group Presentation
08.00-09.00 09.00-
11.00 11.00-12.00
12.00-13.00 13.00-
13;00-14;00
14.00 14.00-15.00
Organizational Changes that can be employed to solve the problem
Implementing Change in an institutional level
LUNCH
Using evidences to demonstrate patient
Implementing Change on a individual level
Group work
Lecture
Lecture
Lecture
3.5
3.5
3.5
3.4
Conclusion
Patient satisfaction remains a significant and commonly used indicator that many medical facilities incorporate in measuring the quality of health care services they offer to patients. A patient’s expectation when they visit a medical facility is in receiving good services. It has come to realization that these expectations are determined by the gender, age, nature of illness, and the attitudes towards the circumstances of a patient.
Patients also expect doctors to keep time, communicate in a simple language that is understandable and behave cordially. It is imperative to realize that patient satisfaction has the capacity to affect the retention of patients, medical malpractice complaints, and clinical outcomes (Otani, et. al). It is essential to note that this training program is a vital element for Houston Methodist St. John Hospital. Patient-physician communication has been a challenge, and if improved, a tremendous opportunity for improvement is likely to be noticed.
The essence of the program is on improving patient-physician communication. The essence of the training program is on improving patient-physician communication. It has been discovered that patient-physician communication is a primary contributor to reduced patient satisfaction. After training, it is anticipated that the levels of patient satisfaction will increase, a factor that will impact an organizations delivery of services in the community. Through the training, the trainees learned variable approaches of improving communication and also increasing the delivery of services to patients aimed at improving the satisfaction levels of patients.
References
Hall, D., Shirey, M. A., & Waggoner, D. C. (2013). Improving Access and Satisfaction with Spiritual Care in the Hospice Setting. Omega: Journal Of Death & Dying, 67(1/2), 97-107.
Otani, K., Herrmann, P. A., & Kurz, R. S. (2011). Improving patient satisfaction in hospital care settings. Health Services Management Research, 24(4), 163-169. https://www.doi:10.1258/hsmr.2011.011008
Otani, K., Ye, S., Chumbler, N. R., Judy, Z., Herrmann, P. A., & Kurz, R. S. (2015). The Impact of Self-Rated Health Status on Patient Satisfaction Integration Process. Journal Of Healthcare Management, 60(3), 205-218.
Appendix
TRAINING NEEDS ANALYSIS (TNA) FOR HOUSTON METHODIST ST. JOHN HOSPITAL.
EMPLOYEE NAME:
POSITION
TNA DONE BY:
Major tasks of position
Training/skills development required?
If yes, identify what training needs exist
How will this be achieved?
(eg on the job, external training)
When?
Who to organise?
Training provider?
Y
N
<insert major tasks of position>
ü
<insert training needs, if any>
<insert how this will be achieved>
<insert when>
<insert who is going to deliver the training>
eg on the job, external training
What do we want to achieve in the period ahead?
<insert comments>
How will the trainees attitudes change towards the new information provided during training?
<insert comments>
How are we going to make this happen?
<insert comments>
What will you need from the Medical Institution to help you to reach your career goals?
<insert comments>
We can write this or a similar paper for you! Simply fill the order form!
As pediatric patients grow from infancy to adolescence, there are many common body system disorders that may potentially present. As an advanced practice nurse caring for these patients, you must understand the pathophysiology and epidemiology of these disorders as this will help you to recognize symptoms and select appropriate assessment and treatment options. In this Assignment, you prepare for your role in clinical settings as you design a protocol for the diagnosis, management, and follow-up care for a common body system disorder.
To prepare:
•Reflect on “Lyme disease”.
•Think about the pathophysiology and epidemiology of the disorder.
•Consider a protocol for the diagnosis, management, and follow-up care of the disorder you selected.
•Think about how culture might impact the care of patients who present with this disorder.
To complete:
Write a 2- to 3-page paper that addresses the following:
•Explain the disorder Lyme disease, include its pathophysiology and epidemiology.
•Explain a protocol for the diagnosis, management, and follow-up care of this disorder.
•Explain how culture might impact the care of patients who present with the disorder you selected.
The School of Nursing requires that all papers submitted include a title page, introduction, summary, and references. The Sample Paper provided at the Walden Writing Center provides an example of those required elements (available at http://writingcenter.waldenu.edu/57.htm). All papers submitted must use this formatting.
SAMPLE ANSWER
Lyme Disease
Introduction
Many different kinds of body infections exist hence, is prudent for advanced practice nurses to understand (APN) them to provide better diagnosis, management, and even follow up. Lyme disease is one of such body system disorders that APN need to know to manage the same well. The author therefore, deliberates on Lyme disease, its epidemiology and pathophysiology, explains protocol from diagnosis, management, and follow-up, and explains how culture might affect the care of patients suffering from this disease.
Lyme disease
Despite the fact that the prevalence of Lyme disease is becoming prevalent in communities, many APN as well as physicians are still unfamiliar with it. Lyme disease known by another name as Lyme borreliosis is among the common vector borne diseases (Pearson, 2014). The disease is infectious as a bacterium known as Borrelia burgdorferi belonging to the spirochaetes causes it. The disease is usually transmitted through the bite of an infected tick.
Pathophysiology
The moment an infected tick bites a human being, B. burgdorferi is left in the skin and henceforth begins to spread. Signs and symptoms of the disease manifest due to the immune response to the spirochete in the tissues of the body (Beard, Nelson, Mead, Petersen, & Raoult, 2012). During the bite, the saliva of the tick is released together with spirochete as the tick feeds and this disrupts the immune response at the site where the bite occurred (Glatz, Resinger, Semmelweis, Ambros-rudolph, & Müllegger, 2015). Therefore, such a point is conducive to spirochete to establish an infection which grows and multiplies on the surface of the skin (dermis). The inflammatory response of the host leads to the formation of a circular EM lesion (Halperin, 2014). Because Neutrophils fails to appear to destroy spirochetes, the EM lesion develops and spread on the entire body. Few days after the bite, the spirochetes spread through blood stream to other parts of the body such as heart, joint, distant skin sites and nervous systems. In case, the bacteria is not treated immediately, it may persist in the body for months or even years, regardless of the production of B. burgdorferi.
Epidemiology
The disease is prevalence in the northern hemisphere and more incidences have been on increase across the world. Reasons for this are changes in biodiversity, climate change, land management, human interactions with nature and increasing awareness about the disease. Laboratory findings in UK found that Lyme cases have increased nearing to 1200 in a year even though true incidence is not known because of many cases that go unreported (Pearson, 2014). Incidences of Lyme disease are higher in Southern England, including, Scottish highland, and London. Level of public and health care professionals’ awareness about the disease in UK is still lacking. The disease has as well been reported in various countries across Africa, Europe, north and South America and Asia. Highest cases are among people aged between 45-65 years followed by those in age bracket 24-44 years (Pearson, 2014).
Diagnosis, management, and follow-up care
Lyme disease has treatment, and the journey begins from diagnosis. Those eligible for diagnosis are those with the history of tick bite, other signs, and symptoms of Lyme disease and erythema migrans (Pearson, 2014). Diagnosis should be clinically based and should be based on careful history taking, examination and getting information from carers, and ensuring careful interpretation of results. Other tests can as well be undertaken as part of the diagnosis to ascertain the infections. Treatment should then start immediately after diagnosis. Even though a range of antibiotics is available, the choice of the best is under debate as some have side effects. Some of the antibiotics recommended include amoxicillin, and doxycycline administered in different dosages depending on the age of the patient (Pearson, 2014). Patients require close monitoring to ensure they take the right medication, dosage until they recover.
Culture Aspect in Care of Patients
The culture of people differs and may have adverse effects on patients with Lyme (Aenishaenslin, Ravel, Michel, Gern, Milord, Waaub & Bélanger, 2014). Some people believe that this disease is for animals and therefore, health care providers may be adamant to take care of such patients. Therefore, the attitudes and beliefs of people, especially the carers can have a negative implication on the health care that is provided to patients. It becomes important for all public health professional and public to be sensitized about the disease for them to accord respect and assistance to Lyme patients.
Conclusion
Lyme disease like any other body disease needs proper management and treatment. The disease is spreading across the world because of increased sensitization. Cultural factors can halt efforts to manage the disease and is appropriate for all relevant authorities to step up their awareness campaigns to sensitive more health providers and public for better management of this disease.
References
Aenishaenslin, C., Ravel, A., Michel, P., Gern, L., Milord, F., Waaub, J., & Bélanger, D. (2014). From Lyme disease emergence to endemicity: a cross sectional comparative study of risk perceptions in different populations. BMC Public Health, 14(1), 1070-1091. doi:10.1186/1471-2458-14-1298
Beard, C. B., Nelson, C. A., Mead, P. S., Petersen, L. R., & Raoult, D. (2012). Bartonella spp. bacteremia and rheumatic symptoms in patients from Lyme disease-endemic region. Emerging Infectious Diseases, (11), 1918.
Glatz, M., Resinger, A., Semmelweis, K., Ambros-rudolph, C. M., & Müllegger, R. R. (2015). Clinical Spectrum of Skin Manifestations of Lyme Borreliosis in 204 Children in Austria. Acta Dermato-Venereologica, 95(5), 565-571. doi:10.2340/00015555-2000
Halperin, J. J. (2014). Lyme Disease: Neurology, Neurobiology, and Behavior. Clinical Infectious Diseases, 58(9), 1267-1272.
Pearson, S. (2014). Recognising and understanding Lyme disease. Nursing Standard, 29(1), 37- 43.
We can write this or a similar paper for you! Simply fill the order form!
Providing cost effective care without limiting access
Providing cost effective care without limiting access
Order Instructions:
Providing cost effective care without limiting access
Providing cost effective care is a professional aspect of the Advance Nurse Practitioner’s role when caring for clients. Diagnostic testing can aid in therapeutic decision making, but contributes substantially to the cost of medical care. Testing is necessary in most cases, and if used improperly can cause significant cost and not lend much to diagnostic accuracy.
Write a 4 page APA formatted paper on the need to provide cost effective care without limiting access to care.
Discuss:
• Why this is an important aspect of providing care to patients
• How care can be made more affordable without limiting access to necessary care
• How to maintain cost effectiveness and still get the needed information for a diagnosis without ordering unnecessary diagnostic exams
Assignment Requirements
The finished Assignment should be a 4-page descriptive and critical/evaluative essay, excluding the title page and references. The viewpoint and purpose of this Assignment should be clearly established and sustained.
Before finalizing your work, you should:
• utilize spelling and grammar check to minimize errors; and
• review APA formatting and citation information found online, or on APA manual
Your Assignment should:
• follow the conventions of Standard American English (correct grammar, punctuation, etc.);
• be well ordered, logical, and unified, as well as original and insightful;
• display superior content, organization, style, and mechanics; and
• use APA 6th edition format for organization, style, and crediting sources including:
• properly formatted header
• 12-point, double-spaced, Times New Roman font
• use of in-text citations
• title page and reference page
• use of headings (if applicable)
Resources
Choosing Wisely: Knowing the Costs of Health Care (Dana Frank, MD)
Choosing Wisely: The Impact of Rising Costs on Health Care (Joe Marine, MD)
Choosing Wisely: The Need to Simplify Health Care (Ann Morrill, MD)
Providing Cost Effective Care without Limiting Access
Introduction
Providing affordable care is a professional characteristic of (APN) Advanced Nurse Practitioner’s responsibility when taking care of clients. Diagnostic procedures in most of the time assist in making therapeutic decision-making. However, these procedures can contribute substantially to the expenditure of medical attention. Testing is crucial in medication, but if used improperly, it can bring considerable expenditure and not lend much for diagnostic accuracy. Therefore, the following discussion will indulge in discussing the importance of enhancing care that is cost-effective without restraining access. In addition, paper will discuss how care can be made more affordable. The paper concludes by suggesting ways on how to maintain cost effectiveness in the provision of cost-effective care without ordering unnecessary diagnostic exams.
Discussion
Providing care that is cost-effective without restraining access has a number of considerable benefits. Considering that the cost of health care services in the U.S. is increasing every year, government and other health stakeholders are looking for ways on how to health care affordable. One importance noticed by Greene (2015) is that cost-effective care will automatically relieve the heavy burden carried by health providers. For instance, health organizations can fight turnover costs of their nurses. This is because saved costs are usually used in motivating and retaining nurses. Persad (2015) argues that this will save the health organization the costs of advertising, and the overall costs employed to market nursing positions in the effort to recruit and employ nurses to take the turnover vacancies. This importance leads to another importance of increased productivity, which is one of the main agendas for the existence of a health organization as a business. Another importance regarding providing cost-effective care without limiting access is an improvement in providing quality healthcare. This is because cost effective care ensures that there is enough money saved to revolutionize medication administration, communication improvement, facilitate intensified and extensive follow-up, as well as client engagement (Greene, 2015). Considerably, affordable care without limited access facilitates coordination of patient care to decrease unneeded assessment and processes. Besides, a health facility can work effectively with other health providers such as case managers to ensure that there is safe and well-timed hospital discharge. Finally, transparency is witnessed when there is cost effective care (Persad, 2015). When cost effective care is put on the ground, nurses and medical practitioners do not find it necessary to direct a client to unnecessary diagnosis or procedures. Rather, the practitioners inform the patients all matters in black and white and involve other professionals in it.
Health care expenditures remain a key challenge to most Americans in accessing quality health care in the U.S. Greene (2015) argues that although such Act as the Affordable Care Act strives to make every American get affordable care, there has been limitation in accessing the health care services. One method to get affordable health care, Greene (2015), for instance, is by patients avoiding scheduling non-medically illustrated labor instructions before thirty-nine weeks. This is meant to reduce the use of unnecessary imaging assessments, for example, early utilization of MRI or CT for mild complaints that will automatically disappear on their own. Dana (2011) continued to assert that most unnecessary tests and procedures expose a patient to radiation and unwanted surgery.
Ann (2011) who added that the inaccessibility to affordable care is because of the complexity of health care echoes Dana’s argument. Ann (2011), an endocrinologist at Maryland Medical Center, argues that the only affordable care that can be made available to Americans is patient-centered care. In other words, Ann (2011) calls for an absolute simplification of the processes involved in mediation in the interest of the patients. Ann (2011) continued to assert that many patients give up in the quest for affordable health due to inconveniences of bureaucratic procedures in accessing health care. However, Joe (2011), a cardiologist at John Hopkins Bayview, appears on the realm of this discussion about affordable health care by attesting that the reason behind inaccessibility to affordable health care is the continued rising costs of health care. Greene (2015) echoes this statement by arguing that patients have to be assisted financially to access health care.
Another alternative to making care affordable is by empowering non-physician providers. This empowerment will ensure that non-physicians such as advanced-practice nurses practice entirety of their training (Persad, 2015). Progressively, these providers will expand the workforce, which will necessarily lower prices to make health care affordable. Making medical insurance cover cheaper will also aim at making health care affordable. Health insurance exchange plans are reasons behind unaffordable health care (Greene, 2015). These costs make makes it hard to make health care affordable.
By fostering efficient communication between health care providers and patients, cost effectiveness can be maintained, and make doctors acquire the required data for a diagnosis without ordering pointless diagnostic assessments. Contributing in the Choosing Wisely, Ann (2011) argued that poor communication between the two parties hinders accessibility for affordable health care. When there is coherent communication between providers and patient, Greene (2015), there is a better discussion about tests and procedures, and the patient will be able to make the decision about his or her condition. For instance, when a man is suffering from prostate cancer is fed with information regarding the treatment of the disease he might not seek medication. Persad (2015) argues that this is because the condition is unlikely to affect him before he dies due to other causes. Therefore, the patient will not go for testing and scanning, as they become unnecessary. Although health care resources are abundant, they are however utilized improperly. Dana (2011) who argued that nurse practitioners do not know the costs of health are procedures gave this statement. He also added that many billions of money is wasted each year through unnecessary services such as fraud and excessive administrative expenditures. Therefore, Persad (2015), the physician ends up recommending unnecessary diagnostic procedures. Thus, there is need to educate the physician about the cost of the health care procedure, which they will be using to reevaluate their decisions before prescribing unwanted medical procedures and tests. In addition, nurse practitioners need to be supplied with comprehensive copies of the cost of each test. According to Dana (2011), this will assist them in getting back to the list and evaluate whether it is effective to carry out a diagnostic test.
Summary
In conclusion, it can be deducted from the above discussion that nurse practitioners can unintentionally result in unnecessary medical testing and procedure. This leads to misuse of resources leading to cost-ineffectiveness. However, this can be averted if there is established good communication between providers and patients to reduce the numbers of unnecessary procedures and tests. Altogether, affordable care will be made available to the patients if medical insurance premiums are made affordable and the workforce of nurse practitioners expanded.
References
Ann, M. (18 Aug, 2011). Choosing Wisely. The Need to Simplify Health Care. [You Tube]. Retrieved on 10 July, 2015 from:
Greene, S. (2015). A survey of emergency medicine residents’ perceptive of the choosing wisely campaign. American journal of Emergency Medicine, (6), 853.doi:10.1016/j.ajem.2015.03.067
Joe, M. (18 Aug, 2011). Choosing Wisely: The Impact of Rising Costs on Health Care. [You Tube]. Retrieved on 10 July, 2015 from:
Persad G. (2015). The Medical Cost Pandemic: Why Limiting Access to Cost-Effective Treatment Hurts the Global Poor. Chicago Journal of International Law, 15559.
We can write this or a similar paper for you! Simply fill the order form!
Community Needs Assessment: Prince George’s County
Order Instructions:
W2 Clinical Assignment: Assess the Needs of the Community
Community & Public Health Nursing
Assess the Needs of the Community
Data Gathering: Data can come from a variety of sources and can include the following:
• Demographics of the community
• Vital statistics
• Previously conducted surveys
• Information from state and local health departments
The paper will use prince Georges County in Maryland as its community in question.
SAMPLE ANSWER
Community Needs Assessment: Prince George’s County
Needs assessment is a vital practice in communities as it allows stakeholders to identify gaps and work toward their closure. It is through needs assessment that parties identify problems and seek measures of addressing them. The utilization of the results that need assessment studies reveal could facilitate developments in communities. The process is usually systematic, and it is the desire to improve living conditions and other aspects of life that motivates the personnel that conducts the assessments. In most communities, needs could be relative, perceived, or expressed.
Prince George’s County has people of varied origin, and Hispanics and African-Americans constitute the majority. 98% of the county’s population was residing in the urban in the year 2012, and only 2% of the total population dwelled in rural areas (Onboard Informatics, 2015). Males constitute 44% of the population while females make up the remaining 56%. According to studies, the mean weight of men in the county is 198 pounds while that of females is 172 pounds (Onboard Informatics, 2015). The population recorded a score of 3.6 on general health, and, therefore, the county hits the average mark. The studies indicated that more than 70% of the residents engage in frequent physical activities (Onboard Informatics, 2015). The studies also showed that less than half of the population smoked cigarettes, and almost a three-quarter of the adults took alcohol (Onboard Informatics, 2015).
There are varied forms of needs in Prince Georges. Public health is among the areas where the residents of Prince George’s express needs. For instance, the community requires an enhancement of health care accessibility. Raised cost of services hinders a significant population from accessing medical care. Measures such as making prescription medications cheaper could promote the accessibility of health care. There is also a considerably uninsured population in the county, and extending cover to such persons could promote care accessibility. Focusing on the needs of the elderly could also offer an efficient measure toward the enhancement of care accessibility. The county has a considerably large population that is beyond sixty-five years, and supporting them could have a substantial impact on the community’s public health sector.
There is also a need for stakeholders to offer intensive education to the residents of the region. For instance, stakeholders could make the population aware of health hazards that could present in their area. There is a need to inform the residents of the appropriate livelihood to adopt so as to avoid diseases. From the demographics, an appreciable percentage undertakes physical activities, and educators could encourage more residents to pursue the approach (Onboard Informatics, 2015). The population also needs education on chronic ailments. It could be necessary to warn the residents of Prince Georges against practices that could predispose them to terminal illnesses.
There is a need to reduce alcohol consumption among residents of Prince Georges. About 80% of the adult population is alcoholic, yet the practice comes with adverse effects on the health of the alcohol users (Onboard Informatics, 2015). The community should understand the conditions associated with alcohol use.
The community also constitutes of people of varied origins, and there could be a possibility of discrimination in care access on the basis of people’s origin. Therefore, there is a need for leaders and health care practitioners to ensure that they offer services beyond racial considerations. Stakeholders should ensure that community members access standard care without racial barriers.
W1 Clinical Assignment:
Define the Community at Risk
During your practicum you will use the follow guidelines to complete your final project and a community teaching project and paper.
Identify the target population Definition of the risk or problem and the significance ( e.g. teenage pregnancy, HIV, obesity).
The target population for this community teaching project will be all sexually active members of the community. This means that the married, divorced, separated and single adults as well as adolescents and commercial sex workers will be involved in this project. HIV knows not age, class, race, ethnicity, religion or even profession. It has the capability of infecting any sexually active individual who engages in irresponsible sexual behaviour with multiple partners. Information and awareness creation on HIV is therefore very essential for the young, the middle-aged and old members of the community (Crawford, Caldwell, Bush, Browning & Thornton, 2012).This population has been chosen because it is at the highest risk of being infected with HIV. The population will therefore be empowered with important information regarding HIV with the aim of reducing and eventually stopping new infections, caring for and treatment of those already living with the disease.
Definition of the problem
HIV has been a problem that has given medical researchers sleepless nights for so many years. It is indeed a great challenge for members of different communities given that up to date, there is no known cure for it. Everybody is at risk of HIV infection given that it is very difficult to tell whether one is infected or not unless a medical test is conducted. As for young people particular those going through there adolescence, the risk of infection is even greater because they lack adequate information on reproductive health and they are also likely to involve themselves in risky sexual behaviour due their strong peer influence. Adults who are married are not safe from HIV either. This is because a good number of married couples have been found to engage in extra marital affairs which have actually predisposed them to the risk of HIV infection. This means that HIV is silently spreading in marriages which were initially thought to be relatively safe. Infants have also not been left out due to the risk of mother to child transmission. Infection with HIV is not a barrier for women to get pregnant and therefore it would be important to educate expectant mother whether living with HIV or not on how they can protect their new born babies from acquiring this deadly virus (Sepúlveda, 2012). Another very common problem that relates to HIV in the community is stigmatisation of those who are living with the virus. Many HIV positive individuals have reportedly been living in fear or even hiding from other members of the society. This is a very serious problem that has also prevented them from accessing their medication which has led to further deterioration of their health.
Significance
This project will play a very crucial role not only to members of the community but also to the public health and nursing profession. Members of the community will be able to learn a lot pertaining to HIV and with such kind of information, new infections will have a significant decline if not a complete halt. This is because some new infections usually occur as a result of ignorance and the moment awareness is created among community members, such cases will definitely decrease. The project will also enable community members to learn about home-based care of people living with HIV since it is a chronic disease. It would also be important for people to be informed about the signs and symptoms of HIV so that they can seek early medical attention before the virus advances in their bodies. Most importantly, the project will be encouraging people to go for frequent voluntary counselling and testing for HIV so that can get to know their status and take appropriate action. Those who test positive for the virus will of course be counselled and prepared to start antiretroviral therapy where as those who test negative will be enlightened on how they can continue protecting themselves against the virus (Kuznetsov, Matterne, Crispin & Ruzicka, 2013).
References
Crawford, T., Caldwell, G., Bush, H. M., Browning, S., & Thornton, A. (2012), Foreign born status and HIV/AIDS: A comparative analysis of HIV/AIDS characteristics among foreign and U.S. born individuals. Journal of Immigrant and Minority Health, 14(1), 82-8. doi:http://dx.doi.org/10.1007/s10903-011-9455-8
Kuznetsov, L., Matterne, U., Crispin, A., Ruzicka, T., Zippel, S. A., & Kuznetsov, A. V. (2013), Knowledge, attitude and behavioral intention to act regarding HIV infection and prevention in immigrants from the former soviet union in Germany: A comparative study with the native population. Journal of Immigrant and Minority Health, 15(1), 68-77. doi:http://dx.doi.org/10.1007/s10903-012-9671-x
Chronic Venous insufficiency (CVI) vs. Deep Vein thrombosis (DVT)
Chronic Venous insufficiency (CVI) vs. Deep Vein thrombosis (DVT)
Order Instructions:
Advanced practice nurses often treat patients with vein and artery disorders such as chronic venous insufficiency (CVI) and deep venous thrombosis (DVT). While the symptoms of both disorders are noticeable, these symptoms are sometimes mistaken for signs of other conditions, making the disorders difficult to diagnose. Nurses must examine all symptoms and rule out other potential disorders before diagnosing and prescribing treatment for patients. In this Assignment, you explore the epidemiology, pathophysiology, and clinical presentation of CVI and DVT.
To prepare:
•Review the section “Diseases of the Veins” (pp. 585–587) in Chapter 23 of the Huether and McCance text. Identify the pathophysiology of chronic venous insufficiency and deep venous thrombosis. Consider the similarities and differences between these disorders.
•Select a patient factor different from the one you selected in this week’s Discussion: genetics, gender, ethnicity, age, or behavior. Think about how the factor you selected might impact the pathophysiology of CVI and DVT. Reflect on how you would diagnose and prescribe treatment of these disorders for a patient based on the factor you selected.
•Review the “Mind Maps—Dementia, Endocarditis, and Gastro-oesophageal Reflux Disease (GERD)” media in the Week 2 Learning Resources. Use the examples in the media as a guide to construct two mind maps—one for chronic venous insufficiency and one for venous thrombosis. Consider the epidemiology and clinical presentation of both chronic venous insufficiency and deep venous thrombosis.
To complete:
Write a 2- to 3-page paper that addresses the following:
•Compare the pathophysiology of chronic venous insufficiency and deep venous thrombosis. Describe how venous thrombosis is different from arterial thrombosis.
•Explain how the patient factor you selected might impact the pathophysiology of CVI and DVT. Describe how you would diagnose and prescribe treatment of these disorders for a patient based on the factor you selected.
•Construct two mind maps—one for chronic venous insufficiency and one for deep venous thrombosis. Include the epidemiology, pathophysiology, and clinical presentation, as well as the diagnosis and treatment you explained in your paper.
This Assignment is due by Day 7.
Please use the writer who did my last mine map if possible. Thank you.
SAMPLE ANSWER
Chronic Venous insufficiency (CVI) vs. Deep Vein thrombosis (DVT)
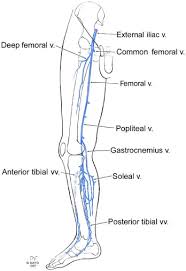
Chronic Venous insufficiency occurs when the valves in the venous system malfunction. This is facilitated by various incidences such as age, smoking, and increased physical inactiveness. When the valves are damaged, they cause the blood to flow back. This forms blood clot in the vein found along the hind limb, causing a disease condition known as Deep Vein Thrombosis (DVT). The clinical manifestation of the disease includes swelling of the ankle if the patient stands of sits for a long period. The swelling is sometimes painful and causes flaking of the skin and itchiness (Davies, Lumsden, & Vykoukal, 2011). Deep Vein Thrombosis (DVT) is a cardiovascular complication that results when the venous valves located at the hind limb becomes damaged. The venous system transports deoxygenated blood from the rest of the body to the heart for oxygenation. During this cycle, blood flows upwards from legs to the heart. For this to occur, the muscles of the feet and the calf contract, squeezing the veins which then propel blood upward towards the heart. The vein has valves are aligned in one direction and facilitate blood transportation. Consequently, blood circulation is disturbed, making it difficult for blood to circulate effectively and blood pools in these veins (Kibbe, Pearce, & Yao, 2010).
CVI and DVT compare in that the diagnostic process is similar and includes use of duplex ultrasound technology to check the blood circulation process. The technique applied is as follows, the transducer part of the machine is normally placed on the site that s directly above the vein in question, the waves on how the blood is flowing together with a 3D formulation of the vein anatomical structure is displayed on the monitor. This diagnosis is important because it is able to diagnose early enough, and the disease gets treated using the appropriate medication. The pharmacological medication is often coupled with on pharmacological medication, such as weight loss, exercises, and the reduction of environmental stressors such as standing for a long period. Other measures include compression stockings and taking antibiotic (Huether, & McCance, 2012).
Evidence based research indicates that the CVI and DVT prevalence illustrate healthcare disparity. This is mainly due to the interactions of healthcare determinants such as genetic, environmental factors, ethnic background, and socioeconomic status. The prevalence rate is high among the African American, Hispanics, and Caucasians as compared to White. Literature associates these findings with environmental exposures and socio economic background. For instance, the white population has high rates of educated people and low rates of low household income (Kibbe, Pearce, & Yao, 2010). This implies that they are able to access the hospital routinely and are treated early before the disease clinical manifestations become worse. On the other hand, these other communities have the highest number of dropouts. The children are more susceptible to drugs and poor living condition at a tender age. Additionally, the high hospital cost act as an obstacle to accessing quality care. Therefore, these people will really on alternative therapies and over counter drugs for a long period, and will only access care during the last stage of the disease. These communities have the highest rates of obesity, which is a main risk factor to DVT and CVI (Murphy & Lloyd, 2013).
References
Davies, M., Lumsden, A., & Vykoukal, D. (2011). Chronic venous insufficiency. Minneapolis: Cardiotext Pub.
Huether, S. E., & McCance, K. L. (2012). Understanding pathophysiology (Laureate custom ed.). St. Louis
Kibbe, M., Pearce, W., & Yao, J. (2010). Venous disorders. Shelton, Conn.: People’s Medical Pub. House—USA.
A Healthcare Article Summary and Discussion Order Instructions: The writer will have to pay attention to all instructions hear as they have proving not to read instructions before attempting these papers.
A Healthcare Article Summary and Discussion
The writer must read all the instructions and carefully respond to all the questions as per the instructions. The writer must properly format the paper in APA 6th edition and must use proper grammar and spellings.
Topic: Healthcare Article Summary and Discussion
1. Review the articles below.
2. Select an article and post a summary to include the following:
a. Name of policy selected and purpose of development.
b. Policy influence on healthcare practice including ethical and legal considerations.
c. Role of APN in influencing change in policies affecting NP practice in your state of choice (Washington DC).
Articles
Journals:
Park, M. (2009). The legal basis of nursing ethics education. Journal of Nursing Law. 13, 107–113.
Burgess, J., Purkis, M. (2010). The power and politics of collaboration in nurse practitioner role development.
Nursing Inquiry. 17. 297–308.
Macinko, J., Silver, D. (2012) Improving state health policy assessment: an agenda for measurement and analysis. American Journal of Public Health. 9. 1697–1705.
Johnstone, M., Kanitsaki, O. (2010). The neglect of racism as an ethical issue in health care. J Immigrant Minority Health. 12. 489–495.
Allen, N., Jackson, H. (2011) What kind of evidence do we need for evidence-based mental health policy? The case of the better access initiative. Australian and New Zealand Journal of Psychiatry. 45. 696–699.
Golden, T, Bryere, S., Karpur, A., Nazarov, Z., VanLooy, S. (2012). Workforce development policy: Unrealized potential for Americans with disabilities. Rehabilitation Education. 26. 5–18.
Poghosyan, L., Lucero, R., Rauch, L., Berkowitz, B. (2012). Nurse practitioner workforce: A substantial supply of primary care providers. Nursing Economic$. 30. 259–294.
Blum, J. (2010). The quagmire of hospital governance – finding the mission in a revised licensure model.Journal of Legal Medicine. 31. 35–57.
Mallarou, M., Paul, S. (2009). Legislative issues in the processing of sensitive personal data in the electronic patient record. Health Science Journal. (3). 139–148.
Green, M. (2008). How national policy affects the care of patients who suffer a heart attack. British Journal of Nursing. (21). 1199–1203.
Gaskin, D. (2012) Recent developments in health law. Accountability after Guantanamo: The Role of U.S. Health Professionals. Journal of Law, Medicine, and Ethics. Spring. 160–175.
Fouka, G., Mantzorou, M. (2011). What are the major ethical issues in conducting research? Is there a conflict between the research ethics and the nature of nursing? Health Science Journal. (5). 3–14.
Mistry, K. (2012). A new framework for childhood health promotion: The role of policies and programs in building capacity and foundations of early childhood health. American Journal of Public Health. (102). 1688–1696.
Giovanni, L. (2012). End-of-life care in the United States: Current reality and future promise – A policy review. Nursing Economic$. (30). 127–135.
Lachman, V. (2012). Ethical challenges in the era of health care reform. Medsburg Nursing. (21). 248-251.
Benatar, S., Gill, S., Bakker, I. (2011). Global health and the global economic crisis. American Journal of Public Health. 646-653.
A Healthcare Article Summary and Discussion Web Resources
• Nursing World. Code of Ethics for Nurses and the Interpretive Statements. Retrieved from http://www.nursingworld.org/MainMenuCategories/EthicsStandards/CodeofEthicsforNurses/Code-of-Ethics.pdf
• National League for Nursing. Retrieved from http://www.nln.org
• National Organization of Nurse Practitioner Faculties. Retrieved from http://www.nonpf.com
• American College of Nurse Practitioners. Retrieved from http://www.acnpweb.org
• American Academy of Nurse Practitioners. Retrieved from http://www.aanp.org
A Healthcare Article Summary and Discussion Sample Answer
A Healthcare Article Discussion
Policies are essential aspects of nursing practice. They promote coordination in the provision of care, and their absence could lead to insufficiencies of services offered. Health management should not only comply with state laws, but they should also adhere to federal regulations as outlined in varied policies (Blum, 2010, Pg. 37). Also, health organizations require having policies that enable them to guard the confidentiality, integrity as well as accessibility of information (Malliarou & Sarafis, 2010, Pg. 144).
A Healthcare Article Summary and Discussion and A Summary of Lachmann’s Article
Lachmann evaluated the Affordable Care Act in terms of its effect on healthcare reforms and promotions (Lachmann, 2012, Pg. 248). The article highlights aspects of ACA that shape, and direct provision of nursing care. The purpose of developing ACA was to make insurance coverage available to as many citizens as possible (Lachmann, 2012, Pg. 248). The plan is among the established policies through which the government seeks to facilitate healthcare provision. ACA has varied aspects that enable it to have remarkable achievements within the healthcare setup. Aspects making ACA successful include its coverage of young adults and pre-existing illnesses. Also, ACA enhances the affordability of insurance exchange plans and has elements that focus it to consumers (Lachmann, 2012, Pg. 248). To achieve cost-effectiveness, ACA limits both lifetimes as well as the annual amount of money that it places in terms of benefits (Lachmann, 2012, Pg. 248). According to the Act, insurers need reviewing their terms of coverage and justify their plans in terms of cost. ACA also purposes to ensure that consumers stand better positions in controlling their health than insurers. To ensure that consumers are at their best position, ACA grants preventive care, choice of doctors, and eligibility to people aged beyond 65 years (Lachmann, 2012, Pg. 248).
Influence of ACA on Healthcare and A Healthcare Article Summary and Discussion
ACA promotes ethics associated with beneficence as well as maleficence through its enhancement of affordability of insurance and its orientation to consumers (Lachmann, 2012, Pg. 249). Morally, all people should enjoy health coverage, and it would be unfair to have some populations denied the right owing to their financial limitations. When people access insurance coverage, they feel more important and realize full functionality in their communities (Lachmann, 2012, Pg. 249). However, ACA also faces both legal and ethical criticism. For instance, the Act forces people to buy the service. In so being, ACA overlooks people’s right to purchase just what they desire. ACA also embraces the use of Electronic Medical Records, yet the technology threatens personal privacy (Lachmann, 2012, Pg. 249).
The Role of Advanced Practice Nurses in Influencing Policies that Affect Nursing Practice in Washington DC
APN practitioners in Washington DC should lead moves toward the establishment of policies that direct nursing practice. It is their primary role to promote their society in terms of health (Lachmann, 2012, Pg. 250). The professionals should express their concerns, especially about health care policies so that residents of State of Washington enjoy high-quality healthcare services. APNs should use their organizations to push for policies that adequately address the requirements of their patients. APNs should ensure that they have sufficient directions on matters regarding nursing practice (Burgess & Purkis, 2010, Pg. 297). In most situations, nurses have a tremendous influence on healthcare setup, and would, therefore, enjoy substantial control of the system (Poghosyan, Lucero, Rauch, & Berkowitz, 2010, Pg. 1). APNs also have the role of calling for reforms on policies that may not lead to the realization of optimal outcomes for Washington DC residents.
A Healthcare Article Summary and Discussion References
Burgess, J. & M.E. Purkis. (2010). The power and politics of collaboration in nurse practitioner role development. Nursing Inquiry, 17(4), 297–308.
John D. Blum J.D. (2010) The Quagmire of Hospital Governance. Journal of Legal Medicine, 31(1), 35-57, DOI: 10.1080/01947641003598229
Lachmann, V. D. (2012). Ethical challenges in the era of health care reform. Medsurg Nursing, 12(4), 245, 248-250
Malliarou, M. & Sarafis, P. (2009). Legislative issues in the processing of sensitive personal data in the electronic patient record. Health Science Journal, 3(3), 139-149
Poghosyan, L., Lucero, R., Rauch, L., & Berkowitz, B. (2012). Nurse practitioner workforce. Nursing Economics, 30(5), 268-274.
Nursing process are standards and guidelines which are used by nurse practitioner to deliver quality care, healthcare that is patient centered. Nursing profession is a complex profession which brings aspects of art and sciences together. Nursing profession is concerned in protecting, promoting people’s overall wellbeing including physical, emotional and psychological wellbeing. The concept of nursing process is eccentric to all nurses; the process involves five steps; a) Nurse assessment; b) nursing diagnosis; c) nursing planning and identification of outcome; d) nursing implementation; e) nursing evaluation (Lee, 2010).
The first step of nursing process is assessment. This entails collection of information and data related to a certain matter or event. Nurse practitioners are required to conduct holistic care on the patient including their cultural background, their religious and social norms. This is to ensure that the interventions established are culturally and socially competent and to establish the exact care demands of a person (Svavarsdottir et al., 2014). The information gathered during the assessment phase are organized and documented, for use in the future. The second step is nursing diagnosis. This entails reviewing the information collected during the assessment more critically. This way, the actual issue of concern is identified, and prognosis is done in accordance to the clinical manifestation of disease. This is also involves identification of risk factors that motivates progression of the disease (Lu et al., 2015).
The next step is nursing planning which involves designing interventions by establishing priorities, identifying objectives that will facilitate provision of expected outcome. The planning process entails identification of interventions as established by evidence based research (RodraA-guez-Martan et al/, 2015). An effective action plan is one which is guided by Maslow’s hierarchy of needs. This involves provision of care as guided by the ladder of needs, and until all patient demands or needs are identified. Evaluation process is the last step of nursing process. It involves measuring of interventions and expected outcome to check if they are congruent with implementation plan. If the outcome is not positive, the interventions can be altered accordingly (Vaillant-Roussel et al., 2014).
Nursing Interventions Classification (NIC), direct nursing interventions include activities which directly interact with the service user. These include interventions such as administering therapy to patient suffering from dementia or Parkinson disease (Svavarsdottir et al., 2014). Indirect nursing interventions are nursing practices that aim at improving patient’s health, but the patient is not directly involved. For instance, the healthcare facility can introduce an automated system to curb medication errors. Additionally, nursing interventions can be grouped into three categories (Lee, 2010). The first category is the interdependent interventions which include activities implemented through partnership and effective communication among the healthcare staff. These include actions such as recommendation of non invasive surgery for patients suffering from renal diseases. These interventions are only carried out if all other alternative therapy has failed, and it involves lots of consultation. The dependent interventions include all nursing practices done only under instructions from the higher authority. This could be termination of service user medication due to medication error or allergic reactions to medications. Lastly, the independent intervention which entails nursing actions performed by nurses without need for permission from the higher authority; and includes all nurse practices under nurse practice (Vaillant-Roussel et al., 2014).
The importance of nursing process is that it guides registered nurse when making healthcare decisions. This is particularly important when making patient centered and culturally competent decisions. This process ensures that the registered nurses can identify the nursing issue, its etiology as well as analyze appropriate risk factors. From the information collected, registered nurse is in a position to design a patient centered plan of action, in an organized and structured process. In this framework, the expected outcomes are focused and oriented towards providing quality care. In each step, the registered nurse must document the information for effective communication and for future use. Evaluation process is important because it helps in analyzing the effectiveness of an intervention. If the action plan goals are inadequately achieve, then the healthcare providers should collaborate and work jointly to identify the underlying barriers which need to be re-evaluated and addressed (Svavarsdottir et al., 2014).
Some of the variables associated with ineffective outcomes include inaccurate assessment and data gathering processes; because some relevant information such as cultural aspects is more likely to be overlooked. In other situation, the interventions and the expected outcome could be unreasonable and somewhat unrealistic. In this case, the registered nurse is required to address the interventions and the expected outcome to ensure that they are congruent. This is done through modification of the assessment plan, diagnosis or even the implementation process. If necessary, the registered nurse can include other healthcare staff to contribute on the most effective ideologies which will bring forth successful interventions as outlined by evidence based research. This also involves thorough and adequate research which will inform the registered nurse adequately on ways and an appropriate strategy to identify the health issue, effective action plan and approaches to obtain the best conclusions (Lu et al., 2015).
Part 2: Nurse Care Plan
Assessment
Patient A resides in a residential care. The patient is 78 years old and has been experiencing mobility complications. For this reason, the patient movement is restricted and opts to use mobility supportive device i.e. wheel chair for movement. The patient is able to carry out the daily living activities such as bathing, dressing and feeding. The patient seems distressed and is often in isolation. The patient medical history is that he has suffered from Congestive Heart Failure (CHF); and has been diagnosed with associated pathologies such as hypertension, weakness in the lower extremities and hyperlipidemia. Previously, the patient was prescribed the following medication such as Atorvastatin 20mg, Lopressor 50mg, Quinapril 20mg and Furosemide 20mg.
The patient current medication includes double dosage of Quinapril and Furosemide at 40mg, Metoprolol 50mg which are administered orally, and 1.5g in 0.9% normal saline (50Ml) given three times a day. Recent regular check up, the registered nurse reported a pressure ulcer on the patient’s right side of the buttock. The ulcer coloration is red with yellow spots, and is estimated to be 10mm by 8mm; and also produces foul smell. Result from culture analysis indicates that the wound is infected by Methicillin resistant Staphylococcus aureus. The physician ordered for debridement of the black tissue, and daily dressing using antimicrobial gel (SilvaSorb).
NANDA-1 nursing diagnosis
Acute pain due to trauma on the tissue is reported; scored at 6 on 0-10 pain scale.
Risk for pressure ulcer due to tissue trauma associated with minimal movement to reduce the pressure.
Assessment data
Vital Signs: Temperature 36.70C; RR 23/Min; HRT 89 BPM; Bp 120/80.
Skin; Dry and Pale, Pupils dilated, experiences muscle cramp; Joint Movement, gastrointestinal system, urogenital systems and neurovascular system are intact.
Expected outcome
The expected outcome are Cognitive outcome- verbalize relieve pain to 2 in a 0-10 verbal pain scale and discomfort while sitting or sleeping; physiologic and affective outcome- the patient is educated on ways to prevent progression of pressure ulcer and minimize occurrence of such incidences in the future. The skin integument healing system could take a longer time frame due to the patient attributes i.e. age and chronic infection which reacts negatively to the patient immune system. In this context, the pan relief is expected to be achieved within 48hours, and healing of the wound within 5 days.
Nursing intervention
Nurse initiated: Identify the main risk factor for pressure ulcer. This includes recording of agility to monitor patient pattern of movement; and evaluate other mobility supportive devices available other than use of wheel chair. Use of alginate dressings to reduce exudates as well as lengthening the wound wears time.
Rationale: This is to establish the most effective strategy to minimize progression of pressure ulcers, and improvise ways to ensure that patient moves frequently or avoid sitting for a long period of time. This is to ensure that the patient does not remain in one position for a long time.
Interdependent intervention: protect the ulcer with silicone dressings to relieve pain, effective transition of patient to the residential facility including exchange or effective communication with the residential facility nurse to ensure that the identified nutritional and exercise strategies are adhered to.
Rationale: This is to ensure that the patient feels comfortable during the healing process. This also ensure that evidence based practice is followed; with the aim of rapid healing process and reduce the progression of disease through interdisciplinary efforts.
Dependent intervention: administration of antibiotics as reported evidence based practice. Rationale: this will help the patient self manage the ulcer pressure, as well as reduce the progression of disease. Use of hydrogel with the aim of soothing painful pressure ulcers; use of antimicrobial dressings so as to control the odor and bioburden. Clean of the peri-ulcer tissue to devitalize the dead tissue and to control the known microbial infection well known for colonization.
The patient will be educated on ways to modify behavior such as mild physical exercises and nutritional modification which will facilitate faster healing rate. For instance, the patient can be taught on approached to redistribute pressure. This includes periodic intervals turn as guided by the patient’s wish or tolerance and the type of support surface. Evidence research practice indicates that the patient should be repositioned after every two hours. The support surface can be modified using repositioning mattresses e.g. visco-elastic foam, pillows, chair cushion.
The patient should be educated on ways to maintain the skin hydrated and the nutritional supplements compatible with the patient healthcare. This includes a lot of protein supplements to facilitate faster healing rate. Additionally, the patient should be advised on ways to take care of the skin. This includes applying of emollients as indicated by the manufacturer.
Rationale: this includes nutritional modification and mild physical activeness to cure, reduce progression and prevent further formation of pressure ulcer.
Part 3: Patient teaching plan
Research indicates that the best healthcare services involve partnership between the service user and the service provider. This is because it establishes a strong bond of trust; thereby strengthening their relationship which improves quality of care. The core factor for a successful partnership is communication. Appropriate communication ensures that the patient’s demands are identified by the service provider, and they are adequately addressed. The best approach of communication is through patient education program (Vaillant-Roussel et al., 2014). This program empowers patients such that they can self manage the health complication with ease. This improves their self esteem and self image. In this context, the registered nurse is mandated to design a teaching plan that would educate the patient with ease. During the designing process, several variables must be put into consideration including the patient age, gender, ethnic background due to language barrier, education and socio economic background. This is important because the nurse can identify with the patient, and can design education material which is custom made for that particular patient. These variables also help the registered nurse in choosing the format of teaching i.e. verbal, written or audio-visual format (Jackson, 2008).
The registered nurses assess the patient specific demands from the patient medical history. Based on the findings from the assessment report, the registered nurse can apply at least three approaches namely cognitive, affective and psychomotor. The psychomotor approach is applied to patients whose educational background is low as it entails physical teaching of the interventions e.g. how to use mobility devices. The affective teaching is the most widely used approach because it is more patient centered. This approach integrates the social cultural beliefs into the clinical interventions (Kehrel, 2015).
The cognitive approach is uses cognitive functions and is mainly used to assess the memory and adaptability of a patient. This approach is commonly used in youths and individuals whose cognitive function is in good condition. Secondly, the registered nurse is required to set both short term and long term goals. People who are closely related to the patient such as care givers should be incorporated in the teaching process. Evaluation process is important because it checks if patients’ understands the concepts taught. This also facilitates to assess the patients strengths as well as weaknesses (Vaillant-Roussel et al., 2014). There are various tools for assessment including interviews, observations or use of questionnaires. These tools record data that will enhance the teaching plan of a patient. In cases where the patient fails to remember or understand the concepts, the registered nurse should revise the teaching design, and if necessary seek more information from literature and peers on the evidence based research and strategies to solve the issue, and to ensure that the patient can effectively manage their healthcare complication (Fleming, 2014).
References
Fleming, J. (2014). A Future for Adult Educators in Patient Education. Adult Learning, 25(4), 166-168. doi:10.1177/1045159514546217
Kehrel, U. (2015). The acceptance of process innovations in drug supply – An empirical analysis of patient-individualized blister packaging in stationary nursing facilities. International Journal Of Healthcare Management, 8(1), 58-63. doi:10.1179/2047971914y.0000000085
Jackson, M. (2008). Fundamentals of Nursing: Concepts, Process and PracticeFundamentals of Nursing: Concepts, Process and Practice. Nursing Standard, 22(32), 30-30. doi:10.7748/ns2008.04.22.32.30.b744
Lee, N. (2010). The Research Process in Nursing – Sixth editionThe Research Process in Nursing – Sixth edition. Nursing Standard, 24(46), 31-31. doi:10.7748/ns2010.07.24.46.31.b1086
Lu, C., Tang, S., Lei, Y., Zhang, M., Lin, W., Ding, S., & Wang, P. (2015). Community-based interventions in hypertensive patients: a comparison of three health education strategies. BMC Public Health, 15(1). doi:10.1186/s12889-015-1401-6
RodrÃguez-MartÃn, B., Stolt, M., Katajisto, J., & Suhonen, R. (2015). Nurses’ characteristics and organisational factors associated with their assessments of individualised care in care institutions for older people. Scandinavian Journal Of Caring Sciences, n/a-n/a. doi:10.1111/scs.12235
Svavarsdottir, E., Sigurdardottir, A., Konradsdottir, E., Stefansdottir, A., Sveinbjarnardottir, E., & Ketilsdottir, A. et al. (2014). The Process of Translating Family Nursing Knowledge Into Clinical Practice. Journal Of Nursing Scholarship, 47(1), 5-15. doi:10.1111/jnu.12108
Vaillant-Roussel, H., Laporte, C., Pereira, B., Tanguy, G., Cassagnes, J., & Ruivard, M. et al. (2014). Patient education in chronic heart failure in primary care (ETIC) and its impact on patient quality of life: design of a cluster randomised trial. BMC Family Practice, 15(1). doi:10.1186/s12875-014-0208-3
We can write this or a similar paper for you! Simply fill the order form!