Why are some children more challenging than others?
Be sure to address the following:
Identify and describe three risk factors which influence behavior (may include considerations of brain development).
Discuss how each factor influences behavior.
Analyze strategies teachers may use to support the process of changing or replacing behaviors.
SAMPLE ANSWER
Behavior Risk Factors In Children
Introduction
Some of the risk factors affecting behavior in children concern behaviorists and sociologists. The existing question that arises is why some children perform better than others do. Not only are they interested on behaviors of children to each other, but also on academic platforms. Therefore, the following discussion will engage in identifying and analyzing some of these risk factors. In addition, the paper will outline some of the indispensible strategies to be used by teachers to deal with such factors
Discussion
Poverty is one of the risk factors to affect behavior. In fact, it affects a child’s academic excellence, social behavior, and well-being. Those children who are reared in impoverished setting do face the risk of developing challenging behaviors. This is attributed to the fact that the children under these environments have a limited number of role models to orient them to positive behavior. According to a research done by Matson (2009), teachers in U.S. find a high rating of children aggression within classroom which is correlated to those children being exposed to community violence. The author concludes by attesting that poverty in most of the cases leads to such pessimistic outcomes as delinquency, school dropout/failure, and violence.
Risk factor to negative behavior can also develop during pregnancy. Fetal alcohol syndrome, which involves a woman taking alcohol during pregnancy, can have detrimental effects to a child during early development. Alcohol taking during pregnancy leads to permanent neurobehavioral and affective diseases that result to impaired central nervous system complication, behavior and cognitive malfunctions, as well as other physical disorders (Willis, 2009). Combination of these complications brings a situation where a child develops difficulty in verbal and nonverbal fluency. They exhibit a slow growth in cognitive development. Their behavior might in some case do not correlate to their current age because of the brain malfunction.
The other notable risk factor influencing behavior is violence. This factor goes hand in hand with child maltreatment. According to a study done by Szigethy, Weisz & Findling (2012) gives that U.S. records a high number of incidents where children are exposed to psychological, sexual, and physical abuse. In fact, more than three million children in U.S. are exposed to child maltreatment. This is catalyzed to the kids being introduced to all form of violence through television news, cartoons, and games (Willis, 2009). Therefore, when children are exposed to violence, whether directly or indirectly, they are more likely to change their perceptive of the world and values to a negative approach. In the effect, children’s ability to learn, to develop association with others, and ability to deal with stress is impaired.
However, there are solutions to the above risk factors. Teachers can evade the detrimental effects of poverty in affecting the behavior of children by consolidating help from different stakeholders from the society to help the children affected. On top of that, the teachers should encourage play between diverse and different children to develop skills that are impeccable to address a common goal, instill respect for each other, and establish cooperation between peers (Szigethy, Weisz & Findling, 2012). Those children who have developed violence-related behaviors should be introduced to the concept of self-control. This is by discouraging watching of violent games and cartoon, and encouraging the use of books that focus on empathy and caring. Above all, dealing with the root problem is very important, and teachers should take an initiate to advise pregnant mothers to avoid alcohol drinking during pregnancy to enhance affirmative cognitive development for the baby.
Conclusion
In summary, poverty, violence, and alcohol taking by pregnant mothers are one of the risk factors affecting behaviors in children. When special considerations are focused to bail out the affected children as well as those who are likely to develop bad behavior by such factors, will ensure that positive behaviors are nurtured and developed. This will see that children improve in both academic and in their social interactions in the society.
References
Matson, J. L. (2009). Social behavior and skills in children. New York: Springer.
Szigethy, E., Weisz, J. R., & Findling, R. L. (2012). Cognitive-Behavior Therapy for Children and Adolescents. Washington, D.C: American Psychiatric Pub.
Willis, C. (2009). Creating inclusive learning environments for young children: What to do on Monday morning. Thousand Oaks, Calif: Corwin Press. https://searchworks.stanford.edu/view/7735862
We can write this or a similar paper for you! Simply fill the order form!
Giving specific examples, evaluate the standard of ethics and morals of the media industry in China.
SAMPLE ANSWER
China’s Standards of Media Ethics
Introduction
Internationally, journalists are expected to conduct themselves professionally and ethically to exhibit the maximum standards of journalism as per given principles. Considering that China is not a collectivistic society, there is high observance of morality in this society mainly drawing from Confucianism teachings (Ambrose & Cross, 2009). The observance of morality is extended from observance of traditions from the grassroots to the media. This is destined to create a good rapport between different stakeholders within media industry. Therefore, the following discussion indulges in viewing some of the standards of media ethics and morals in China.
Discussion
The government of China strives to see that freedom of press is felt among its media stakeholders. Furthermore, it has established laws and regulations to regulate and control how these freedoms should be exercised. One of the standards of media ethics in China is accuracy of reports given (Beardsley, 2010). Media houses are controlled on the type of information they releases to the public. For example, media inform of radios and televisions’ news broadcast in China face strict laws pertaining the type of information broadcasted (Christians, Fackler, McKee, Kreshel & Woods, 2013). If a journalist is found conspiring to give out false information, criminal charges are laid against him or her.
The second aspect of morality of which is an ethical media standard is the respect to the source of information (Davison, Martinsons, Murata, Drummond, Li, & Lo, 2009). Chinese people, Fukawa & Erevelles (2014) and Wang (2011), have the tendency to respect people regardless of what they are. The government as well as the public expects that respect to be exemplified by the media. In simple terms, journalists should observe that anonymous of the source of information to be adhered for security purposes. Therefore, if a source of data dictates that his or her identity to remain anonymous, then it should be it. In other cases, journalist should not be engaged in stereotypical communication (Fortner & Fackler, 2011). According to In Couldry, In Pinchevski & In Madianou (2013), it is against the law in China to engage in such practices such as naming suspects of crimes before they are being charged. Still on the same platform of the respect for human rights in media ethics, diversity of human experiences and views should also be apprehended (Ip, 2009). What this means is that the tendency of journalists in China to discriminate people based on how unpopular they are, should be avoided at all cost. Still on the same line, Jung, Klein & Caldwell (2014) demand that photojournalist while on their line of duties should be very cautious to ensure that they do not expose or risk the safety of their subjects when taking photos to represent breaking news. To the maximum, as Keller (2009) argues, journalism should be ethical in showing compassion to those people affected unsympathetically by news broadcast. In addition, journalist still on the same line should use particular special sensitivity when handling juvenile and inexperience subjects.
In China like its counterpart Western countries, genuine information is appreciated. (Kleinman, Yan, Jun, Lee & Zhang (2011) gives that it is a serious offence to fund, buy, and give gifts such as tour incentives to corrupt a source of information. In reciprocal, journalists themselves are not allowed to accept favors and compensation from those personalities who might seek to affect coverage (Lu, 2009). Therefore, they should act independently. China’s strict media rules punishes such individuals who act in their capacity to influence programs and reports. Such penalties such as jail terms and revocation of licenses follow the victim. Media ethics and morals in China extend to incapacitation of other journalists (Sardy, Munoz, Sun & Alon, 2008). In China, journalists are put under strict guidelines to ensure that they do not intentionally incapacitate the efforts of other journalists. In addition, journalists are not allowed to cause bizarre using another journalist’s condition whether to the public or to the other journalists.
Accountability is another indispensable media ethic in China. It is the sole duty of a journalist to stress and clarify new topics and welcome conversation with the general-public over a specific journalist’s conduct (Sardy, Munoz, Sun & Alon, 2010). In addition, still on accountability, a journalist should encourage the critics from the public to air out their voices against the news media. It should be a promise as Wang & Young (2014) argues of a journalist to accept mistakes and correct them with immediate effect. To supplement the concept of accountability on media ethics, Small (2013), Shaw & McKeever (2012) and Spence (2011) attest that journalist should aggressively expose unethical malpractices of the news media. Journalist should stand firm to report such malpractices such as payment of sources of information to the court of law (Ip, 2009). Above all, journalist being accountable to their listeners, readers, and viewers should abide by the same elevated standards to which they hold each other.
Conclusion
In summary, China has an easy task in observance of ethics and morals in media. This is because of Confucians teachings, which aggressively stressed on people being good to all people regardless of race, status, or gender. Therefore, China progressively ensures that ethical and morals in media are observed to the latter. Offenders caught violating media ethics and morals are heavily punished as per given rules and regulations.
References
Ambrose, D., & Cross, T. L. (2009). Morality, ethics, and gifted minds. New York: Springer.
Christians, C. G., Fackler, M., McKee, K. B., Kreshel, P. J., & Woods, R. (2013). Media ethics: Cases and moral reasoning.
Davison, R. M., Martinsons, M. G., Ou, C. X. J., Murata, K., Drummond, D., Li, Y., & Lo, H. W. H. (2009). The ethics of IT professionals in japan and china*.Journal of the Association for Information Systems, 10(11), 834-859. Retrieved from http://search.proquest.com/docview/198795215?accountid=45049
Fukawa, N., & Erevelles, S. (2014). Perceived reasonableness and morals in service encounters.Journal of Business Ethics,125(3), 381-400. doi:http://dx.doi.org/10.1007/s10551-013-1918-5
Fortner, R. S., & Fackler, P. M. (2011). The Handbook of Global Communication and Media Ethics. New York, NY: John Wiley & Sons.
In Couldry, N., In Pinchevski, A., & In Madianou, M. (2013). Ethics of media. Houndmills, Basingstoke, Hampshire: Palgrave Macmillan.
Jung, Y., Klein, J., & Caldwell, M. L. (2014). Ethical eating in the postsocialist and socialist world.
Keller, P. (2009). Liberal democracy and the new media. Oxford: Oxford University Press.
Kleinman, A., Yan, Y., Jun, J., Lee, S., & Zhang, E. (2011). Deep China: The Moral Life of the Person. Berkeley: University of California Press.
Lu, X. (2009). A chinese perspective: Business ethics in china now and in the future.Journal of Business Ethics, 86(4), 451-461. doi:http://dx.doi.org/10.1007/s10551-008-9857-2
Sardy, M., Munoz, J. M., Sun, J. J., & Alon, I. (2010). Dimensionality of business ethics in china.Competitiveness Review,20(1), 6-30. doi:http://dx.doi.org/10.1108/10595421011019948
Small, M. W. (2013). Business practice, ethics and the philosophy of morals in the rome of marcus tullius cicero.Journal of Business Ethics, 115(2), 341-350. doi:http://dx.doi.org/10.1007/s10551-012-1401-8
Spence, E. H. (2011). Media, markets, and morals. Malden, Mass. [etc.: Wiley-Blackwell.
Wang, H. (2011). Protecting privacy in China: A research on China’s privacy standards and the possibility of establishing the right to privacy and the information privacy protection legislation in modern China. Heidelberg: Springer.
Wang, X., & Young, M. N. (2014). Does collectivism affect environmental ethics? A multi-level study of top management teams from chemical firms in china.Journal of Business Ethics, 122(3), 387-394. doi:http://dx.doi.org/10.1007/s10551-013-1761-8
We can write this or a similar paper for you! Simply fill the order form!
Hi I need the assignment by tomorrow evening with the copy of turntin report. i am attaching the guidelines for the assignment with the order. Thanks.
SAMPLE ANSWER
Introduction
Myanmar is a country situated in South East Asia and in the recent years the country has experienced an insurgence in the number of reported malaria cases with an estimated of thirty thousand reported cases annually. This has being mainly attributed to the rise of resistance to both chloroquine and artemisinin. This resistance is mainly because in the South Eastern Asian region there is a lower level of natural immunity unlike other parts of the world. (World Health Organization, 2010, pg 7)
Epidemiology
It has been shown that unlike the other malaria a prone region where plasmodium falciparum is more prevalent, in Myanmar plasmodium vivax malaria is more prevalent. I think this means that it easy to reduce the number of malaria cases and this is because vivax malaria is known not to be as fatal (and it exhibits frequent lapses) as plasmodium malaria and it also has a short incubation period. Although the malaria vivax is not as fatal I think this can easily lead us to conclude that an enormous economic loss will be encountered. (Rollinson, Hay, Price & Baird, 2013, pg 16)
It has been showed that the malaria containing parasites have shown degrees of resistance in Myanmar that is Mefloquine resistant falciparum and chloroquine resistant vivax. I think the best way to deal with such an issue is by conducting more researches so as to find more efficient drugs which the parasites will not be able to resist against. (Blas & Sivasankara, 2010, pg 60)
In Myanmar, just like in other Asian countries, malaria is common among the hard to reach population which mainly consists of the migrant population and the urban poor. In some areas though, the risk of contracting this disease depends on human behaviors. Since the risk of contracting malaria is not equal even in people in the same geographic region, I think there is the need to identify such populations and clearly understand the epidemiology of malaria among them so that the better interventions are sought. I think their behavioral risk factors also need to be identified. I also think it is important for these groups to access health care and this can be achieved through initiating control programmes. Although the prevalence of malaria in pregnancy is not common, I still think there is need to pay attention since prevention is better than cure.
Following the frequent malaria outbreaks that have been reported over the past decade I think continuous eradication projects should be carried out so as to avoid resurgence of malaria after the eradication project in Sri Lanka in 1967-1967
Social determinates
It has been shown that in Myanmar malaria is most at times transmitted during migration times as people migrate from one place to the other for example during the times of epidemics such as earthquakes and migrants moving into the country, people massively migrate from one place to the other. Those travelling from malaria prone areas have usually being found to be the main people transmitting this disease. I think the best way to curb this is by the government restricting movements from the malaria prone areas and if the movement is necessary and unavoidable then these people should be secluded to particular areas until all the necessary tests have been done on them and it has being proved that they do not suffer from malaria. (Blas & Sivasankara, 2010, pg 39)
Illiteracy has also contributed to the spread of this disease and this is so because, with a low level of illiteracy, the level of awareness concerning the disease is then definitely low. The best way to curb this I think is by initiating programmes that will ensure people are educated on malaria focusing on issues such as its spread, measures to curb its spread, the signs and symptoms and the treatment. I also think this issue can be addressed through introducing malaria related topics in school so as to increase the awareness level among the locals. (Blas & Sivasankara, 2010, pg 36)
Poverty has also been shown to be a major malaria social determinant. Most of the poor families in Myanmar cannot sustain the preventative measure such as use of mosquito nets and repellants hence making the disease more prevalent among the poor population. Malaria treatment also requires money and this has been difficult to seek among the poor families hence retaining a high mortality rate among the poor due to malaria. If it was up to me, I think this can be addressed through the government of Myanmar in association with other organizations such as the World Health Organization carrying out programmes that will ensure that all the poor families get all materials they require to prevent malaria such as nets for free. The same should also be done when it comes to treatment. (Blas & Sivasankara, 2010, pg 45)
Poor health services in Myanmar which is indicated by the presence of very few hospitals and health practitioners in general is another great and grave issue which has significantly contributed to the spread of malaria in the region. I think this can be addressed by the government through the ministry of health by allocating more funds which will aid building new health facilities, refurbishing the ones present, employing more practitioners and initiating campaigns aimed at fighting malaria. (Jameson, 2013, pg 101)
The burden of the disease
The disease has had a major impact on the people of Myanmar. Malaria, HIV and TB ranked the 5th place in country’s burden of disease. The total years of life lost due to premature mortality by malaria were 2000. The financial cost used in fighting malaria enormous for example in 2013 US$ 22.5 million was used. Usually, when the bread winners of a family are affected by the disease for example when the bread winner succumbs to the death, the family social and economic status suffers. (Martini & Chesworth, 2010, pg 360)
In my opinion I think the government should set aside funds that will cater for the families who have lost their bread winners. I think the government should also source for more funds that will enable them fight malaria from organizations such as the World Health Organization
Conclusion
My contribution in the group presentation was on the epidemiology of malaria in Myanmar. I focused on several issues as follows
Firstly, was the population of people in Myanmar affected by malaria and I was able to find out that there is a high number of reported cases for example in 2013 there were 198 million reported cases of malaria with an estimated 584,000 deaths reported with about 78% of these death cases being of children under the age five years old. (World Health Organization, 2014, pg 56)
Secondly, was the morbidity and mortality cases of malaria where I was able to conclude that over the past years there has been a decrease both the morbidity and mortality rates. For example in 1988 the morbidity rate was at 25 people per a thousand while the mortality was at about 10 per a thousand people. In 2010 the morbidity rate had fallen to about 7 people per a thousand people whilst the mortality was now at about 2 people per a thousand people. (World Health Organization, 2014, pg 63)
Thirdly, was the distribution pattern of malaria cases in the country and was I was able to discover that the North Western region of Myanmar was the most affected with over 75 reported cases per a thousand people. This was followed by the Central and Eastern regions where reported cases per a thousand people ranged from 1 to 10 people. I then found out that over the years the male population was more affected by the disease compared to the female population. (World Health Organization, 2014, pg 67)
Lastly, was and the epidemiologic triangle of malaria in the country where I was able to generalize that the environment played a major role in the spread of the disease for example bush land, lakes and ponds and that the most vulnerable population was comprised of; Children under five, pregnant women, people living in swamps and coastal areas, the poor, people living in remote areas, illiterate citizens and the IDPs. I also found out that the best way to reduce the vulnerability of these people was through conducting educations on malaria related issues, eliminating potential sources for mosquitos’ life cycles, using of protective clothes, insecticides and mosquito nets and anti-malaria drugs. (World Health Organization, 2014, pg 70)
Epidemiology plays a major role in the global health education. I say this because epidemiology provides critical information such as the pattern of the disease and its prevalence among the population. With such information we are able to determine the major determinates of the disease and the vulnerable population. This provides a background that will enable us know how to eradicate the disease and carry out the necessary preventative measures. (Rollinson et al…, 2013, pg 87)
Epidemiology also helps us reduce the impact of a disease, for example it is through this study that it can be determined that the disease has greatly affected the education system in the country hence calling for the necessary actions such as initiating programmers that will ensure that all the children who have been orphaned by this disease get the necessary required education.
It is thus important for the society to help in the fighting of malaria in conjunction with other organizations such as the World Health Organization.
References
Blas, E., & Sivasankara, K. A. (2010). Equity, social determinants and public health programmes. Geneva: World Health Organization.
World Health Organization. (2010). Guidelines for the treatment of malaria. Geneva: World Health Organization.
Rollinson, D., Hay, S. I., Price, R., & Baird, J. K. (2013). The Epidemiology of Plasmodium vivax. Burlington: Elsevier Science.
Manguin, S. (2010). Biodiversity of malaria in the world. Chestghum: Health Sciences.
Martini, I. P.,Chesworth, W. (2010). Landscapes and societies: Selected cases. Dordrecht: Springer.
Jameson, M. (2013). The impact of malaria in South East Asia and the tropical regions. Burlington: Elsevier Science.
Elizabeth, A., Casman, H.,& Dowlatabadi. (2010) The contextual determinants of Malaria. Springer Australia.
Malaria in Myanmar
Marking Criteria
Description
Available
Actual
Introduction
Identify selected topic and provide brief background to the topic
3
Reflection and Analysis
Provide a critical reflection of the selected topic under the set objectives in relation to your perspective on the
1: Epidemiology
2. Social determinates
3. Burden of disease
Critical reflection is supported by up-to-date (less than 5 years) and peer reviewed literature, (may include journal articles, bioethics literature and relevant professional and government documents)
APA referencing style is used
7
Conclusion
Synopsis of your contribution to the group presentation and the value of this to global health education .
10
TOTAL
20
We can write this or a similar paper for you! Simply fill the order form!
4. Priority of risks.
(a) Calculate the Priority of the risks by first assessing the consequences, exposure and probability using the Risk Level Calculator below
(b) Complete the Safety Sign Check List
5. Control Methods. Describe how you would control each hazard and or risk using the hierarchy of control and any induction and training necessary.
SAMPLE ANSWER
Implementing and Monitoring WHS
Employees and customers are often faced with risks when in the business premises. Managers try to minimize the risks occurring by trying to mitigate them to ensure that the workplace is safe and the workers and customers are also safe and free from hazardous exposure. A risk is not avoidable and is present in everyday activities. A risk can be defined as an uncertainty that surrounds events to be performed in future and the outcome (Chance & Brooks, 2015). That is the expression of the likelihood and impact of an activity which has the potential of influencing the achievement of the objectives of a company.
However, this paper addresses four hazards that might be experienced in Winter Garden noting down the potential risks, prioritizing the risks by calculating the priority list and finally provides the control methods to control each hazard using the hierarchy of control.
Identification of risks in the workplace
There are four common types of hazards that employees are exposed in the workplace. That is Physical hazards, ergonomic hazards, biological hazards and chemical hazards (Burke, 2013). The most common type of workplace hazards are Physical hazards. Four hazards that might occur in Winter Gardens include:
Slip and fall accidents
Negligent security
Elevator and Escalator accidents
Food poisoning
The above mentioned hazards are real and often occur in workplace. The management should often develop measures to mitigate such risks in order to have a safe working environment.
Potential of risks
Clients in Winter Gardens might succumb to injuries and hazards such as tripping and slipping. These injuries expose clients to potential risks such as broken limbs, sprains, injured necks and backs etc (Chance et al., 2014). Security negligence may expose the clients visiting Winter Gardens to crime which might lead to loss of property or even injuries in the event of crime or terrorism related crimes. Elevators and escalators also expose clients to accidents when they move from one place to another in the Winter Gardens. Food poisoning is also a potential danger which can occur even in exotic places like Winter Gardens. Food poisoning might expose individuals to risk of being diagnosed with E. coli and Salmonella. Therefore, it is important to observe safety measures in the workplace (Hoyt et al., 2013).
Priority of risks
Type of risk
Slip and Fall accidents
Consequences
VL
1
exposure
VH
8
probability
C
10
Risk value
19
Negligent Security
Consequences
VH
8
exposure
L
2
probability
H
6
Risk value
16
Elevators and escalator accidents
Consequences
VL
1
exposure
H
6
probability
C
10
Risk value
17
Food Poisoning
Consequences
L
2
exposure
M
4
probability
VH
8
Risk value
14
Safety Control checklist
HAZARD OR RISK
YES
NO
LOCATION
1. Are people able to identify what protective equipment must be worn?
ü
2. Are employees and visitors required to keep specific instructions?
ü
3. Are any arieas restricted accesses to authorized persons only?
ü
4. Are any activities prohibited in the workplace?
ü
5. Are persons warned of any dangerous areas of risks?
ü
6. Are persons warned of hazards that may cause injury or damage?
ü
7. Can persons be injured due to the way that they carry out their tasks?
ü
8. Are dangerous goods stored or used in the workplace?
ü
9. Are fire-fighting appliances properly identified
ü
10. Is the lacation of First-Aid equipment clearly identified?
ü
11. Are emergency exists, evacuation routes and assembly areas properly identified?
ü
12. Is traffic flow and parking controlled around the workplace. With safe speed limits defined?
ü
Recommendations and Measures to Control Each Hazard
The best way to hazards is to put measures that can help in mitigating the risks involved. To avoid tripling in the garden, items within the buildings should be arranged in an orderly manner also to reduce accidents caused by tripling while at work (Rampini et al., 2014). All grease, food or water spills should be wiped off the floors immediately. On the same note, loose wiring and electrical cords within the environment should be taped on the walls or floors.
The management of Winter Gardens should also tighten up security and bar individuals having weapons from accessing the facility to prevent crimes that might occur due to negligence. Security also needs to monitor all security cameras within the facility especially the parking garage (Rampini et al., 2015). To prevent elevator and escalators accidents, the management of Winter Garden should ensure that all elevators and escalators in the facility are well maintained and put in place. On the same note, the organization should also address safety concerns that may arise during maintenance checks. Finally, food should be cooked properly and hygiene should be observed while handling either cooked or raw food to prevent the occurrence of food poisoning within the Winter Gardens.
References
Chance, D., & Brooks, R. (2015). Introduction to derivatives and risk management. Cengage Learning.
Rampini, A. A., Sufi, A., & Viswanathan, S. (2014). Dynamic risk management.Journal of Financial Economics, 111(2), 271-296.
Hoyt, R. E., & Liebenberg, A. P. (2011). The value of enterprise risk management. Journal of Risk and Insurance, 78(4), 795-822.
Burke, R. (2013). Project management: planning and control techniques.
We can write this or a similar paper for you! Simply fill the order form!
I want to know the cost to paraphrase this paper please.
SAMPLE ANSWER
Abstract
The United States of America offers the best health care services in the world. It is however unfortunate that some Americans still lack the best of the services due to varied reasons. Differences are evident along the lines of ethnicity and race. The less fortunate are mainly the non-white Americans, the blacks and the Indians. The situation has indeed attracted attention from researchers and academicians all over the globe. Quality health care should be available for all Americans regardless of their skin color. The health care system therefore needs to be more inclusive and available to people of different beliefs, sexuality, and religion among others. In general, a better health care system is needed to offer equal services to the entire population. Humanity is endorsed with intelligence that enable hem realize inequality and launch uprisings to fight for their rights. However, the affected groups are unable to air their concerns as a competent leadership is lacking in the system to call for quality health services to the groups.
Introduction
It is evident that change is required in health care but the lack of efficient leadership to drive the transformation offer the greatest challenge. Researchers have been reluctant in addressing the issue especially from the perspective of implementing changes that would result to equal services to people of different ethnicities. In some research works, however, researchers only point out the relation between health care for the public and emotional feelings. In this project, the role of appropriate leadership in driving transformations for provision of equal health care services to all Americans is discussed as a measure to ensure that the disadvantaged groups get their fair share. Studies carried out aim at improving health care services to all ethnic groups and races. Generally, emphasis is put on the minority groups
Disparities in the Provision of Quality Health Services to the Minority
In the US, ethnicity has been noted to influence access to health care with more difficulties for the non-whites. The research project takes a critical position and exhaustively examines the existence of disparities in access to health care for the minority groups. Transformation leadership is taken as the most appropriate vehicle in conveying the inevitable change required in the sector. In the paper, the influence of disparities in the health care sector on the implementation of the Affordable care act is examined and recommendations made on the best ways of handling the unacceptable situation. Extensive research is done to ensure that reliable evidence is used in the call exploration of the issue.
Research and review
Disparities in the health care sector as The Kaiser Family Foundation termed them entail inequality in care provision for Americans of different origin, religion, beliefs among other aspects of life (2013). With the disparities, different groups receive different levels of care and for the US skin color is among the leading factors leading to the differences. Agency for Healthcare Research and Quality wrote that differences are evident in the means in which diseases are handled in different populations as expected, disease outcomes also take the trend initiated by the variations in care provision (2012).
To further illustrate, the disparities also cause differences the type of diseases, injuries as well as disabilities and mortalities that different groups experience. From another perspective, differences result from insufficiency of health care services and cultural practices as a result of differences in social; and economic backgrounds. A link is noted between the disparities, emotions as well as the societal issues for different populations. As Deng and Gibson (2008) noted, people with poor economic background receive poor quality care as compared to their rich counterparts. It is also noted that financial instability plays a role in destabilizing the emotional status of individuals. Economic factors are noted to be one of the leading contributors in determining the quality of care people receive regarding their health. People with poor socioeconomic status often get low quality care and end up being emotionally discouraged.
Disparities in access to health care are translated in the life expectance for people in different categories. The minorities are generally found to lead a shorter life as compared to the more abled majority of the Americans. The Affordable Care Act initiated by president Obama has nevertheless achieved in minimizing the gap in health care access between people in different groups. Since its establishment, disparities in the health sector are noted to have subsided with an approach toward equality.
To solve the problem of disparities in the sector, it is important for the leaders to bring changes by collaborating with the framers of policies in the sector. by developing appropriate strategies, leaders would lead their subjects out of the emotional setbacks that result with inequality in access of high standard care in health institutions. It would be important if leaders for example, enact policies that would bring the poor closer to the rich. The policy makers also have the responsibility to solve the issue and end the long-felt disparities. By improving the socioeconomic status of the minority, All Americans would afford the current insurance plans and access to care would be generally be equaled for all. As the Agency for Healthcare Research and Quality wrote, Americans would afford quality health care and there would be minimal pooling of funds into healthcare (2012). It should be noted that most of the shortcomings in ensuring equal access to quality health care are financial in origin.
Research shows that transformational leadership is the best tool in identifying change, formulating a vision as well as executing the changes from an authoritative position to obtain the required changes. (Assanova & McGuire, 2009). To create equality, leaders should institute essential reforms that create coordination and supervisory guidelines for the care of the minority groups (Alino & Alban, 2011). By taking the measure, leaders would be at a better position to evaluate their progress and implement the policies provided on the eradication of the disparities in the health sector. Leaders are in addition expected to understand the need of emotional intelligence as well as its influence on the lives of their subjects. In the mode of leadership, leader’s performance should go beyond the anticipations. This would be achieved by encouraging integrity and fairness through support provision and recognition. As Deng and Gibson (2008) wrote, leaders in transformational leadership try as much as possible to avoid self-interest and would therefore steer up toward elimination of the disparities and lead to the achievement of equal care for people of varied backgrounds.
Gap in the literature
In this research, a gap is noted to exist at the level of leadership and therefore needs to be filled. Assanova and McGuire noted that there exist volumes of leadership that can address the healthcare disparities for the different groups (2009). It is important to address the gaps as by so doing, the transformational leadership and an approach to emotional intelligence forms the basics in achieving curbing the disparities evident in health care provision.
Problem Statement
Disparities in the health sector involve provision of care between for people of varied races, ethnicities, religions and many other divisions. The imbalance existing in the sector results from social, economic as well as cultural factors. Disparities are seen in many forms. Among them is the access to health care, attendance given for various diseases, as well as genetic and ethnic factors. Disparities eventually lead to differences in disease outcomes for different populations. In most cases, the outcome is more adverse for the disadvantaged minority groups as compared to the outcome seen in most other Americans. According to research, a link exists between disparities and low birth weights, and premature miscarriages among other reproductive health abnormalities. These issues often have significant effect on emotions and hence social activities undertaken by the different individuals.
Identifying Gaps to Impact Change
General health includes optimal body functionality inclusive of one’s mental status and functioning. Emotional senses also comprise the general wellness. It is therefore important that people’s emotions are protected from by offering the quality services to them without incidences of discrimination based on skin color, race, ethnicity, religion or any other factor likely to create divisions. It is necessary that leaders realize the impact of emotions on ones health. People often experience emotional destruction from discriminative treatment based on their status in the society. Obstacles noted to affect quality care provision to people include geographical locations, ethnicity, race, gender as well as one’s social status. Health disparities have effect on the psychological states of people and their performance is often influenced. Among personal factors affected by disparities are abilities, acquaintance as well as skills. In addition, health disparities are known to predispose people to chronic diseases and high death rates (Agency of Heathcare Research and Quality, 2012). Research has shown for example that African Americans have a 10% higher risk to cancer as compared to their white counterparts. The same case is seen with diabetes and other common chronic illnesses.
It is also notable that minority groups are less likely to consult private doctors as compared to the people in the majority groups. Poor access to health services is one of the factors that predispose the minority to diseases. Again, the problem roots from the economic status of the people. It is however saddening that the gap between the rich population and their poor counterparts often widens instead of narrowing. The whites in America continue to access health services with increasing efficiency while the situation worsens for the blacks. Such situation as Agency for Healthcare Research and Quality wrote impacts negatively on the livelihood of the minority groups. Minimizing the disparities in the sector would boost emotions at the personal level leading to improved health conditions for the minority groups. Transformational leadership that aims to care for emotional intelligence would lead to better lives for the minority groups and they would in turn enjoy a longer life span.
Personal Public Health Leadership Theory
One of the key pillars of an organization is its leadership. There has been intensive research to explore on appropriate forms of leadership. Researchers have developed multiple theories explaining leadership. Qualities that distinguish quality leaders have been outlined in many research works. Transformational leadership is one of the theories that offer explanations on most appropriate leadership practices. The theory emphasize on individual achievements. The theory for instance indicates that charisma is a necessary trait for leaders. Together with the ability to lead people toward high productivity, charisma makes a leader more appropriate to execute transformations (Lang, 2010). The bond that exists between transformational leaders and their subjects is a motivational factor and reduces incidences of distrust between the parties. In transformation leadership therefore, behavior of the parties is modified to allow healthy interactions between the parties. The mode of leadership in addition orients employees toward a common goal making it easier for organizations to run smoothly. A serving interaction is established in the organization rather than that dominated by a feeling of power (Bass & Riggo, 2006). In addition, the leadership depicts direct relation with personal characteristics. Confidence and emotional feelings are depicted in transformational leadership. In this way, leadership integrates personal attributes with management. It is therefore necessary that transformational leaders be constituted in the management of organizations that require reforms. The style of leadership would work for situations requiring behavioral change in addition to improved management.
Nature of Organizational Change in Healthcare using transformational
Leadership approach
Professionals in health care provision are working to ensure that improvements are noted in the sector. Differences in care provision based on ethnicity, race, religion and color are intolerable for the profession. Leaders in health care are expected to be skillful and to depict competence by being emotionally supportive. The disconnection between leadership and emotional competence should be corrected for the best outcomes on the move to improve equal access to quality health care.
It is important for the framework employed in closing the gap to ensure that health goals are pursued. The framework should offer strategies to which leaders are expected to base their decisions. Such strategies should see to the reduction of individual interests and prioritize on achievements as an organization. By using such leadership methods, the disparities seen in quality health care provision would be solved.
A Representation of the Public Health Leadership Theory
Set Directions: Mission, Vision and Strategy
Fig.1 Transformational leadership style cycle using emotional intelligence
Fig 2 The Nature of Organizational Change in Healthcare using transformational Leadership approach.
How the Visual Representation addresses the Literature Gaps
The system addresses gaps by development of concepts from scientific methods of data collection (Les & Magdelena, 2008). Among the developed concepts are theories that that explain different situations in from a scientific approach. The representations are scientific in origin and are the concepts are therefore reliable to refer to in order to understand scientific issues. After identification of the relevant issues, leadership strategies can be formulated to help solve the problems. Generally, visual representation offers proper understanding of situations which in turn allow for development of appropriate leadership techniques to handle the issues.
Method of Data Collection and Analysis
Data was collected by the use of structured questionnaires. Data analysis was enabled by the use of the SPPS statistical software as well as Monkey Survey.com. Data evaluation on the other hand was done through T-test. To maintain the validity of the research, randomization was used in selection of participants in the study. To evaluate transformational leadership, the Pearson coefficient was used together with ordinal and nominal measurement scales. By the use of the tools, the impact of transformational leadership on the lives of the minorities in the US was determined.
Significance of the Study
The research study addressed a problem that is often neglected by researches. The research may open the way for more comprehensive studies regarding provision of quality services to the American minority groups. The study also offered transformative leadership as an approach to overcome the disparity. The research outcome provides important information and strategies that would help in handling the disparities.
Ethical Considerations
All activities in the study were bound within ethical requirements. To further guarantee privacy, standard guidelines regarding information handling will be strictly adhered to. As a requirement, the study will be approved by Public Health Department of Walden University. Permission will also be sought from relevant authorities in the community under test.
Conclusion
The health sector in the United States has been characterized with disparities for long. As observed, the disparities root from differences between the rich and the poor. The larger the gap between the two classes, the more the disparities observed in the health sector. Among the key factors resulting to the disparities are socioeconomic status of the people, ethnicity, race, religion, values and beliefs among others. The best means of addressing the disparities as seen in this research involve the use of transformative leadership. Such leadership should see to increased social welfare among the minority and increased wages to close the gap. All Americans are entitled to equal access to quality health care and leaders should ensure that citizens enjoy the right. Emotional intelligence should also be coupled with transformative leadership for fast achievements in provision of equal access to services.
Alimo-Metcalfe, B., & Alban-Metcalfe, J. (2011). The development of a new transformational Leadership Questionnaire . The Journal of Occupational and Organizational Psychology, 74, 1 – 27 .
Creswell, J. (2011). Research Design: Qualitative, quantitative, and mixed methods approach Custom Ed. Thousand Oaks, CA: Sage Publication.
Deng, L. & Gibson, P. (2008). ” A Qualitative Evaluation on the Role of Cultural Intelligence in Cross-Cultural Leadership Effectiveness,” in International Journal of Leadership Studies, Vol. 3 Iss. 2, 2008, pp. 181-197, 2008 School of Global Leadership & Entrepreneurship, Regent University. URl.
Lang, M. (2010). Transformational leadership: fundamental, models, differences and impact on employees Norderstedt. Germany. Duck und Bindung.
Les, Z & Magdelena, L (2008) Shape Understanding System: The First Step towards the Visual Thinking Machines. Heidelberg. Springer.
We can write this or a similar paper for you! Simply fill the order form!
DuPont Analysis of companies for the past three years
DuPont Analysis of companies for the past three years
Order Instructions:
This week the writer will build on what he completed on the first week with order #112856 and will add the respond to the questions hear below as week 2 and will take the completed solutions from #112856 and add as week 1 at the beginning of the paper like that he will be building the paper up as we go forward. Remember this is a continues assignment and it will run for a couple of weeks. As mentioned earlier, week one was order #112856 and the response to the questions below will be week 2 so take note and I have resubmitted a template hear to use to add week one and 2, so let the writer pay attention to those details. Also when the writer adds the references from 112856 to this paper, he must make sure the are in alphabetical order as per APA.
• Investment Analysis and Recommendation Paper – continued from #112856
During this week, you will assess the company you selected for your Investment Analysis and Recommendation Paper relative to its competitors in terms of financial ratios. Financial ratio reports are available on numerous Web sites (examples: Reuters, Google, Finance, Hoovers). Remember, different Web sites may use slightly different definitions.
Using income statements and balance sheets for your company AND at least one of its main competitor’s, respond to the following:
• Calculate the DuPont identity for both companies for the past three years.
• Discuss any differences and/or trends that emerge.
Write up a 2-page summary minimum of your findings, including any calculations you made, and how you gathered your information. Please follow the template and present the information base on the templates headings.
SAMPLE ANSWER
DuPont Analysis of companies for the past three years
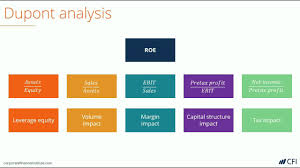
Return on Investment (ROE) is the is one of the most important company analysis tools that is used to measure how well a company manages and creates value to their shareholders. However, the values on the ROE can sometimes be misleading in terms of real value and risks associated with a particular investment. The numbers in the ROE can easily be misleading to financial analysis if the individual components of the ROE have not been broken down to their individual components. In this regard, DuPont can bridge the gap created by the ROE and provide a reliable measure of how the company creates value for its shareholders (Mitchell, Mitchell, & Cai, 2013). DuPont is the financial analysis tool that enables the breakdown of the ROE into its various individual components such as financial leverage, asset turnover, and profit margin (Haskins, 2013). The following is the financial calculation of DuPont of Chesapeake Energy Corporation, together with their competitor, Anadarko Petroleum Corporation (APC) (Cheasapeake Corp, 2015).
DuPont takes utilizes the basis of the individual component of ROE which is given by;
Profit Margin X Asset Turnover X Leverage Factor
Chesapeake Energy Corporation (CEC) Financials for the past three years
2014
2013
2012
Total Assets
$40,751,000
41,782,000
41,611,000
Shareholders’ Equity
$16,903,000
15,995,000
15,569,000
Revenue
$20,951,000
17,506,000
12,316,000
Net Income
$1,917,000
724,000
769,000
Anadarko Petroleum Corporation (APC) Financials for the past three years
2014
2013
2012
Total Assets
61,689,000
55,781,000
52,589,000
Shareholders’ Equity
19,725,000
21,857,000
20,629,000
Revenue
18,470,000
14,581,000
13,411,000
Net Income
(1,750,000)
801,000
2,391,000
In the year 2012;
The DuPont for Chesapeake Energy Corporation is given by
Net Profit x Asset Turnover x Leverage Factor
(769,000/12,316,000) x (12,316,000/41,611,000) x (41,611,000/12,316,000)
= 0.0624 x 0.256 x 3.379 = 0.054
The DuPont for Anadarko Petroleum Corporation (APC) is given by
(2,391,000/13,411,000) x (13,411,000/52,589,000) x (52,589,000/20,629,000) =
=0.1783 x 0.255 x 2.541 = 0.116
In the year 2013;
The DuPont for Chesapeake Energy Corporation is given by
(724,000/17,506,000) x (17,506,000 / 41,782,000) x (41,782,000/15,995,000) =
0.041 x 0.419 x 2.612 = 0.045
The DuPont for Anadarko Petroleum Corporation (APC) is given by
(801,000/14,581,000) x (14,581,000/55,781,000) x (55,781,000/21,857,000) =
0.055 x 0.21 x 2.55 = 0.029
In the year 2014;
The DuPont for Chesapeake Energy Corporation is given by
(1,917,000/20,951,000) x (20,951,000/40,751,000) x (40,751,000/16,903,000) =
0.091 x 0.514 x 2.411 = 0.113
The DuPont for Anadarko Petroleum Corporation (APC) is given by
(1,750,000/18,470,000) x (18,470,000/61,689,000) x (61,689,000/19,725,000) =
0.095 x 0.299 x 3.127 = 0.089
Differences and trend that emerge
In the year 2012, the operating efficiency of APC (0.18) was higher than that of CEC (0.06) as can be seen in their profit margins. In the same year, it can be deduced that the asset use efficiency of between the two companies are almost the same since they stood at 0.255 for APC and 0.256 for CEC. On the other hand, the financial leverage for CEC was higher (3.4) than the financial leverage for APC (2.5).
In the year 2013, the operating efficiency of APC (0.05) was still higher than that of CEC (0.04). In the same year, the asset use efficiency of CEC was higher than the asset use efficiency of APC. Similarly, CEC had a higher financial leverage in the year 2013 than APC. Overall, it can be deduced that CEC performed better than APC in the year 2013.
In the year 2014, the operating efficiency of APC (0.095) was higher than that of CEC (0.091). However, the asset use efficiency of CEC stood higher (0.5) than that of APC (0.3). On the other hand, APC had a higher financial leverage (3.1) than CEC (2.4) as can be deduced from the financial calculations. The higher the financial leverage, the better a company is placed to provide good value for its shareholders (Brian, Sandra, & Jennifer, 2013)
References
Brian, J. H, Sandra, M. T. & Jennifer, C. H. (2013). Benefit Corporation Concerns for Cheasapeake Corp. (2015). Company Profile: Chesapeake Energy Corporation. MarketLine Financial Service Professionals. Journal of Financial Service Professionals. 74-82.
Haskins, M. E.(2013). A decade of DuPont ratio performance. Management Accounting Quarterly, 14(2), 24-33.
Tips for Success
The M6A3: Application of the Nursing Process Paper counts as 30% of your grade for this course.
We suggest that you develop and outline and use the following time-line as your guide for completing your paper:
Week 1: Review the requirements for the paper.
Week 2: Begin developing an outline for your paper.
Week 3: You should have your outline completed.
Week 4: You should be using your outline to write your paper.
Week 5: Continue work on your paper.
Week 6: Finalize your paper and submit by the end of the week.
linked item M6A3: Application of the Nursing Process Paper
Using APA format, the information from this course, and your assigned readings write a six (6) to ten (10) page paper (excludes cover and reference page) addressing the application of the nursing process to a patient care scenario. Use these directions and the scoring rubric as you develop the paper. Outlines and abstracts are NOT required with this paper. Do not include the scenario in the paper
A minimum of three (3) current professional references must be provided excluding a nursing diagnosis book. Current references include professional publications or valid and current websites dated within five (5) years. Additionally, a textbook that is no more than one (1) edition old may be used. Do not use abbreviations…write out everything.
The paper consists of three (3) parts:
The meaning and use of the nursing process in making good nursing judgments that effect patient care
The development of a plan of care using the nursing process for a specific patient situation
The preparation stage for a teaching plan to prevent a recurrence of a similar situation
The following sheet will assist you when composing the plan of care for the paper: Overview of the Nursing Process.
Part 1 (3-4 pages)
Review the required readings about the nursing process. In your own words, define each step of the process and provide an example for each step.
In the implementation step, what is meant by direct and indirect care as described by the Nursing Intervention Classification (NIC) project?
Discuss the three (3) types of nursing interventions (nurse-initiated, dependent, and interdependent) that applies to the patient care situation. Provide an example of each (refer to your textbook).
Explain how the nursing process provides the basis for the registered nurse to make a nursing judgment that results in safe patient care with good outcomes.
Discuss how the registered nurse evaluates the overall use of the nursing process. Identify three (3) variables that may influence the ability to achieve the desired outcomes for the patient.
How is the plan of care modified when the outcomes are not met?
How does the RN use the nursing process to make decisions about the priority of care?
Part 2 (3 pages)
Patient scenario
A 78-year-old man is living in an assisted living facility. He is able to walk very short distances and uses a wheelchair to transport himself to the communal dining room. He administers his own medications independently and bathes himself. Over the last year he prefers to remain in the wheelchair even when in his room. He has a history of CHF, hypertension, hyperlipidemia and lower extremity weakness. He is able to state his current medications include metoprolol (Lopressor) 50 mg once daily by mouth, furosemide (Lasix) 20 mg once daily by mouth, Quinapril (Acupril) 20 mg once daily by mouth, atorvastatin (Lipitor) 20 mg once daily by mouth. During a routine examination, his physician noted a pressure ulcer over the ischium on the right buttocks. The wound is oval about 10mm x 8 mm, with red and yellow areas in the middle and black areas on some surrounding tissue. It has a foul odor. The patient had been padding the area so “it doesn’t get my pants wet”. The physician arranged for him to be admitted to the hospital in order for intravenous antibiotic therapy and wound care to be initiated. After being admitted to the hospital his medications are: metoprolol (Lopressor )50 mg orally every 12 hours, furosemide (Lasix ) 40mg once daily by mouth, quinapril HCl (Accupril) 40 mg once daily by mouth, cefazolin (Ancef)1.5 Grams in 50 mL 0.9 % Normal Saline intravenously three times a day. The result of the wound culture identified Methicilin-resistant staphylococcus aureus. After a surgical debridement of the black tissue a SilvaSorb® (antimicrobial gel) dressing was ordered daily.
Develop a Plan of Nursing Care for this patient that includes all steps of the nursing process:
One (1) actual NANDA-I nursing diagnosis statement addressing the priority problem the patient is experiencing. You need to provide the entire nursing diagnosis statement. For example: Acute pain, related to tissue trauma, as evidenced by patient rating pain at 7 on the 0-10 verbal pain scale. Provide a rationale, with evidence, why this nursing diagnosis is the priority for this patient.
What is the assessment data that supports the use of this nursing diagnosis? These are the assessments you will collect to determine if the patient has this nursing diagnosis. For example: Will assess the patient’s pain using the 0-10 verbal pain scale.
One (1) expected outcome (realistic, measureable and contains a time frame). that addresses the diagnosis and meets the criteria for an expected patient outcome. Discuss whether the outcome is a cognitive, psychomotor, affective or physiologic outcome. Discuss why the time frame selected for the evaluative criteria was selected. Use evidence as the basis for the time frame and criteria. You need to be specific to this particular patient. For example: Patient will rate pain at 3 on the 0-10 verbal pain scale. Of course, you would also need to answer the rest of the items in this section.
Four (4) nursing interventions that includes at least one (1) nurse-initiated, one (1) dependent, one (1) interdependent intervention. Label your interventions as above. Provide a rationale for each intervention that is evidence-based. Lastly, your interventions must be able to move the patient toward the achievement of the outcome. Select interventions, you as the RN can perform, that could reduce the pain and provide the rationale as to why; be sure they are evidence-based. For example: Teach patient guided imagery to distract attention and reduce tension.
Part 3 (1-2 pages)
To assist the patient in preventing a recurrence of a similar incident once he returns to the assisted living environment, the RN needs to develop a teaching plan. Use the nursing process to consider the information the RN would need prior to development of the plan. Respond to the following and be able to support your answers. You will not be developing a teaching-learning plan but demonstrating using the teaching-learning process to prepare for an individualized plan.
How does the RN decide the format of the teaching plan, i.e., written, verbal, or other?
How does the RN know which information needs to be included?
When does the RN determine how and when to evaluate the teaching-learning process?
Compose your work using a word processor (or other software as appropriate) and save it frequently to your computer. Use a 12 font size, double space your work and use APA format for citations, references, and overall format.
SAMPLE ANSWER
Nursing Process and Nursing care plan
Part 1: Nursing Process
Nursing process is the key factor that facilitates the nurses in delivering quality patient centered care. Nursing is defined as the science and art concerned with protecting and promoting peoples psychological, physical, psychological and cultural aspects. The science is based on a big theoretical framework whereas its art is depicted on the caring capacities and skills of each nurse. The concept of nursing process was established to defined to guide the nurses when making decisions on care provision and it involves five major steps namely; a) Assessment, b) diagnosis, c) planning/identification of outcome, d) implementation, and e) evaluation (Bruylands Et al., 2013).
Assessment is the first step of nursing process and involves gathering of information and data concerning a particular event. The nurses are encouraged to perform holistic care assessment of both patient healthcare history and physical examination so as to determine the specific healthcare demands of a patient. The data gathered is sorted, organized and documented for future references. Nursing diagnosis is the second step in nursing process; which involves analysis of the assessment and data gathered. Diagnosis process is conducted with the aim of establishing the patient’s specific healthcare needs. It involves identifying the actual problem including disease clinical manifestation. It also includes identification of risks factors and ways to improve patient’s outcome (Liu, 2013).
Planning step entails all activities geared towards development of priorities, objectives and the identification of the desired outcomes. It involves identification of specific nursing interventions as documented by action plan. Nursing action plan is effective if it is guided by Maslow’s hierarchy of needs and the Betty Neuman’s system theory. The implementation process involves putting the action plan into action to achieve the desired outcome set for each patient. The patient continued to receive treatment and quality care until their healthcare condition is achieved. The last step is evaluation and it involves assessing of the outcomes to see if it is congruent with the action plan. If the outcomes are negative, the interventions are modified appropriately (Fleming, 2014).
According to Nursing Interventions Classifications (NIC), direct nursing interventions refer to nursing interventions which involve direct interaction with the client/patient. For example, medication therapy being provided to person with congestive heart failure. Indirect nursing interventions include strategies that are implemented to improve patient’s health but the client is indirectly involved. This includes issues such as introduction of hourly rounding’s in hospital to reduce the number of hospital falls. Nursing interventions are classified into three broad categories including; a) dependent, b) interdependent, and c) independent intervention. Interdependent intervention involves nursing actions that are implemented through partnership and teamwork. It involves intensive consultations across the healthcare provider before any intervention is implemented. These includes actions such recommend surgery to patients with hyperthyroidism. This will only be done if all other therapy implemented has failed, and it involves a lot of consultation between the healthcare providers before the decision is made. The dependent interventions involve strategies that are recommended by higher health care authorities to the nurses. These include actions such as terminating patient’s medication due to reactions. The independent intervention includes all actions that can be implemented by the nurse without any consent from the authority. These involve all practices permitted by nurse practitioner scope of practice (Kehrel, 2015).
The nursing process guides the registered nurse in taking patients medical history while still remaining culturally competent. Nursing process requires the nurses to identify the healthcare problem, identify the etiology analyze the risk factors. Using the data generated form these process, the nurse can design patient focused action plan. The process also guides the identified intervention implementation in an orderly and structured manner. The outcomes expected are goal oriented and focused in providing care to the patient (Lu Et al., 2015). The process requires documentation in each step and well communicated whenever it is necessary. The nurse interventions are then evaluated to check if they match the expected patient outcome. The evaluation process requires joint effort between the healthcare providers; and where the outcomes are not achieved, it may require a little bit of brainstorming to identify the gap and to establish the variables that need to be re-evaluated. Some of the variables that can be re-evaluated include the data gathering/ assessment to check if the information was collected thoroughly or there was some information that were overlooked. The second variables include diagnosis to check if risk factors were adequately explored (Vaillant-Roussel Et al., 2014).
In some cases, the etiology can be wrong or inadequately explored. In some cases, the expected outcomes and interventions developed could be unrealistic or unreasonably unmanageable. If the outcomes are not met, the nursing process begins all over again from the assessment, diagnosis and action plan to implementation. This time, the nurse can involve other peers so that they can contribute to the healthcare dilemma and hopefully identify the relevant ideologies in establishing the best intervention. The best intervention is the evidence based one. The nurses need to make thorough research to identify the best practice which must be agreed by all the health care providers and the stake holders involved. This way, the nursing processes helps the registered nurse by helping then identify and define the problem, gather the healthcare information relevant to the matter and to generate the best possible conclusions (Svavarsdottir Et al., 2014).
Part 2: Nursing care plan
Assessment
George King lives in a residential care facility. His movement is restricted and mainly depends on wheel chair. He can manage the daily living activities such as bathing and dining. He likes living in isolation. He has history of Cardiac Heart Failure disease, hyperlipidemia, and hypertension and lower extremity weakness. He is under the following medication. His previous medication including Lopressor 50 mg, Atorvastatin 20 mg, Furosemide 20 mg and Quinapril 20 mg.
He is currently on Metoprolol 50 mg; Quinapril 40 mg, Furosemide 40 mg which are administered orally and cefazolin 1.5 g diluted in 50 mL 0.9% normal saline which is administered thrice a day. Recent routine medical checkup reported a pressure ulcer on his right side of the buttock. The ulcer is estimated to be around 10 mm by 8 mm. It is red in color with yellow sports all over it. The ulcer produces foul odor.
Physical examination
Height: 5’8”; Weight: 56 kg; Temperature: 36.60C; Pulse: 90 BPM; Respiration: 22/Minute; Bp: 160/7 80 mm Hg: Skin is most but pale; the pupils dilated; the neurovascular system, muscular system and gastrointestinal system are intact. The patient complains of memory loss.
Nursing diagnosis
Manage the pressure ulcer
Pain relieve
Patient education
Pathophysiology
The pressure ulcer is on the patient’s right side of the buttock. The ulcer is estimated to be around 10 mm by 8 mm. It is red in color with yellow sports all over it. The ulcer produces foul odor.
Outcome expectation
The main objective is to relieve the discomfort associated with the pressure ulcer. The patient has to verbalize reduction of pain by 80%. The patient must be taught on ways to ensure that the pressure ulcer does not progress and to prevent occurrences of the pressure ulcer in the future.
Nursing interventions
Establish the main reason why the patient prefers to use the movement aid rather than walking. This will facilitate identifying strategies to ensure that the patient does not remain sitting most part of his life
Record the patients agility to record and monitor the patient pattern of movement so as to determine alternative walking aids that can be used other than the wheel chair
Nurse will conduct evidence based practice that can be applied to reduce progression of the disease and to relieve as well as cure the pressure ulcer nursing interdisciplinary approach.
Educate the patient on behavioral modification such as mild exercises that can be done routinely to ensure that the patient does not remain seated most part of his life
Rationale and evaluation
The patient verbalizes pain relief. There is little discomfort. The main reason the pressure ulcer occurred was the prolonged sitting in one position. The patient verbalizes the understanding of the disease pathophysiology
The routine monitoring and increased exercise relieved the patient pressure ulcer. The patient was also advised to use roho cushion seats to reduce the pressure on the wound
The teaching program was objective and realistic. The RN is considering to teach other patients on strategies to reduce the pressure ulcer
Part 3: Patient teaching plan
Working in partnership between the patient and the healthcare provider is important because it makes it possible to establish an all-inclusive relationship between these two parties. The man aim of partnership is to improve the quality of care. Communication is a key factor in teaching the patient on the best self-care management. Patient education program is important because it enables patient understand their health conditions thereby improving their self-esteem. The registered nurse is responsible for the development of a teaching plan; and during the process, the nurse should put several factors into consideration. To decide the format of teaching, the nurse must be close with the patient so as to identify their specific care needs that needs to be addressed through education (Fleming, 2014).
The main objective for patient education is to empower the patient, and once the teaching process initiates, it should not cease until the registered nurse is sure that the patient can take great care of themselves. The patients’ health care demand can be assessed through physical examination and through consultation of medical history so that the nurse can identify the specific patients’ healthcare requirements. Based on the patient’s assessment report, three approaches can be used to teach the patient. Cognitive approach involves using the patient cognitive function. The affective teaching involves applying of social cultural values and beliefs to make the patient trust the registered nurse education. This is particularly important when dealing with patient who belief in traditional and cultural values. Psychomotor involves physical teaching to the patient. Additionally, the nurse should use the best format based on the patient age, education back ground and cognitive function to strategize if he/she will use verbal, written or audiovisual approach (Bruylands Et al., 2013).
Using the best approach, the nurse can identify the best intervention for each need. This includes identification of long term and short term objectives. Other close persons that interact with the patient can also join in the teaching process so that they can accord the patient the support he/she needs. For the mentally challenged person, the psychomotor teaching approach is the best. For the elderly, the registered nurse is advised to use audiovisual approach because it makes it better for the patient to understand. The young and those whose cognitive function is in good condition can be taught using cognitive approach and both verbal and written format. The registered nurse should always check for feedback to evaluate if the patients completely understand the education completely. During the assessment, the nurse should assess weakness and strengths. This will enable the nurse to address the weakness better. Assessment can be conducted through questionnaires and observations. The report made can be used to enhance the patient teaching plan even more. In some cases, the objectives may not be realized because they are too complicated or unmanageable. In this context, the registered nurse should begin the whole process again, and where necessary integrate the peers so that they can contribute to strategies to help the patient self-manage their care (Svavarsdottir Et al., 2014).
References
Bruylands, M., Paans, W., Hediger, H., & Müller-Staub, M. (2013). Effects on the Quality of the Nursing Care Process Through an Educational Program and the Use of Electronic Nursing Documentation. International Journal Of Nursing Knowledge, n/a-n/a. doi:10.1111/j.2047-3095.2013.01248.x
Fleming, J. (2014). A Future for Adult Educators in Patient Education. Adult Learning, 25(4), 166-168. doi:10.1177/1045159514546217
Kehrel, U. (2015). The acceptance of process innovations in drug supply – An empirical analysis of patient-individualized blister packaging in stationary nursing facilities. International Journal Of Healthcare Management, 8(1), 58-63. https://www.doi:10.1179/2047971914y.0000000085
Liu, J. (2013). Exploring nursing assistants’ roles in the process of pain management for cognitively impaired nursing home residents: a qualitative study. J Adv Nurs, 70(5), 1065-1077. doi:10.1111/jan.12259
Lu, C., Tang, S., Lei, Y., Zhang, M., Lin, W., Ding, S., & Wang, P. (2015). Community-based interventions in hypertensive patients: a comparison of three health education strategies. BMC Public Health, 15(1). doi:10.1186/s12889-015-1401-6
Svavarsdottir, E., Sigurdardottir, A., Konradsdottir, E., Stefansdottir, A., Sveinbjarnardottir, E., & Ketilsdottir, A. et al. (2014). The Process of Translating Family Nursing Knowledge Into Clinical Practice. Journal Of Nursing Scholarship, 47(1), 5-15. doi:10.1111/jnu.12108
Vaillant-Roussel, H., Laporte, C., Pereira, B., Tanguy, G., Cassagnes, J., & Ruivard, M. et al. (2014). Patient education in chronic heart failure in primary care (ETIC) and its impact on patient quality of life: design of a cluster randomised trial. BMC Family Practice, 15(1). doi:10.1186/s12875-014-0208-3
We can write this or a similar paper for you! Simply fill the order form!
Hong Kong healthcare systems can be described as mixed structure where private, public and alternative traditional medical therapy. Research estimates that the public hospitals offer about 90% of the inpatient and outpatient services. The private sectors cover 70% of the outpatient and in-patient services. The public sector obtains funds from the government taxation and complemented by little copayments amounts from the patients pocket. Due to the high life expectancy, Hong Kong population consists of the elderly people; consequently, this translates to a high frequency of diseases associated with old age such as psychosocial disorders, increased frequency of disease, high morbidity and mortality as well as the rate of government dependency. Consequently, the health care costs are high and has been anticipated to rise. This has increased pressure to avail quality care to the society and at affordable costs. There are numerous health care reforms and introduction of new policies to ensure that Hong Kong citizens are healthy (Huque, 2013).
Hong Kong healthcare system is robust and has provided quality care to the citizens for the longest time. The government has continued to strengthen the healthcare system so as to improve the system. The life expectancy of the Hong Kong people is highest in world which is reported as 80.9 years in males and 86.6 years in female. The infant mortality is the lowest and is recorded at 1.6 per 1000 births. The growth rate is slow and is reported to be between 0.4 to 0.6% in the last three decades. The proportion of youths has continuously reduced by 5% from 17% in the last three decades. On the other hand, the number of the elderly people has continuously increased. The age trend in this nation indicates higher elderly than the youth. Whereas it is a good thing, this acceleration in the increase of the elderly people is not only affecting the nation’s Economic growth but also attributed to the healthcare burden especially among the chronic diseases (Lueng Et al., 2015).
Health care system in Hong Kong
Healthcare reports estimates that about 50% of diabetes incidences in Hong Kong are from the elderly people. This metabolic syndrome has been listed as the leading cause of death as it accounted for 1.4% mortality in Hong Kong in 2013. The psychological issues and mental health such as dementia has also been on the rise. These rates at which the psychological disorders are increasing seem to overburden the social workers making them seek for other alternatives. Other non-communicable diseases such as thyroid cancer, respiratory disorders such as influenza, pneumonia and asthma have been reported to be the leading cause for hospitalization (Wong Et al., 2011). The most communicable disease which has been reported in Hong Kong is rotavirus and gastroenteritis. According to world health report in 2005, 35 million of 58 million deaths reported in the world are attributable to non-communicable (NCD) diseases such as cardiovascular diseases, cancer, accidents and injuries. The increases in these NCD are attributable to unhealthy lifestyle which involves consumption of unhealthy dietary, binge consumption of alcohol and sedentary lives. These brought forth increased burden among the families, the community and the government at large.
With this background of health concerns in Hong Kong, it is evident that primary health care is the frontline factor that acts as an interface between the healthcare system and the population. Effective primary care indicates that there are greater equity in healthcare and that care is easily accessible and at an affordable cost. Literature indicates that there effective partnership and collaboration between the healthcare and service users provides the best patient outcome including reduced emergency visits, better preventive care, better self-management for diseases with chronic diseases and reduced hospitalization cost. With the increased cost of care; and the challenges facing the health systems in Hong Kong calls for reforms in the primary care. HK government has been striving to reform its primary care. Fortunately, Hong Kong health care systems are among the best in the world (Kung Et al, 2014).
However, NCD is the leading burden in Hong Kong and it is projected to continue to rise in the future years to come due to advancement in technology. This poses major challenge to the public health. Research indicates that improving primary care has economic benefits. Promoting the primary health is a joint responsibility which requires everyone to participate in various sectors. The government major role is to provide legislative policies and frameworks which regulate service user and provider safety by controlling the hazards at the hazards; whereas the business sector’s major responsibility is to improve competitiveness to facilitate healthy choices. The Non-governmental movements and community organizations role is to implement the programs that focuses on health promotion on subgroups and the vulnerable and underprivileged people in the society (Wong Et al., 2015). To achieve a high performance demands a healthcare system demands higher expenditure and efforts in fighting the NCD. Investing in preventive care has been found to be the most the key factor in ensuring the economic development. For this reason, the government main objectives have been to provide the citizens with adequate support to enhance their sense of belonging and to maintain their dignity and enhance their worthiness. For the elderly and people living with disability, the government aims at providing cost effective care services. One of the systems that the government has embraced and is continuing to improve by expanding the home care based healthcare services as well as taking care through support such as “The Elderly Health Care Voucher Scheme (Yam Et al., 2011).”
The new infrastructure that the government has continuously planned to improve is the provision of healthcare services. The government has begun its initiative by increasing the number of hospital beds and surgery operation rooms to ensure that the healthcare capacity is widely accessible and meets the increasing demands. Additionally, the government has continued to promote primary care because it is the main link between the citizen and the health and social care. This involves expanding community healthcare facilities so that healthcare can be easily accessible. The government is also establishing frameworks specific for each NCD to promote the healthcare of individuals.
Secondly, the government has broadened the quota systems for both the general practitioners in the outpatient and in the in-patient services. There are ongoing strategies to improve the emergency department to ensure that waiting time for emergency care is reduced. The government in a joint venture with the private developers has increased service volume at an affordable cost. Some of these ventures include procuring of new haemo-dialysis services to ensure that the treatments are eligible to most patients with chronic renal failure. Radiology resources are also being outsourced for patients from underprivileged patients with chronic diseases (Liu & Yueng, 2013).
The government has continued to strengthen the geriatric rehabilitation services and the outreach services at the community level. This is with the aim of improving quality of life of elderly, people with mental disorders and people living with disability. The government have also increased their regulations on the residential care for these people to ensure that the issue of safety and healthcare management. Currently, they are ongoing pilot study on the general outpatient Clinic and the impact of privatization of public program in Kwun Tong, Tuen Mun and Wong Tai Sin districts. This is with the effort to increase the scope of care for the long term care of chronic diseases. The infrastructural development involves all the sectors in health including the mental health concerns. For example, the government is planning to increase the number of hospital beds in the largest mental health hospital in Siu Lam Hospital (Mercer Et al., 2010). This strategy aims at clearing up cases of severe complications of mental health associated with the prolonged waiting lists before the sick patients are attended to. This aims at strengthening the manpower of the mental health expertise through the introduction of peer support for patients with mental disorders. To promote the healthcare of its citizen, the government is also supporting other alternative traditional medicine. The Department of Health acknowledges this therapy and has funded several researches to evaluate the feasibility of these medicines. Additionally, it has been indicated by the evidence based research that NCD is the major healthcare burden in Hong Kong. Therefore, the government has continued to regulate the nutrition and safety of the processes food. In fact, the food safety Laboratory in Pok Fu Lam is being expanded by the government to ensure that there is effective testing of packaged food product so as to safe guard the people safety (Owolabi Et al., 2013).
Additional to the establishment of these infrastructures that supports and promotes health, the department of health has implemented several pilot schemes that will provide financial care services to the elderly. This includes implementation of discharge support program to the patients after they are discharged from the hospital and have challenges self-managing their health. There are also on going pilot study to ensure that the elderly that need long the care such as Guangdong Residential care Service Scheme (Hui, 2010). These strategies are great and very beneficial to the the society and the nation at large. One cannot quantify the financial cost of any disease to the individual or even the community. Economic analysis indicates that the cost of treatment for healthcare associated with NCD, injuries and poisoning is higher than the cost of NCD prevention and would save Hong Kong citizens from suffering and reduce the death rates. The existing healthcare has limited focus on effective preventive strategies. There needs more resources to establish systems that will inform the public as well as empowering the society. The voluntary organization and the department of health need to come together to integrate the necessary efforts towards both primary and secondary prevention strategies (Rashed Et al., 2014).
When socio economic evaluation was conducted on primary care in Hong Kong, it was found that most people use private health care as their main source of health care and often prefer to finance their health care costs from their pockets. The study indicated that Hong Kong citizen are more satisfied by the care quality compared to the public health care. The trend indicated that people who get quality care are those whose income is considerably high. This implies that only these people who are above average as compared to those who used public clinics. Several other studies have found a stronger association between the qualities of care with the socio economic background of a person. The lower income group cannot afford primary care which attributes to the increase in NCD incidences and mortality rates. Even with the Voucher system which was established to help the elderly whose main aim was to provide financial assistance to the elderly so that they can also access care in the private sector. Such schemes are meant to reduce burden on the public health care facilities (Hui, 2010).
This is particularly important because Hong Kong epidemiological studies indicate that NCD are at high prevalence’s among the old and the low income households. It is estimated that the prevalence rate for chronic illness in Hong Kong is five folds higher in individuals above 65 years than the youth. The level of education is also associated with better health care and lower incidences of overweight. People with low education reports higher rates of diabetes type 2, hypertension and cancer (So Et al., 2012). Despite the increase in health care disparities, the department of health has offered little if any solutions to rectify the prevailing social and health care disparities. Most studies indicate that much economic costs can be saved through collaboration and working in partnership between the service user, service provider and other stakeholders whose energy is geared towards healthcare protection and promotion. Through pooled knowledge and information sharing, the existing disparities can be reduced effectively by applying public regulations and policies and collaborative actions by the public actions. The actions could range from investing in human capital to quality education. These mechanisms are the best approaches to combat poverty through increased employment (Rashed Et al., 2014).
The best strategy to reduce the prevalence of NCD is through an establishment of a clear vision which focuses on reminding people on the long term outcomes of their effort. For a successful strategic framework, the Hong Kong must inform her citizens on the advantages of maintaining their health. This in turn will establish a caring community which integrates all the relevant stakeholders to ensure that the community sustains healthy lifestyle as guided by competent healthcare providers. Consequently, the country will establish a sustainable healthcare culture which aims at promoting health and incorporating strong elements of disease prevention with equal strength as the curative care among the public. This will significantly reduce the disease burden including premature mortality due to NCD or disability associated with NCD (Lam, Liu & Wong, 2012).
However, not even the voucher scheme that has facilitated reduction of health care burden. The NCD still remains a burden to the health ministry. This implies that it is time the government seeks other approaches to promote cultural change which places higher value preventive care than the curative care. It has been suggested that the financing healthcare reform is more of a political move than a strategy to help the healthcare industry. The problem of the aging population is here to remain and so is the issue of increase in healthcare expenditure. There needs a critical analysis in the health care to look into new approaches that will ensure that the society health is protected, promoted and sustained. There are other numerous non ambitious elements that the government can explore to promote health which will involve the health care providers, service users and other relevant stake holders so that they can be collaboratively reach to a consensus and pave way for more improvements in the future (Cheng Et al., 2013).
Conclusion
In summation, it important for the department of health to establish strategic framework that will facilitate establishment of an environment which will promotes the health of the citizens. The government must engage the population in promotion of their health, their relatives and the community at large. It is important for the health care department to establish strategies that will prevent or even delay the onset or progression of NCD for the Hong Kong populations. Drawing together the strengths each stakeholder to a pooled knowledge and also skills from various relevant stake holders in the society will ensure that each aspect of the society is represented adequately and prevailing gaps are adequately addressed. The determinants of health are very pervasive such that health promotion and prevention of disease will require involvement of the community in all sectors and all realms of environment including education and work place. Partnership is the most effective strategy of working with people from diverse backgrounds, tradition, values and beliefs. This is because collaboration maximizes the strengths and weaknesses prevailing in the healthcare with the aim of attaining the overall objective which is establishing a healthy nation.
References
Cheng, V., Tai, J., Wong, Z., Chen, J., Pan, K., & Hai, Y. et al. (2013). Transmission of methicillin-resistant staphylococcus aureus in the long term care facilities in Hong Kong. BMC Infect Dis, 13(1), 205. doi:10.1186/1471-2334-13-205
HUI, E. (2010). Perceptions of ethical practices in Hong Kong public hospitals: inter- and intra-professional similarities and differences. Journal Of Nursing Management, 18(6), 746-756. doi:10.1111/j.1365-2834.2010.01102.x
Huque, A. (2013). Can Public Management Contribute to Governance in Developing Countries?. Public Organization Review, 13(4), 397-409. doi:10.1007/s11115-013-0259-2
Kung, K., Wong, C., Wong, S., Lam, A., Chan, C., Griffiths, S., & Butler, C. (2014). Patient presentation and physician management of upper respiratory tract infections: a retrospective review of over 5 million primary clinic consultations in Hong Kong. BMC Family Practice, 15(1), 95. doi:10.1186/1471-2296-15-95
Lam, W., Lui, P. L & Wong, W. (2012). Contemporary Hong Kong government and politics. Hong Kong: Hong Kong University Press.
LEUNG, R., CHUNG, K., LI, V., CHEUNG, R., LAM, C., & ZIEA, E. (2015). Development of Electronic Health Record for Chinese Medicine eHR(CM) Sharing System in Hong Kong. Integrative Medicine Research, 4(1), 115. doi:10.1016/j.imr.2015.04.205
Liu, S., & Yeung, P. (2013). Measuring fragmentation of ambulatory care in a tripartite healthcare system. BMC Health Services Research, 13(1), 176. doi:10.1186/1472-6963-13-176
Mercer, S., Siu, J., Hillier, S., Lam, C., Lo, Y., Lam, T., & Griffiths, S. (2010). A qualitative study of the views of patients with long-term conditions on family doctors in Hong Kong. BMC Family Practice, 11(1), 46. doi:10.1186/1471-2296-11-46
Owolabi, O., Zhang, Z., Wei, X., Yang, N., Li, H., & Wong, S. et al. (2013). Patients’ socioeconomic status and their evaluations of primary care in Hong Kong. BMC Health Services Research, 13(1), 487. doi:10.1186/1472-6963-13-487
Rashed, A., Wilton, L., Lo, C., Kwong, B., Leung, S., & Wong, I. (2014). Epidemiology and potential risk factors of drug-related problems in Hong Kong paediatric wards. British Journal Of Clinical Pharmacology, 77(5), 873-879. doi:10.1111/bcp.12270
So, W., Chan, C., Choi, K., & Chan, D. (2012). Perspectives on the use of and service needs of cancer preventive services for ethnic minorities in Hong Kong: a study protocol. J Adv Nurs, 69(9), 2116-2122. doi:10.1111/jan.12067
Wong, E., Coulter, A., Hewitson, P., Cheung, A., Yam, C., & Lui, S. et al. (2015). Patient Experience and Satisfaction with Inpatient Service: Development of Short Form Survey Instrument Measuring the Core Aspect of Inpatient Experience. Plos ONE, 10(4), e0122299. doi:10.1371/journal.pone.0122299
Wong, F., Chan, F., You, J., Wong, E., & Yeoh, E. (2011). Patient self-management and pharmacist-led patient self-management in Hong Kong: A focus group study from different healthcare professionals’ perspectives. BMC Health Services Research, 11(1), 121. doi:10.1186/1472-6963-11-121
Wong, J., Cheung, E., Cheung, V., Cheung, C., Chan, M., & Chua, S. et al. (2004). Psychological responses to the SARS outbreak in healthcare students in Hong Kong. Med Teach, 26(7), 657-659. https://www.doi:10.1080/01421590400006572
Yam, C., Liu, S., Huang, O., Yeoh, E. K & Griffiths, S. M. (2011). Can vouchers make a difference to the use of private primary care services by older people? Experience from the health care reform program in Hong Kong. BMC Health Services Research, 11, 255.
We can write this or a similar paper for you! Simply fill the order form!
Acting as supervisor for a company of your choice, draft two examples of formal company e-mails to employees.
The first email will be good-news message delivering information that your employees will likely view as positive.
The second email will be a bad-news email delivering information that your employees will likely view as negative.
Each email will be approximately two-three concise, professionally-written paragraphs in an appropriate tone. Post both emails in the same document.
SAMPLE ANSWER
Business communication in nursing emails
Bad Email
Dear employees,
Our company’s turnover rate for the last financial year is reported to be unexpectedly low. Consequently, the company is experiencing financial downside and this call for a contingency plan to reduce the operation costs. For this reason, the management has agreed to reduce the number of employees.
We have strived to the best of our abilities to avoid this approach but there is no other alternative to stabilize the financial crisis. We regret to inform you that we have to terminate some positions held by new employees, interns and freshers.
We are sincerely grateful for your diligence and commitment towards achieving the company goal. We assure you that this move is only a temporary measure and when the situation stabilizes, we may consider hiring you back. The company will give you some bonus as a measure of our gratitude.
Yours Sincerely,
HR
Good Email
Dear employees,
Kindly accept our warmest gratitude for your hard work and marvelous contributions to the organization. We value the much time and energy dedicated towards achieving the organization goals and mission. It is a great pleasure to know that we can always account on you as we strive to climb even higher.
The company management was delighted to learn that our company was voted among the best performing company in the world. We understand that this was not easy, and that it is your willingness strives above and beyond.
For this reason, the management has decided that every employee shall have a pay raise of 13% of their current salary. The employees will also have increase in major allowances including house allowance, medical allowance and transport.
Yours Sincerely,
HR
We can write this or a similar paper for you! Simply fill the order form!
my group is Crown Resort Ltd, group work is prepare 3 presentation about Crown Resort Ltd background, Corporate Social Responsibility and Internal and External Environments.
Essay requires you to write about your/the group work stages based on the reading i.e. forming (what your group did in the forming stages; storming etc) and how this links to the tuckman reading. You must begin with an introduction i.e. the group work approach by tuckman can be found in our own Crown Resort Ltd group. Each stage should be a heading under which you should write about it.
Then the conclusion is basically what you think about tuckmans model – did it work for your group or not. You must read the articles provided in the question outline to know how to effectively complete the assignment correctly.
SAMPLE ANSWER
Tuckman’s Framework
Working in groups has never being an easy experience because of the different views from group members. Therefore, when creating a group it is very important to ensure that the group has fewer members because huge groups tend to have many misunderstandings. Effective groups make work easier, each member’s opinion is considered, work is done on time and a lot of information and ideas is available for the task. Groups help people to gain good communication skills, improve on their leadership and teamwork skills. Cooperation and communication between teams is very important because group members are able to arrange and discuss on how to handle the task assigned to them. Working in a team also requires proper time management, communication and working together. Issues of ignoring some member’s opinion cause conflicts between them which is not healthy for the work to be done (Wlodarczyk, 2011, pg 50).
In our group, it was not that easy for us to form the group. We had to choose members who are active though it was not that easy because the activity was an outside one. We required members who will work together more effectively and efficiently. We wanted to form a team with common goals, and who will make it possible for us to finish the task on time. It was not easy for us to know which person to choose as our leader because we were not that familiar with one another. Identification of each individual’s role was not also that easy because we were not aware of each group member’s ability. Though this stage was quite challenging we managed to form the group (Corey, Corey, & Haynes, 2014 pg 13).
In our storming stage, we experienced a lot of disagreements between ourselves and sometimes we couldn’t agree on anything at all. This was greatly affecting our work progress. In this stage, everyone wanted to prove that they were fit for some roles and there was too much competition on who was to become the group leader and who was to do a certain role. At this stage, we almost felt like doing away with the group because some members did feel comfortable with the tasks we had assigned to them. At the end, we came up with problem solving solutions and we used them to solve the disagreements between members (Wlodarczyk, 2011, pg 63).
Finally, our group was now established everyone was aware what roles he/she was to play in accomplishing the task and ready to work together. We established process of decision-making and we experienced fewer conflicts in this stage. At the end of our norming stage we were closer with one another and we almost had a brand for our group. In our performing stage, our group had common goals of achieving the task and everything was being done as we had planned. Work was easier and conflicts were no more. At this stage any challenges which occurred were being handled by the whole group. There was more teamwork compared to the other stages (Owen, Brooks, & Grunwald, 2013, para 5). Our adjourning stage was not that easy because we had become friends with one another and we had become of great influence to each other’s life actually the group at this stage felt more of a family. A lot can be done in teams compared to when done individually. Also, have learned that conflicts will always be present in groups what is important is how they are handled. It is very important to be part of an active group this is because active groups act as a motivation to group members. This is because active groups accomplish their tasks on time and they have proper time management and are goal oriented.
Reference list
Corey G, Corey S.M, & Haynes R. 2014. Groups in action: evolution and challenges. New York. Cengange Learning.