Combine all elements completed in previous weeks (Topics 1-4) into one cohesive evidence-based proposal and share the proposal with a leader in your organization. (Appropriate individuals include unit managers, department directors, clinical supervisors, charge nurses, and clinical educators.)
For information on how to complete the assignment, refer to “Writing Guidelines” and “Exemplar of Evidence-Based Practice.”
Include a title page, abstract, problem statement, conclusion, reference section, and appendices (if tables, graphs, surveys, diagrams, etc. are created from tools required in Topic 4).
Prepare this assignment according to the APA guidelines found in the APA Style Guide, located in the Student Success Center.
This assignment uses a grading rubric. Instructors will be using the rubric to grade the assignment; therefore, students should review the rubric prior to beginning the assignment to become familiar with the assignment criteria and expectations for successful completion of the assignment.
You are required to submit this assignment to Turnitin. Refer to the directions in the Student Success Center. Only Word documents can be submitted to Turnitin.
SAMPLE ANSWER
Antibiotic Resistance in Treatment of UTIs
Abstract
Infections of the urinary tract are among the most prevalent infectious diseases that are also accompanied by a substantial financial burden on the patient and the entire healthcare system (Grabe et al., 2008). Urinary Tract Infections (UTIs) range from these affecting the urinary bladder to those affecting the kidneys. The infections are classified according to the site of infection. These include urethritis (urethra), vaginitis (vagina), pyelonephritis (upper urinary tract), and cystitis (urinary bladder) (Mazulli, 2012). Different pathogenic microbes can be attributed to the condition. These include bacteria from the staphylococcus species such as Staphylococcus saprophyticus, the Klebsiella species, Pseudomonas aeruginosa, enterococci bacteria and also from the yeast fungi which is common among women (Mazulli, 2012). However, the main causative agent in the community and hospitals is the bacterium Escherichia coli (E.coli) that is a normal flora in the bowel and accounts for approximately 75 – 95% of UTI cases (A.D.A.M Inc, 1997-2008). Antibiotics are commonly used in the prevention and treatment of UTIs. However, this frequent use of antibiotics has resulted into the development of antibiotic resistance and vaginal and intestinal dysbiosis. This has become problematic in the treatment of UTIs and this paper, therefore, provides evidence of the spread of antibiotic resistance in UTI treatment.
Problem Statement
The treatment and prevention of UTIs has most of the time involved the use of antibiotics as the first-line treatment. This often follows the isolation and culture of the etiological agent to select the appropriate antibiotic for use. However, today there is increasing resistance to most of the antimicrobial agents prescribed for the treatment of UTIs in both community and hospitals settings. This is spreading to even the most potent antimicrobial agents hence the need to establish alternative approaches for treatment.
For example, a study was conducted in India and was aimed at reporting the resistance pattern among the most common uropathogens that were isolated in a tertiary care hospital setting. The focus of this study was on resistance to ciprofloxacin (Mandal, Acharya, Buddhapriya, & Parija, 2010). Nineteen thousand and fifty samples were collected, cultured and the pathogenic microbes isolated. The susceptibility to antibiotic tests were done using the Kirby-Bauer disk diffusion method after noting the clinical and demographic characteristics of each patient. E.coli was isolated and out of the total samples selected 62% were sterile while 26.01% had significant growth (Mandal, Acharya, Buddhapriya, & Parija, 2010).
In addition, 2.3% had insignificant growth, and 9.6% of the samples were contaminated. The ciprofloxacin-resistant E.coli had a strong association with gynecological surgery among the female participants, UTI in adulthood, prior antibiotic use, and uropathy among men and complicated UTI among women (Mandal, Acharya, Buddhapriya, & Parija, 2010). The continuous of ciprofloxacin was, therefore, linked to the development of resistance in males, females, and in-patients. This indicates the need to rationalize the use of antibiotic treatment or most importantly develop alternative approaches.
Trimethoprim and Sulfamethoxazole are often used as a first-line treatment for UTIs. However, there is increasing resistance towards the drug that is resulting to a significant decrease in its use. This antibiotic is an inhibitor of the bacterial folate synthesis that is needed for the synthesis of thymidine hence the synthesis of DNA (Hilbert, 2011). These drugs are administered in a combined ratio of 1:5 (SXT) and the guidelines indicate that it should be avoided where the resistance reaches between 15% – 20% (Gupta et al., 2011).
The North American Urinary Tract Infection Collaborative Alliance (NAUTICA) conducted a study to analyze the development of resistance towards SXT. They used 1,142 Uropathogenic Escherichia coli UPEC isolates from 40 medical centers. The results revealed that 21% of the participants had resistant isolates (Hilbert, 2011). In another study conducted by the Arkansas River Education Service Cooperative (ARESC), a similar result was found and in this case the resistance was higher at 29%. Trimethoprim and Sulfamethoxazole inhibit the enzymes dihydrate folate reductase and dihydropteroate synthetase respectively. The resistance to the drug is mediated by gene transfer of the genes that are responsible for encoding the resistant enzymes (Hilbert, 2011). In a study conducted using 305 UPEC isolates revealed that 66% had encoded a dfr allele that encoded a trimethoprim-resistant dihydtrate folate reductase and 96% had a sul gene encoding for the sulfamethoxazole-resistant dihydropteroate synthetase (Hilbert, 2011). These genes appeared due to the continuous use of SXT, and their presence facilitate the spread of resistance elements among the bacterial population hence the increased resistance.
Finally, there is also the development of resistance to other aetiological agents for UTIs. For example, the Klebsiella species (K. pneumoniae) accounts for approximately 1-6% of the uncomplicated cases of UTIs (Schito et al., 2009). The bacterium is resistant to penicillin and nitrofurantion intrinsically and shows resistance to other common antibiotics used for the treatment of UTIs. Per Schito et al. (2009), a study conducted to establish the resistance of K.pneumoniae indicated 23% resistance to SXT, 21% to cefuroxime, 12% fosfomycin and 6% ciprofloxacin (Schito et al., 2009).
An earlier study by Kahlmeter in 2003 revealed similar results. In the two studies mentioned, the 94-99% of the isolates showed susceptibility to ciprofloxacin and 91-96% were susceptible to amoxicillin-clavulanic acid. However, due to the continuous use of the drugs today, there is increasing resistance (Hilbert, 2011). Moreover, K. pneumoniae accounts for 8-11% 0f catheter-associated UTIs (CAUTIs) within the hospital setting (nosocomial infections). In the above studies, 17-21% of isolates from individuals with CAUTIs were resistant to an extended spectrum of cephalosporins while 10% were resistant to carbapenems (Hilbert, 2011). This indicates the growing resistance of UTIs etiological agents to antibiotics and the need for new treatment approaches.
Conclusion
UTIs are among the most common forms infections today. Moreover, their prevalence is also on the rise including among men. Antibiotics have been for a long time the first line of treatment for infectious diseases. Treatment involves the isolation and culturing of isolates to identify the main causative agent. The common cause of UTIs is the bacteria E.coli; however, there are other species of bacteria that can also cause the disease. In the past, antibiotics were effective for UTI treatment, but due to the continuous use of the antibacterial drugs the bacteria are increasingly developing resistance. The resistance is developing as a result of mutations and other processes. The resistance is continuously increasing from the “weaker” forms of antibiotics to even those that were initially thought to be the most efficacious including the development of multiple resistance. Due to the increasing prevalence of UTIs and the resultant rise in resistance to antibiotics, it is imperative that alternative approaches of treatment should be employed.
References
A.D.A.M Inc. (1997-2008). Urinary Tract Infection. 1-4.
Grabe, M., Bishop, M. C., Bjerklund-Johansen, T. E., Botto, H., Çek, M., Lobel, B., et al. (2008). Guidelines on the management of urinary and male genital tract infections. European Association of Urology.
Gupta, K., Hooton, T. M., Naber, K. G., Wullt, B., Colgan, R., Miller, L. G., et al. (2011). International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis, 52, e103-120.
Hilbert, D. W. (2011). Antibiotic resistance in urinary tract infections: Current issues and future solutions. In P. Tenke (Ed.), Urinary tract infections (pp. 194-206). InTech.
Mandal, J., Acharya, N. S., Buddhapriya, D., & Parija, S. C. (2010). Antibiotic resistance pattern among common bacterial uropathogens with a special reference to ciprofloxacin resistant Escherichia coli. Indian J Med Res, 136, 842-849.
Mazulli, T. (2012). Diagnosis and Management of Simple and Complicated Urinary Tract Infections (UTIs). Can J Urol., 19 (Suppl 1), 42-48.
Schito, G. C., Naber, K. G., Botto, H., Palou, J., Mazzei, T., Gualco, L., et al. (2009). The ARESC study: an international survey on the antimicrobial resistance of pathogens involved in uncomplicated urinary tract infections. Int J Antimicrob Agents, 32, 407 -413.
We can write this or a similar paper for you! Simply fill the order form!
Select one of the following ethical issues in healthcare:
Foregoing curative medical treatment due to religious beliefs
Use the CSU Global Library and select Internet sources to conduct research on your chosen topic. Based on your research, provide the history of the issue from a legal, ethical, and moral perspective. In your paper address the following questions:
Do the consequences of actions always direct what is morally required?
What should happen when two principles come into conflict? For example, should patient autonomy be considered more important than beneficence? Defend your position.
Are moral and ethically rules always binding, or are they only guidelines to be assessed in each case? Defend your position.
Your paper should be 10-12 pages in length, well-written, and formatted per CSU-Global specifications for APA Style. Support your analysis by referencing and citing at least six (6) credible, peer-reviewed sources other than the course textbook (Ethics in Health Administration: A Practical Approach for Decision Makers, 2nd ed, by Eileen E. Morrison).
SAMPLE ANSWER
Foregoing Curative Medical Treatment Due to Religious Beliefs
Introduction
Healthcare professionals frequently find themselves in dilemmas as they undertake their chores at the workplace, with some directly confronting the ethical issues while others turning away. Usually, the moral courage that one possesses is what matters most as it, more often than not, helps the practitioners in addressing the various ethical issues that may present themselves; which could even involve doing something otherwise considered wrong. Inasmuch as there usually are predetermined courses of action considered ethically moral or otherwise, the consequences of the course of the action taken is what really matters (Stewart, Adams, Stewart, & Nelson, 2013). Because of this, an action that is otherwise not acceptable may have to be carried out in order to get to achieve a desirable consequence; for instance, according to most religious doctrines, abortion is not acceptable, even the conscience of the individual that may be involved may not allow it. However, if done for the sake of good will remains morally binding, for instance, the case of complications in pregnancy.
In order for us to get to understand the implications of the ethical issues pertinent with the health care practice, there is the need to understand the definition of nursing by the International Council of Nurses (ICN). Under it, the profession is defined as: “Nursing encompasses autonomous and collaborative care and communities of all ages, groups, families and communities, sick or well and in all settings. Nursing includes the promotion of health, prevention f illness and the care of ill, disabled, and the dying people. Advocacy, promotion of safe environment, research, participation in shaping the health policy and in patient and health systems management, and education are also key nursing roles.” (ICN, 2011). As outlined by Morrison (2011), the definition incorporates the three fundamental components of bioethics. It is, thus, conceivable to say that the health practitioners have the obligation of developing a well-founded ground of ethical understanding with regards to the protection of the people; which is their sole duty.
Moral Courage
The ability of one to make the right decisions in such situations that involve moral and ethical issues is what is called moral courage. According to Day (2007), moral courage is “a trait displayed by individuals, who, despite adversity and personal risks, decide to act upon their ethical values to help others during difficult ethical dilemmas. As Hall (2014) asserts, such individuals tend to strive to see to it that the only do what is right, even in cases whereby most are expected to choose least ethical behavior, which could even be not taking any action.
Conflict of Principles
Religious, spiritual and cultural beliefs and practices remain very crucial in the lives of most patients, yet most health practitioners usually find themselves at the dilemma of whether to, how and when to address such issues when dealing with patients. In the past, the physicians were basically trained on the various ways of diagnosing and treating the various diseases, but with very little or no training on the spiritual approach to the ordeal. Besides, the professional ethics allows the professionals no chance of impinging their personal beliefs on their patients who are usually very vulnerable (Brierley, Linthicum, & Petros, 2013). The matter is even complicated further by the characteristic nature of most nations of religious pluralism, having a wide range of systems of beliefs: agnosticism, atheism to the very many religious assortments. Because of this, it tends to be very difficult getting to fully understand the religious beliefs of all the patients from all walks of life.
The very first temptation that would prove worthwhile in this case is for the professionals to fully avoid the doctor patient interactions with respect to their spiritual or religious beliefs. This simplest solution may never be the best as several studies have shown that the spiritual and cultural beliefs f various patients have been proved to be very important factors for the patients to be in a position of coping with relatively serious illnesses (McCormick et al, 2012). McCormick et al (2012), assert that the engagement of the spiritual beliefs of the patients in their healing process may be devised by the health practitioners through comparison of their own beliefs against those of the patients.
Case Scenario: Foregoing Curative Drugs due to Religious Beliefs
In some communities, there is too much belief in the traditional practices that accepting the modern medicines becomes very difficult. Such communities have a belief system in which they believe and may recognize the move towards accepting the western medicine as evil. In such a case, the patient may never be taken to the hospital, or worse still, after getting to the hospital refuse to take the prescribed medicine on the belief that it is against the doctrines of their religion. The most common cases, include, but not limited to; blood transfusion, abortion, taking of family planning pills and even the normal tablets.
Conflict in Principles
In case of the principles coming into conflict, there usually is the need to be very flexible as there are so many ways in which the situations may present themselves. For effective resolution of such conflicts, the ethical and professional principles, rather than the personal preconceived ideas, should always form the pillar for the effective decision making when it comes to ethics (ANA, 2011). The ethical behavior of nurses is usually guided by a set of principles contained in the American Nurses Association (ANA) Code of Ethics of Nurses (2001). It is expected of all the nurses that they uphold all the principles in the course of their practice of professional nursing, while, at the same time, the Cord of Ethics for Nurses encourages them to ensure consistency with their personal values. There is also emphasis on the need to hold open discussion with regards to conflicting ethical principles in such a manner that all the principles are placed at the same level and treated equally.
Autonomy versus Beneficence
Autonomy
Autonomy refers to the personal self-rule that is both free from controlling such interferences that may result from others and the personal imitations that my put meaningful choices at jeopardy. In the health care, autonomy forms one of the key guidelines for the clinical ethics. A point that must be noted is that when speaking of autonomy, it does not merely imply leaving the patients the freedom of making their own choices. Rather, the health practitioners are under an obligation to see to it that they create the conditions that provide room for the independent choices, thought under some guidance. The respects for autonomy scenarios include giving room for autonomous choices as well as respecting the right to self-determination of an individual.
It must be noted that the doctors are usually visited by the people because they may not be equipped with the necessary information or background necessary for the making of informed choices. Hence, it is the physicians that educate the patients in order for them to adequately understand the situations, including; addressing the fears and emotions that may interfere with the decision making ability of the patients. Confidentiality is another form of autonomy very crucial in administering the treatment to the patients.
Beneficence
Usually, this is an action done purely for the benefit of others through either removing harm or simply by improving their situations. Apart from being refrained from causing harm, the health practitioners are expected to see to it that they help the patients. Due to the nature of the relationship inherent between the patients and the physicians, the doctors have the obligation removing or preventing harm and balancing and weighing the possible risks against the possible benefits of any action.
Balancing of autonomy and beneficence
Amongst the most difficult and common ethical issues to tackle comes in when the patient’s autonomous decision comes into conflict with the beneficent duty of the physician, which is mainly looking after the best interest of the patient. For instance, a patient who has very strict religious background may refuse to take medicine, simply because they believe in spiritual healing. This may be so challenging, especially when the physician has successfully diagnosed the ailment and knows its cause well, hence, its prescription (ANA, 2011). At such a point, the physician may be under the challenge of whether to maintain the autonomy of the patient or take a beneficence action, which will violate the autonomous requirement of the patient. More often than not, the two are equally important, however, beneficence comes first as it is a matter of life and death.
Basically, the modern biomedical ethics are grounded on four principles, which balance categorical Imperative of Emmanuel Kant: you must always do the right thing no matter what it takes, and Utilitarianism of John Stuart Mill and Jeremy: make the best decision for everyone all around. When in combination, the principles are usually called Principalism.
Respect for autonomy: giving priority to the informed choices of the patient. This theory asserts that the practitioners need to see to it that the wishes of the patients are taken into consideration. As such, the wish by a patient to have a kind of special attention with regards to choice of the health care services administered should solely depend on the patient’s wish.
Non-malfeasance: do no harm
Beneficence: do what is best for the patient, regardless of their consent. This principle asserts that the consent of the patient may be overlooked in order to see to it that the course of action is for their own good. With this, the health care practitioners are expected to ensure the good of the patients even if it means doing what they don’t wish for. The ultimate consideration of the morality will lie in the consequences, and at times, even if a patient requested for the end not to have blood transfusion due to religious beliefs, they may eventually end up thanking the physician, rather than suing them (Morrison, 2011).
Justice: always balancing the social and individual costs, risks and benefits. The physician has the obligation of seeing to it that they properly advise the patients with respect to the possible risks involved to ensure they are well informed before getting to a medical ordeal.
Morals and Ethics
Most of the moral dilemmas that tend to arise in medicine are usually analyzed using the four aforementioned principles but with some consideration given to the resultant consequences, though the frameworks may have limitations. The judgment of the best consequences is not always clear, and din case the principles conflict, the ease of deciding on the best dominant is always very hard. Virtue ethics usually focuses on the nature of the moral agent rather than how right the course of action taken is. Usually, as a practitioner, the ethical principles, which guide what action to be taken do not usually take into account the moral agent’s nature (Cordella, 2012). To look into how binding the morals usually are, the “standard” Jehovah’s Witness case may be used.
A very competent adult believer loses too much blood due to bleeding in a vessel in an acute duodenal ulcer, and the only best chances of saving his life is by having a blood transfusion together with some operation done on him. In exercising his autonomous decision, the patient requests for surgery and treatment with the best non-blood products available, and refuses blood transfusion. He even accepts the risks that are pertinent with surgery without blood transfusion.
It is very important for the health practitioners to get to distinguish between morality and legally binding courses of actions as an action may be legal but not moral and vice versa. For instance, the resuscitation of a dying patient may be considered legal, but not moral. On the other hand, when a patient falls too sick at home, it may be moral to over speed to the hospital but illegal. Also, the physicians have the obligation of distinguishing between religion and morality. From instance, some of the religions believe in circumcising women while others recognize it as a sin.
Moral Frameworks
However, the moral theories tend to provide different frameworks upon which the nurses may be able to get clarification as well as view the patients’ disturbing situations. Widely used and applicable are three frameworks that may guide the physicians. The three basic broad categories of the moral frameworks are: virtue theory, deontological and utilitarianism theory.
Virtue theory
This theory exclusively probes the human morality. It gives very little attention to the regulations that people need to adhere to; rather, it puts more emphasis on what is deemed necessary in development of human characteristics considered as good, just like living a generous and kind life.
Deontological ethics
These are usually associated with the ethical and moral standards in the execution of the professional duties by the health professionals.
Utilitarianism theory
This is the belief that any form of action is considered as being right as long as it leads to the greatest good for larger number of people. As such, there usually is a calculation on the outcome of any particular action. As such, if a health practitioner considers an action as having high propensity of bringing good and happiness to larger number of people; it definitely is the right thing to do (Morrison, 2011). In other words, the utilitarianism tends to base its reasoning on the usefulness of the action that may make it be considered as moral or immoral; for the course of action to be considered as moral, the good outcomes have t outweigh the bad ones.
Moral principles
They are the broad and general statements of philosophical concepts that provide the foundations upon which the moral rules are founded.
The health practices usually come with too many challenges which leave the practitioners at a dilemma in more often situations than not. For instance; the debate n abortion, organ transplant, end-of-life issues, management of personal health information and the allocation of the scarce health resources. Looking into each of the aforementioned issues, it usually leaves the platform very open for the practitioner to decide what they deem right course of action to take. As put across by Elliot (2011), “Culture provides the rules or framework that guides us as we negotiate our way through our daily activities of life.” Through the assessment of the heritage of any particular patient helps the nurses to understand well how such a person relates to their surroundings, how they view health and wellness, their various ways of gaining and applying knowledge as well as any other area that may be of interest in health care provision.
Most of the nations of the world, for instance, in America, the populations are characterized by people of vast diversification in the religious, ethnic, sexual orientation and nationality. As such, the patients that visit the health centers present with themselves varied symptoms requiring medical attention, some based on illness while others grounded on the cultural and religious backgrounds of the patients.
As the patients are guided through any healthcare facilities of the dialysis unit, it is very recommended that the practitioners not only concentrate on the clinical needs, but also see to it that they identify the patient’s demographics and religious orientations amongst others. The problem very common is the avoidance of the common mistakes that greatly impact safety and quality and instead, pay too much attention on the nature of the illness and how the patient may be treated. In doing this, they are not really identifying with the patient in order to attend to them as an individual. A point that must be noted is that all patients have diversified characteristics and needs, both the clinical and non-clinical, which affects the manner in which they participate, receive and view their treatment (Morrison, 2011).
Unlike in the past when health provision was mainly limited to a particular community, mostly, where one came from, there have increasingly arisen changes due to the cultural and religious diversity. There is need for the healthcare providers to see to it that they are well conversed with all the possible cultural and religious traditions inherent in the societies within which they work. It is based on this challenge that the terminology ‘cultural competence’ came to be, whereby all the practitioners are expected to be able to work in the various cultural and geographical regions without much trouble (Cordella, 2012). This may only be so through getting to first and foremost understand the various cultures to help learn their beliefs.
A fact that all health care practitioners must come to terms with is the diversity in the religious beliefs inherent in the various cultures and people from different walks of life. The beliefs of the various patients tend to be aligned to their religious backgrounds, which may never be easy to change. Due to this, it is in order that all the professionals fully understand the possible challenges that they may expect, however, they should never let the various beliefs by such patients waver their conscious mind of making the right decisions to do good. Once a person believes in the consequence o the course f action they are about to take, they should do so without any fear.
Conclusion
In conclusion, we as health practitioners are faced everyday with caring for patients of different faiths, cultures and religions. It is important to always keep an open mind and allow yourself to try to understand the faith that our patients believe. Understanding other cultures and beliefs are critical in the healing process. In healthcare today as physicians, we need to keep an open and unbiased mind, treating everyone as equal. Through the development of proper cultural competence, we may help our patients by accepting their beliefs without abandoning our own personal customs. As health practitioners, we may not be able to change the beliefs of the various patients from the different walks of life as the populations continually get diversified, rather, there is need to remain open minded in order to accommodate the diverse beliefs. In addition, as long as we believe that the course of action that we are taking will lead to more good than bad, then the autonomous stake of the patients should always be put at stake. After all, they will eventually appreciate the results.
Brierley, J., Linthicum, J., &Petros, A. (2013). Should religious beliefs be allowed to stonewall a secular approach to withdrawing and withholding treatment in children?. Journal of Medical Ethics, (9). 573. doi:10.1136/medethics-2011-100104.
Conflicts between religious or spiritual beliefs and pediatric care: informed refusal, exemptions, and public funding.(2013). Pediatrics, (5), 962.
Cordella, M. (2012).Negotiating Religious Beliefs in a Medical Setting. Journal Of Religion & Health, 51(3), 837-853.
Elliot G. (2011). Cracking the cultural competency code. Canadian Nursing Home, 22(1), 27-30.
Hall, H. (2014). Faith healing: religious freedom vs. child protection: the medical ethics principle of autonomy justifies letting competent adults reject lifesaving medical care for themselves because of their religious beliefs, but it does not extend to rejecting medical care for children. Skeptical Inquirer, (4). 42.
International council of nurses, (ICN). (2011). Nursing and health professions. 2011.
Krohn E. (2013). Recovering health through Cultural Traditions. Forth World Journal, 12.
Lamparello, A. (2001). Taking God Out of the Hospital: Requiring Parents to Seek Medical Care For Their Children Regardless of Religious Belief. Texas Forum On Civil Liberties & Civil Rights, 647.
Morrison, E. E. (2011). Ethics in health administration : a practical approach for decision makers / Eileen E. Morrison. Sudbury, Mass. : Jones and Bartlett Publishers, c2011.
Stewart, W., Adams, M., Stewart, J., & Nelson, L. (2013).Review of Clinical Medicine and Religious Practice. Journal Of Religion & Health, 52(1), 91-106.
We can write this or a similar paper for you! Simply fill the order form!
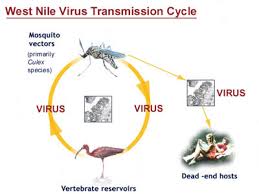
For the month of August, 12 new cases of tuberculosis and 12 new cases of West Nile virus infection were reported to a county health department. You are not sure if either group of cases is a cluster or an outbreak.
What additional information might be helpful in making this determination? Why? How would you obtain this information?
SAMPLE ANSWER
Week 4 discussion
Quick response is vital in case of any outbreak of diseases. Health departments and other agencies have the duty to act swiftly to contain these clusters or outbreaks. For instance, in this case where a country’s health department reported 12 new cases of tuberculosis and West Nile virus infections, it becomes critical to collect information quickly to determine whether it is a cluster or an outbreak for immediate action. The author deliberates on additional information required to make determination as well as reasons why and the process of obtaining information in such instances as tuberculosis and West Nile virus outbreaks.
To determine whether these cases are a cluster or an outbreak, it requires adequate information. Information pertaining to these cases will include the rate of occurrence of the diseases, the community or region affected and the frequency of the illness among many others. Outbreak occurs when the number of victims is more than the expected cases (Sterhr-Green, Paul, Voetsch & MacDonald, 2010).
This information is required because it helps to determine the number of people that are affected and in adopting appropriate strategies to counter the same (CIFOR, 2010). A cluster and an outbreak requires different strategies to contain further spread of the disease and therefore being armed with this vital information is essential to approaching the challenge amicably.
Obtaining this information is yet another important aspect in seeking to determine whether the case above is a cluster or an outbreak. One way of obtaining information is partnering with the health agency to come up with appropriate ways to get information on the ground (UIC, 2005). It is also important to partner with the community members and other leaders to help in establishing the causes and the time of the outbreak among other information. Information will also be obtained through interviews and administration of questionnaires with the victims and their close family members.
Every bit of information must be cited
must also write a treatment plan with 2 long term goals and 2 short term goals for each of the long term goals and 2 interventions for each short term goal.
USE PEER REVIEWED SOURCES AND SCHOLARLY SOURCES FOR ACCURATE INFORMATION AND WELL RESEARCHED ASSIGNMENTS FOR VALIDITY.
Review the grading rubric on turntin to avoid penalization which will lead to low grades.
We can write this or a similar paper for you! Simply fill the order form!
HPI
A 40-year-old Asian American male, who works as a roofer, complains that three days ago he was lifting a heavy object at work, following which he got low back pain. The pain is in the middle of the back near his waist. The pain increases when he bends forward and he is experiencing numbness and tingling in the toes of his right foot. He has had similar symptoms before, but it has not been so bad in the past. This is the worst he has had because in the earlier instances, he has never had the tingling sensation in his right foot before.
In the past, he got better with rest and some Ibuprofen. He is worried that he will not be able to continue his work and make money. He is out of work as a result of the pain. He has a lot of difficulty getting sleep at night. He has started taking some of his friend’s medication and it seems to help.
He has pain in the mid lumbar area, which radiates to the right buttock. He also has numbness and tingling down the back of his right thigh to his toes. The pain and numbness has been increasing since the problem started three days ago. He has tried over-the-counter Ibuprofen and some stretching exercises, but it does not seem to help. He has not sought any medical care yet. In the past, the pain had just gone away, but this time the pain is persistent. There is a gradual worsening of his symptoms and he is concerned about the pain that has been increasing steadily over the past three days. He is wondering whether he has a herniated disc. His major concern is that he has no health insurance and will be missing work.
ROS
Pain in the mid lumbar area radiating to the right buttock. There is a tingling sensation that goes down the back of his right thigh to the toes. He does not have urinary or bowel incontinence. No nausea, vomiting, or fever. He denies abdominal pain and pain with urination. There is no gross hematuria.
MEDICATIONS
Patient does not take any prescription medications, only over-the-counter Ibuprofen. He is using 800mg of Ibuprofen every four hours. Patient is compliant with the prescribed regimen; in fact, he could be using too much. Patient is seeking care because of the increasing pain. He has tried chiropractic manipulations in the past for low back pain.
Common low back pain affects more than two thirds of people aging over 40 years. It a rampant problem in the society on the basis of its direct cost associated with health care as well as its socio-economic ramifications. Ten percent of the people with low back pains fear that the pain may evolve to become a chronic case. With reference to the case study of the 40 year old Asian American man, the cause of his musculoskeletal condition is thought to be caused by physical straining especially lifting heavy loads (Leg Numbness, Tingling Feet and Toes. (Dawson, n.d.).
From the signs and symptoms of the subject in the case study, it can be suspected that he is suffering from DDD. The herniating of the disc may occur suddenly or gradually, especially after lifting a heavy load from the ground. The disorder is the most prevalent cause of disability among the middle aged persons.
Pathophysiology
His suspicion that he has a herniated disc in the lumbar spine which is probably pressing the sciatic nerve is likely to be true. Herniation of the nucleus pulposus (HNP) come about when this nucleus breaks dissociates from the annulus fibrosus of an intervertebral disc which is the spinal shock absorber. This leads to degenerative disc disease (DDD).
Signs/symptoms
Pain is the most common disabling symptom in musculoskeletal disorders. The man in the case study has been forced to seek medical attention quite often as a result of the pain. The symptoms characterizing DDD have been manifested by the patient. These include pain, tingling in the lower back, calf or foot, thigh, typically affecting one side. The symptoms worsen when the patient is standing, sitting, lying down and some certain movements such as bending or, as in the case of the subject in the case study, lifting objects from the ground (Degenerative Disc Disease Progression over Time. (n.d.).
Progression trajectory,
The progress of lumbar degenerative disease is slow since it also starts as a benign, manifesting its symptoms in a slow rate. According to the case study, the pain tends to increase with time especially during some movements. It is predicted that if one starts experiencing several low back pains at the age of thirties, chances of being in a wheel chair when they reach sixties are high. Although there will be progression in the disc generation, it is not common for low back pain and related symptoms to progress (Disc Disease Progression over Time, n.d.).
Diagnostic testing
The diagnostic of DDD is done by achieved through carrying out various diagnostic studies. Some of the tests carried out include computed tomography, discography, radiographs and magnetic resonance. The discography is able to tell the source of pain experienced by the patient. These studies are, for instance, provocative discography, lumbar radiographs and magnetic resonance imaging. The patient history, physical examination together with these studies is useful in the diagnostic process although they are not in and of themselves ultimate procedures in the diagnosis of pain. The overall diagnosis is therefore determined by the clinical status of the patient and his response to the prescribed treatment (Hasz, 2012).
A reliable explanation on the cause of back pain experienced by patients is obtained through a diagnosis of degenerative disc disease. This is a usual practice during clinical practice.In Diagnosis of these patients is carried out to find evidence associated with degenerative changes. This is done by healthcare providers by use X-ray, Computed Tomography (CT) or MRI scans. The result obtained from the diagnostic tests provides an explanation for the cause of pain. The health care team use the diagnosis as the basis of decisions made on treatment models chosen. In some cases, procedures such as epidural steroid injections and spine surgeries are focused on modifying degenerative changes occurring in the spine. A common belief by most of the healthcare providers and patients is that these diagnostic tests involving MRI or CT scan make out the cause of pain or degenerative disc changes experienced in the spine (Degenerative Disc Disease., n.d.).
Treatment options
Treatment of degenerative disc disease is treated effectively by conservative care which also comprises of medication to manage pain and inflammation. This medication may be administered orally or intravenously through epidural injections. There are many surgery forms available today as a common form of treatment for DDD. The surgeries use different technologies which have to pass a test of time. Different cultures also have their own remedy on how to conservatively intervene against this disorder. However, exercise and physical therapy is cuts across all cultures and interventions. It is worth noting that there is no sure way of treating DDD hence this remains highly difficult and controversial (Alexandre, 2011).
Differentiate the Disorder from Normal Development
The normal intervertebral discs occur between the vertebral bodies which is important in linking the discs together. They form make up to one third of the spinal column in which they also form consist of its main joints. Normal discs play an important role in providing mechanical support through constantly transmitting loads arising from body activity as well as body weight through the spinal column. The spinal column is flexible due to these discs which allow torsion, bending and flexion. There thickness is approximately 7–10 mm thick and have a diameter of 4 cm. The thick outer ring making up the complex intervertebral discs structures are made of fibrous cartilage known as the annulus fibrosus, which also lines a more gelatinous core referred to as the nucleus pulposus. The cartilage end-plates sandwich the nucleus pulposus. With an increase in age and as one grows and there is skeletal maturation, the distinction between the annulus and nucleus decreases and the nucleus becomes less gel like and more fibrotic. The morphology of the disc changes becoming more disorganized
Physical and Psychological Demands on the Patient and Family
The man in the case study is said to be divorced hence he depends on himself through a job he gained through his high school certificate. Having been overwhelmed by challenges of marriage indicates that the patient must have contributed to many problems in the family probably mainly caused by his illnesses.
Key Concepts to Achieve Optimal Management and Outcomes
Optimal disorder management and outcomes with regards to care for the man suffering degenerative disc disease refers to concepts which will improve his wellness and control of problems and psychological factors closely associated with the specific physical conditions and disease. It is important to manage the patient’s cognitive and psychological factors in competence to enable him to manage his own affairs. Also, there is need to manage factors which will ensure motivation, productivity, leadership and healthy workplaces.
With patient-centered care, the family and their patient should be provided with relevant and adequate information which will enable them to manage the disorder ethically. Since it typically arises from the aging process hence it has a tendency to care become a chronic problem. This means that the patient should lead an active life, according to evidence based care, so as to manage their incapacity, whether short term or long term disability.
The Role of Interdisciplinary Team
There is no one person, due to his skills and knowledge can claim responsibility over the success of the team or provision of all care needed by the patient against a disorder such as DDD.Each of the individuals in a team handling the disorder shares a common although each contributes his common goal. The physicians, health care givers and family or friends join the collaborative care teams which align themselves around values and requirements of the patient. The collaborative team should agree on which regenerative therapies would be suitable to repair the degenerated disc or discs.
Facilitators and Strategies to Overcome Barriers
Some of the strategies acceptable by the American Nurses Association are aimed at overcoming self destructive tendencies and promoting patient centered care. In order to restore the patient to back to active life, identification of a proper form of treatment is necessary. The medical practitioners need to use the most appropriate diagnostic procedures before choosing the most preferred therapy for the patient. The patient in the case study has not sought for adequate medical intervention due to economic and social inadequacy.
Alternative ways are available to intervene in the patient’s case. Since he is divorced at the age of 40 years and already takes the blame, this may be a hindrance for his quick recovery. The team is encouraged to provide a lasting solution which is helpful in enabling the man to move on in life. For instance, exploring ways of carefully evaluating the patient’s psychosocial issues with an aim of providing professional counselling will improve the man’s better view of life. Identification of these psychosocial problems would make it easier to counter the factors which quicken the rate at which the disorder becomes chronic. The musculoskeletal disorder related pains will be controlled hence setting the patient toward healing process.
Section II
Plan of Care
According to basic science the disc is not entirely to blame for the pain the pain the patient may be experiencing. This gives the first hint on where the care plan should be directed since it indicates that annulus is not obviously compromised. The care plan considers both indications and diagnostics for either disc replacement or fusion in patients with DDD. However, research hold that the benefits of this process still do not outweigh risks.
How does patient’s socio-cultural background potentially impact the optimal management and outcomes of this plan of care?
From the patient history given, therapy needs to be coupled with a structured rehabilitation program that takes account of cognitive-behavioural therapy and exercise. Research should provide a guide or a framework on this can be done owing to the fact that the man is lonely.
Subjective Data and Objective Data
The patient’s subjective data entails the history taken from his background with regards to his sickness from degenerative disc disease. On the other hand, the objective data will include all other factors related to the effects of the patient’s sickness. These include his divorce, lack of health insurance and poor attention to medical therapy in relation to continuing with work. The issue of family dysfunction, social isolation and poor attention to proper health measures would comprise of objective data.
Assessment
From the history given the patient has not sought for proper medical attention since he only prefers over the counter Ibuprofen. Although he has tried chiropractic manipulation in the past, his problems could not end since this was not the best remedy for this.
Goals of care
·To change the patient’s attitude toward medical attention
·To ensure the patient commences appropriate medication immediately; involving diagnosis and prescription of the right drugs.
·To counsel the patient approach marriage on a better dimension so as to win his wife back.
·To give enable the patients adopt a better lifestyle of nutrition, exercise and work.
How does patient’s socio-cultural background potentially impact the optimal management and outcomes of this plan of care?
The social cultural background of the patient, which is engraved in his attitude to all the issues surrounding him, would make it difficult to implement this plan. However, with an enforced rehabilitation, the plan will work wonders. The negative perception of the patient toward the use of social amenities and services provided would make it a challenge for a successful disease management.
Plan of care
The plan of care for the patient and others like him is to be based on evidence based care. This involves paying serious attention to many aspects other aspects besides responding to patient symptoms and patient history alone. The identification of the right therapy should be ideal to comprehensively solve the problems the man’s seeking. This includes working in collaboration with close family members, employer and other medical experts (Belfer, 2013).
1.Diagnostic test:List, Include IC9 codes.
I.Physical examination
II.Computed Tomography (CT)
III.Provocative discography,
IV.Lumbar radiographs
V.Magnetic resonance imaging
2.Medications: Listnew or changes to dose and time. Make sure you write medication, dose, route and length of time to take if relevant.
vAcetaminophen (such as Tylenol)
vNSAIDs, or non-steroidal anti-inflammatorydrugs. These are:
1.Ibuprofen
2.Naproxen
3.COX-2 inhibitors
(Pain Medications for Degenerative Disc Disease Treatment. (n.d.).
3.Conservative treatments:This would be treatments such as ice, raise head of bed, weigh every day, etc.
Conservative treatment for degenerative disc disorder is based on the patient’s culture. The Asian American people treat DDD by tying a restrainer around the lower back to exert pressure on the part expected to have a lumbar curvature.
4.Education: The education plan for the patients such as the patient in the case study is the introduction social training on how to balance work, family, social life, nutrition and exercise.
5.Collaboration and/or referrals: To ensure the plan is implemented, the county health officer would be mandated to supervise the process. With this position, the officer is capable of influencing all departments and institutions in the country where the individual comes from.
6.Follow-up: The follow-up will comprise of the implementation tools. These include a copy of care plan, sample regimen for the disease and charts for illustration.
References
Alexandre, A., Masini, M., & Menchetti, P. M. (2011). Advances in minimally invasive surgery and therapy for spine and nerves. Wien: Springer.
Belfer, I. (2013). Nature and Nurture of Human Pain. Hindawi, 2013(-), -.
A Comprehensive Soap Note for an STI HPV Infection Order Instructions: Purpose: To explain what each section of the SOAP note should include. Remember that Nurse Practitioners treat patients in a holistic manner and your SOAP note should reflect that premise.
A Comprehensive Soap Note for an STI HPV Infection
SUBJECTIVE DATA: What the patient tells you but organized by you in a logical fashion
Chief Complaint (CC):
1. Location
2. Quality
3. Quantity or severity
4. Timing, including onset, duration, and frequency
5. The setting in which it occurs
6. Factors that have aggravated or relieved the symptom
7. Associated manifestations
Medications: list each one by name with dosage and frequency
Allergies: include specific reactions to medications, foods, insects, environmental
Past Medical History (PMH): Illnesses, hospitalizations, risky sexual behaviors. Include childhood illnesses
Past Surgical History (PSH): Dates, indications, and types of operations
OB/GYN History: (if applicable) Obstetric history, menstrual history, methods of contraception and sexual function
Personal/Social History: Tobacco use, Alcohol use, Drug use. Patient’s interests, ADL’s IADL’s if applicable. Exercise, eating habits
Immunizations: Last Tdp, Flu, pneumonia, etc.
Family History: Parents, Grandparents, siblings, children
Review of Systems: Go Head to toe. Cover each system that covers the Chief Complaint, History of Present Illness and History (this includes the systems that address any previous diagnoses). YOU DO NOT NEED TO DO THEM ALL UNLESS YOU ARE DOING a TOTAL H&P. Remember, this is what the patient tells you.
General: any recent weight changes, weakness, fatigue, or fever
Skin: rashes, lumps, sores, itching, dryness, changes, etc.
HEENT:
Neck:
Breasts:
Respiratory:
Cardiovascular:
Gastrointestinal:
Peripheral vascular:
Urinary:
Genital:
Musculoskeletal:
Psychiatric:
Neurological:
Hematologic:
Endocrine:
OBJECTIVE DATA: This is what you see, hear, feel when doing your physical exam. Again, you go head to toe and you only need to examine the systems that are pertinent to the CC, HPI, and History unless you are doing a total H&P. Do not use WNL or normal. You must describe what you see.
Here is where the vital signs go. Include ht and wt and BMI
General: General state of health, posture, motor activity and gait. Dress, grooming, hygiene. Odors of body or breath. Facial expression, manner, affect and reactions to people and things. Level of conscience.
SKIN:
HEENT:
Neck:
Chest/Lungs: ALWAYS INCLUDE IN YOUR PE
Heart/Peripheral Vascular: ALWAYS INCLUDE THE HEART IN YOUR PE
Abdomen:
Genital:
Musculoskeletal:
Neurological:
ASSESSMENT: Need to list your priority diagnosis(es) first. For each priority diagnosis, list at least 3 differential diagnoses. Support your selection with evidence.
Example: Migraine headache (tension headache, cluster headache, brain tumor)
Hypertension (renal disease, stress, renal artery stenosis)
For holistic care you need to include previous diagnoses and indicate whether these are controlled or not controlled and remember to include that in your treatment plan.
What evidence or guidelines did you use to support your diagnoses?
PLAN: Treatment plan. Labs, x-rays, etc. Include both pharmacological and non-pharmacological strategies. Include alternative therapies. When do they need to follow-up? Any referrals? Consultations?
Health Promotion: What does the patient/ family need to do to promote their health? Exercise, healthy diet, safety, etc.
Disease Prevention: For the patient’s age, what needs to be done to detect disease early…fasting lipid profile, mammography, colonoscopy, immunizations, etc.
What evidence did you use to support your treatment plan?
REFLECTION: What did you learn from this experience? What would you do differently? Do you agree with your preceptor based on the evidence? Really think about what you are doing in clinical.
A Comprehensive Soap Note for an STI HPV Infection Sample Answer
A Comprehensive Soap Note for an STI (HPV Infection)
S: Subjective Information
Chief Complaint (CC): “I have small bumps on my genital area.”
History of Present Illness (HPI): Ms. Z is a 21-year-old white American woman who is a sexual worker present with complaints of the presence of small bumps that developed on her genital area since she began doing her current job six months ago. She describes the bumps her genital area as being flat-topped and darker than her normal skin tone. She also describes her vaginal discharge as foul smelling and occurs during sexual intercourse and complains of an aching pelvis and experiencing some abdominal pains. She further presents with similar bumps on her feet and nails that are causing irritation. The aggravating factor was sexual intercourse with no relieving factor. She has a normal menstrual cycle with no signs of infection or disease had last being on August 20th 2014, and the age of onset was 12 years. She has multiple sexual partners and one regular partner with similar bumps. She uses the birth control pills Drospirenone and Estradiol and never uses a condom. Her Pap test taken three months ago was inconclusive. She has a previous medical admission and surgical history with unknown allergies to medicine and no childhood illness.
Medications: Bath control pills Drospirenone and Estradiol 1 daily tablet PO.
Allergies: Uknown allergies to medications, foods, insects and environment.
Past Medical History (PMH): no history of an STI, admitted for alcohol poisoning for three days in March 2013, admitted for ecstasy overdose in June 2013, admitted for starvation and fed through a tube in January 2014.
Past Surgical History (PSH): Intentional Termination of Pregnancy
(ITOP) in March 2013.
OB/GYN History:
Obstetric History: GO, TO, AO and LO. Regular menstrual period that is on time and lasts for four days and the contraception method is the birth control pill Drospirenone and Estradiol, and she is extremely sexually active.
Menstrual History: Menarche occurred at 12 years old and her last period was on August 20th 2014, and her period is regular lasting for four days. The results of her last Pap test 3 months ago were unknown.
Contraception Method: Bath control pills Drospirenone and Estradiol 1 daily tablet PO.
Personal/Social History: she is single with no children and is a commercial sex worker at a local club. She takes at least “at least six bottles of alcohol, smokes a packet of cigarettes and occasionally takes ecstasy. She rarely and has a single regular sexual partner and multiple daily and lifetime partners. She has developed a low self-esteem after the attempted rape that occurred on her 20th birthday, and she ran away from home not reporting the case to the authorities or informing the mother. She never uses a condom despite knowing the risks and has no known hobbies.
Family History: mother whose age is unknown and today she is an alcoholic and living in a shelter for the homeless.”
Review of Systems:
General: Significant changed in appetite, fatigue and weakness with a considerable weight loss.
Gastrointestinal: she experiences abdominal pains.
Genital: She reported a foul smelling vaginal discharge with no itching or burning sensation.
Psychiatric: She admits having developed depression since the attempted rape incidence
O: Objective Information
Vital Signs: BP 96/74, P 76, R 12, T 37.50 C and W 100 lbs.
General: Ms. Z is a 21-year-old woman but appears five years older than her age. She is constantly biting her nails and unsettled displaying anxiety. She looks weak and frail with a bony framework. She is well kempt, but her face seems to be having traces of makeup that was left indicating she did not take a bath. She occasionally smiles with a strong perfume. She is eloquent in English and does not speak much although she was cooperative in answering the questions.
SKIN: Pale with no rushes.
HEENT: her eyes are sagged with equal round pupils and accommodation. She has normal hair distribution and normal oral mucosa and all the teeth.
Pelvic Exam: The external genitalia had a triangular escutcheon with multiple flesh-colored lesions (>0.5 cm) in the perineal area. There was no hymen and with a piercing at the clitoris and another just above the rectocele area. There was a thick, foul-smelling yellow discharge with small masses of warts with signs of inflammation. There was right adnexal cervical tenderness and severe cervical motion tenderness. The uterus was large, smooth and mobile.
Neurological: She is alert, conscious of the time and place, and responds appropriately.
A: Assessment
Human Papillomavirus (HPV) infection. This is a small, double-stranded virus that mostly that affects the epithelial cells of the skin (Ramírez-Fort, Khan, Rady, & Tyring, 2013). This is the most likely condition as it affects the cutaneous epithelium and result into skin warts that are categorized with their epidemiological association with cervical cancer. Infection with low-risk HPV results into benign or low-grade abnormalities of the cervical cell, genital warts, and papillomas of the larynx. The high-risk HPV results into lesions that can turn into a tumor in undetected and untreated. It is passed through skin contact especially during sexual intercourse, but intercourse does not always have to be involved (Ramírez-Fort, Khan, Rady, & Tyring, 2013). The treatments include includes Podofilox 0.5% gel or solution, Imiquimod 5% cream, or Sinecatechins 15% ointment. Therapy that is provider-administered includes cryotherapy with liquid nitrogen or cryoprobe, podophyllin resin 10% – 25% in compound tincture of benzoin, or Trichloroacetic acid (TCA) or bichloroacetic acid (BCA) 80% – 90% (CDC, 2012)
Herpes Simplex Virus (HSV). This virus is part of the alpha herpes virus subfamily of the herpes viruses and is of two types HSV – 1 and HSV – 2 (Karasneh & Shukla, 2011). It is a double-stranded DNA virus forming part of the alpha herpesviridae subfamily of viruses and distinguished using their antigenic differences in their protein envelope (Azwa & Barton, 2009). This is the second likely condition as its spread through sexual intercourse and especially where there is no condom use. The infection results into the development of lesions in the perennial area of the genitals (Azwa & Barton, 2009). This is treated with antiretroviral drugs such as acyclovir, famciclovir, and valacylovir oral or topical drugs. Alternative care is also effective that is dietary supplements, and these are, for example, L-lysine, aloe Vera, eleuthro, and Echinacea (Levitsky et al., 2008).
Yeast Infection. Yeast is fungi that live in small colonies in the vagina, and an infection occurs when the yeast cell colonies increase in the vagina (Kaufmann, 2000). This is the least likely because it is not an acute condition and does not require sexual intercourse to develop. The warts are also not serious as they do not easily spread, and their treatment and side effects are not as serious as in HPV and HSV (Kaufmann, 2000). Treatment is often effective unless the infection is recurrent and often involves maintenance of proper hygiene. Pharmacological treatment involves the use of an antifungal cream, tablets, suppository, or ointment. A single flucunazole oral tablet dose is also effective. Azole medication is effective for long-term treatment and taken for seven to fourteen days (Mayo Clinic, 2014).
P: Plan
Diagnostics:
Pap Test/Pap Smear/Culture (HPV): Also known as a pap smear and investigates abnormal changes in the cervical cells. Cells to be used as samples are removed from the cervix, and they are cultured and observed through a microscope in the presence or absence of genital warts (Coutlée, Rouleau, Ferenczy, & Franco, 2005).
Antigen detection test (HSV): Fresh sore cells are scraped off they are then smeared on a microscope slide to find antigen markers on the cells found on the surface that are infected with the virus (Shulman et al., 2012).
Fungal Smear (Yeast infection): The superficial cells are obtained and cultured to isolate the yeast infection (Elin, Whitis, & Snyder, 2000).
Health promotion: She should also continue with a special protein and carbohydrate diet for the next six months, urinate and wipe properly after sexual intercourse, wear panty liners, avoid douching both in general and during treatment. Continue with regular morning run and the ortho tricycle for the next on yea and avoid intercourse with the infected regular partner and reduce sexual activity.
Referral to a counselor would be necessary to provide therapy to deal with the trauma, maintain proper hygiene, and from the attempted rape including the need for a lifestyle change and a nutritionist for proper diet and nutrition.
Return in case of recurrence and persistence of symptoms
Disease Prevention: Regular pap tests
Pharmacological therapy employed the Centre for Disease Control and Prevention guidelines on Genital warts and the Canadian Consensus Guidelines on Human Papillomavirus. The non-pharmacological guidelines were from the American Psychological ACNP and Promotion Dietary Guidelines for Americans.
Reflection
The process of diagnosis and determining the appropriate treatment for patients is rigorous and requires a careful consideration of all symptoms the patient is presenting because certain disease may have similar symptoms. For the diagnostic process, I would place more emphasis on the psychological factors of the patient as they seem to be the underlying factors for the patient’s behaviors that are putting her at risk. I would also inquire of the client can change her job as it is the greatest risk factor. The regular partner should also seek medical intervention. The evidence provided is in line with HPV and its treatment guidelines by the various bodies hence I agree with the instructor.
A Comprehensive Soap Note for an STI HPV Infection References
Azwa, A., & Barton, S. E. (2009). Aspects of Herpes Simplex Virus: A Clinical Review. J Fam Plann Reprod Health Care, 35 (4), 237–242.
Coutlée, F., Rouleau, D., Ferenczy, A., & Franco, E. (March/Aprl 2005). The Laboratory Diagnosis of Genital Human Papillomavirus Infections. Can J Infect Dis Med Microbiol, 83-91.
Elin, R. J., Whitis, J., & Snyder, J. (2000). Infectious Disease Diagnosis From a Peripheral Blood Smear. Laboratory Medicine, 31 (6), 324-328.
Karasneh, G. A., & Shukla, D. (2011). Herpes Simplex Virus Infects most Cell Types In vitro: Clues to its Success. Virology Journal, 8 (481), 1-11.
Kaufmann, D. A. (2000). The Fungus Link: An Introduction to Fungal Disease Including the Initial Phase Diet (2nd ed., Vol. 1). (B. T. Hunt, ed.) MediaTrition.
Levitsky, J., Duddempudi, A. T., Lakeman, F. D., Whitley, R. J., Luby, J. P., Lee, W. M., et al. (2008). Detection and Diagnosis of Herpes Simplex Virus Infection in Adults with Acute Liver Failure. Liver Transpl, 14, 1498-1504.
Ramírez-Fort, M. K., Khan, F., Rady, P. L., & Tyring, S. K. (eds.). (2013). Human Papillomavirus: Bench to Bedside. Basel, Switzerland: Karger Medical and Scientific Publishers.
Shulman, S. T., Bisno, A. L., Clegg, H. W., Gerber, M. A., Kaplan, E. L., Lee, G., et al. (September 9, 2012). Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases , 1-19.
We can write this or a similar paper for you! Simply fill the order form!
Assignment Assess your Knowledge of Foundational Concepts
Assess your knowledge of foundational concepts essential to the nursing management of client health by taking the interactive quiz, located in the media “Arterial Blood Gas Interpretation.” http://lc.gcumedia.com/zwebassets/courseMaterialPages/nrs410v_self-assessment-v1.1.php
The quiz is designed as a tool for self-assessment. When you encounter questions that seem vaguely familiar, click on the media’s study materials, which are organized by topic (e.g., anatomy, biology, chemistry, pharmacology). This media will serve as a refresher for the concepts that build upon one another in nursing practice.
You will have the opportunity to retake the quiz until you achieve a passing score of 100%.
Once completed, please save your results and submit to the instructor.
SAMPLE ANSWERS
Knowledge of Foundation Concepts
Student ADA Version
of the Arterial Blood Gas Interpretation Pre-Assessment
Anatomy
Backward effects of left-sided heart failure include:
In performing a physical assessment, the nurse notes the patient has a “barrel” configuration to the chest. This is a consequence of:
Reduced intrapleural pressures
Bronchial airway expansion
Increased vital capacity
Increased residual lung volume
Student ADA Version
of the Arterial Blood Gas Interpretation Pre-Assessment
Anatomy
Backward effects of left-sided heart failure include:
Pulmonary congestion
Jugular vein distention
Dependent edema in the legs
Bounding pulses
Anatomy
In performing a physical assessment, the nurse notes the patient has a “barrel” configuration to the chest. This is a consequence of:
Reduced intrapleural pressures
Bronchial airway expansion
Increased vital capacity
Increased residual lung volume
Anatomy
Ausculation of the chest reveals bilateral fine crackles in the bases bilaterally, indicating:
Right-sided heart failure
Left-sided heart failure
Pneumonia
Acute respiratory distress syndrome
Biology The signs and symptoms of anemia are all related to what common pathophysiologic feature of the condition?
Increased oxygen consumption by tissues
Decreased blood oxygen content
Vasodilation
A shift in the oxyhemoglobin dissociation curve
Biology In addition to hypertension, preeclampsia is characterized by:
Nausea and vomiting
Fatigue and lower back pain
Protein in the urine and edema
Retinal changes and rates in the lungs
Biology Common manifestations of bacterial pneumonia include all of the following except:
Fever
Productive Cough
Tachypnea
Hyperinflation
Biology Closed drainage systems work to re-expand a lung after pneumothorax by:
Re-establishing the normal negative intrapleural pressure.
Creating a positive pressure in the pleural space
Removing excess fluid from the pleural space so that there is room for lung expansion.
Pulling oxygen into distal air sacs to re-expand lung tissue
Biology Patients with chronic renal failure usually exhibit:
Bradycardia
Hypokalemia
Hypocalcemia
Hematomas
Biology The diet of a patient in end-stage kidney disease is restricted in all of the following except:
Fluid
Potassium
Protein
Calories
Anatomy
Which of the following is true of the biological functions of progesterone?
Progesterone is the most important hormone associated with pregnancy.
Progesterone directs male sexual characteristics.
Levels of progesterone increases if the egg is not fertilized.
Levels of progesterone remain stable if the egg is not fertilized.
Anatomy
Which of the following is true of the biological functions of testosterone?
Testosterone is not secreted by the ovaries.
Testosterone is needed for development of female secondary sexual characteristics.
Testosterone stimulates ovulation.
Testosterone is needed for development of male secondary sexual characteristics.
Anatomy
Which of the following is true of the biological functions of estrone?
Estrone is required for proper development of male secondary sexual characteristics.
Level of estrogen degreases if the egg is not fertilized.
Estrone is required for proper development of female secondary sexual characteristics.
Estrone affects only the reproductive organs.
Biology
What is the function of hemoglobin?
Hemoglobin is the protein in red blood cells that is responsible for carrying oxygen to the cells of the body.
Hemoglobin is a lipid in red blood cells that is responsible for carrying oxygen to the cells of the body.
Hemoglobin is a protein in white blood cells that is responsible for carrying oxygen to the cells of the body.
Hemoglobin is a protein in red blood cells that is not responsible for carrying carbon dioxide to the cells of the body.
Biology
Why is heat an effective means of sterilization?
Heat is an effective means of sterilization because it destroys the proteins of microbial lifeforms, including fungi, bacteria, and viruses.
Heat is an effective means of sterilization because it destroys the proteins of anaerobic microbial lifeforms, including fungi, bacteria, and viruses.
Heat is an effective means of sterilization because it destroys the lipids of microbial lifeforms, including fungi, bacteria, and viruses.
Both (B) and (C).
Chemistry:
List the enzymes whose levels are elevated in the blood serum following an MI.
CPK, LDH, AST, and SGOT
LDH, AST, and SGOT
CRE, AST, and ALT
None of the above
Chemistry
What is the physiological function of gluconeogenesis?
Gluconeogenesis is production of glucose from noncarbohydrate molecules in times when blood glucose levels are low. This ensures proper function of brain and red blood cells, which only use glucose as fuel.
Gluconeogenesis is production of glucose from noncarbohydrate molecules in times when blood glucose levels are high. This ensures proper function of brain and white blood cells, which only use glucose as fuel.
Gluconeogenesis is production of glucose from carbohydrate molecules in times when blood glucose levels are low. This ensures proper function of brain and red blood cells, which only use glucose as fuel.
None of the above
Chemistry
What effect does glycogen metabolism have on glucose levels?
Glycogen metabolism traps glucose within liver cells and increases storage of glucose in the form of glycogen. These processes decrease blood glucose levels.
Glycogen metabolism traps glucose within liver cells and increases storage of glucose in the form of glycogen. These processes increase blood glucose levels.
Glycogen metabolism releases glucose within liver cells and increases storage of glucose in the form of glycogen. These processes decrease blood glucose levels.
None of the above
Chemistry
Carbon monoxide binds tightly to the heme groups of hemoglobin and myoglobin. How does this affinity reflect the toxicity of carbon monoxide?
Since carbon monoxide binds the heme groups of hemoglobin, it is easily removed or replaced by oxygen. As a result, the effects of oxygen enhancement result in what divers call the “bends.”
Because carbon monoxide binds the heme groups of hemoglobin, it is easily removed or replaced by oxygen. As a result, the effects of oxygen deprivation result in suffocation.
Because carbon monoxide binds tightly to the heme groups of hemoglobin, it is not easily removed or replaced by oxygen. As a result, the effects of oxygen deprivation result in suffocation.
None of the above
Pathophysiology
Which of the following may be a reason to order an ABG on a patient?
The patient suddenly develops shortness of breath
An asthmatic is starting to show signs of tiring
A diabetic has developed Kussmaul’s respirations
All of the above
Pharmacology
How do sulfa drugs selectively kill bacteria while causing no harm to humans?
Folic acid is a vitamin required for the synthesis of a coenzyme needed to make the amino acid methionine and the purine and pyrimidine nitrogenious bases for DNA and RNA and folic acid is produced by humans.
Sulfa drug binds to the enzyme, no product is formed, folic acid is made and the biosynthesis of methionine and nitrogenous bases increases.
Humans are not harmed because they do not synthesize their own folic acid. It is obtained in the diet.
None of the above
Pharmacology
What occurs when glycogen metabolism is stimulated by insulin?
Insulin stimulates glycogen synthase, the first enzyme in glycogen synthesis.
Insulin stimulates glycogen synthase, the first enzyme in glycogen synthesis. It also stimulates removal of glucose from the bloodstream into cells and phosphorylation of glucose by the enzyme glucokinase.
Insulin stimulates glycogen synthase, the first enzyme in glycogen synthesis. It also stimulates uptake of glucose from the bloodstream into cells and phosphorylation of glucose by the enzyme glucokinase.
All of the above
Pharmacology
What is the medical application of cortisone? Cortisone is used to treat:
Rheumatoid arthritis, asthma, gastrointestinal disorders, and a variety of skin conditions.
Kidney disease, high blood pressure, and osteoporosis.
Muscle disorders, tuberculosis, and thyroid disorder.
All of the above
Anatomy
Oxygen saturation is likely to be lowest when an asthmatic with a diagnosis of pneumonia is positioned:
In a high Fowler position
Lying on the left side
Lying on the right side
Lying supine with the head of the bed flat
Chemistry
Laboratory test results indicative of thrombocytopenia, in addition to a low platelet count, would be:
Increased PT
Prolonged bleeding time and poor clot retraction.
Increased aPTT
Decreased RBC count.
Pharmacology
The purposes of epinephrine injection include all of the following except:
Stabilizing mast cell membranes.
Relaxing bronchial smooth muscle.
Supporting arterial blood pressure.
Blocking histamine receptors.
Pharmacology Therapeutic interventions focused on increasing the oxygen supplied to the heart and decreasing the heart’s demand for oxygen include:
Antiplatelet drugs
Anticoagulants
Morphine sulphate
Thrombolytic drugs
Pharmacology An intervention that would contribute toward the healing of a peptic ulcer is:
Steroid administration
Blocking or neutralizing of acid secretion
Surgical removal of the ulcer
Intravenous nutritional support
Pharmacology Aspirin and NSAIDs are causative factors for the development of peptic ulcer disease because they:
Increase acid secretion
Allow proliferation of H. pylori
Damage the mucosal barrier
Alter platelet aggregation
Pharmacology Your patient is interested in trying medication to improve low mood/depression. All of the following medications might be appropriate except:
Selective serotonin reuptake inhibitors
Amitriptyline
Serotonin and norepinephrine reuptake inhibitors
Benzodiazepines
Anatomy
Ausculation of the chest reveals bilateral fine crackles in the bases bilaterally, indicating:
Right-sided heart failure
Left-sided heart failure
Pneumonia
Acute respiratory distress syndrome
Biology The signs and symptoms of anemia are all related to what common pathophysiologic feature of the condition?
Increased oxygen consumption by tissues
Decreased blood oxygen content
Vasodilation
A shift in the oxyhemoglobin dissociation curve
Biology In addition to hypertension, preeclampsia is characterized by:
Nausea and vomiting
Fatigue and lower back pain
Protein in the urine and edema
Retinal changes and rates in the lungs
Biology Common manifestations of bacterial pneumonia include all of the following except:
Fever
Productive Cough
Tachypnea
Hyperinflation
Biology Closed drainage systems work to re-expand a lung after pneumothorax by:
Re-establishing the normal negative intrapleural pressure.
Creating a positive pressure in the pleural space
Removing excess fluid from the pleural space so that there is room for lung expansion.
Pulling oxygen into distal air sacs to re-expand lung tissue
Biology Patients with chronic renal failure usually exhibit:
Bradycardia
Hypokalemia
Hypocalcemia
Hematomas
Biology The diet of a patient in end-stage kidney disease is restricted in all of the following except:
Fluid
Potassium
Protein
Calories
Anatomy
Which of the following is true of the biological functions of progesterone?
Progesterone is the most important hormone associated with pregnancy.
Progesterone directs male sexual characteristics.
Levels of progesterone increases if the egg is not fertilized.
Levels of progesterone remain stable if the egg is not fertilized.
Anatomy
Which of the following is true of the biological functions of testosterone?
Testosterone is not secreted by the ovaries.
Testosterone is needed for development of female secondary sexual characteristics.
Testosterone stimulates ovulation.
Testosterone is needed for development of male secondary sexual characteristics.
Anatomy
Which of the following is true of the biological functions of estrone?
Estrone is required for proper development of male secondary sexual characteristics.
Level of estrogen degreases if the egg is not fertilized.
Estrone is required for proper development of female secondary sexual characteristics.
Estrone affects only the reproductive organs.
Biology
What is the function of hemoglobin?
Hemoglobin is the protein in red blood cells that is responsible for carrying oxygen to the cells of the body.
Hemoglobin is a lipid in red blood cells that is responsible for carrying oxygen to the cells of the body.
Hemoglobin is a protein in white blood cells that is responsible for carrying oxygen to the cells of the body.
Hemoglobin is a protein in red blood cells that is not responsible for carrying carbon dioxide to the cells of the body.
Biology
Why is heat an effective means of sterilization?
Heat is an effective means of sterilization because it destroys the proteins of microbial lifeforms, including fungi, bacteria, and viruses.
Heat is an effective means of sterilization because it destroys the proteins of anaerobic microbial lifeforms, including fungi, bacteria, and viruses.
Heat is an effective means of sterilization because it destroys the lipids of microbial lifeforms, including fungi, bacteria, and viruses.
Both (B) and (C).
Chemistry:
List the enzymes whose levels are elevated in the blood serum following an MI.
CPK, LDH, AST, and SGOT
LDH, AST, and SGOT
CRE, AST, and ALT
None of the above
Chemistry
What is the physiological function of gluconeogenesis?
Gluconeogenesis is production of glucose from noncarbohydrate molecules in times when blood glucose levels are low. This ensures proper function of brain and red blood cells, which only use glucose as fuel.
Gluconeogenesis is production of glucose from noncarbohydrate molecules in times when blood glucose levels are high. This ensures proper function of brain and white blood cells, which only use glucose as fuel.
Gluconeogenesis is production of glucose from carbohydrate molecules in times when blood glucose levels are low. This ensures proper function of brain and red blood cells, which only use glucose as fuel.
None of the above
Chemistry
What effect does glycogen metabolism have on glucose levels?
Glycogen metabolism traps glucose within liver cells and increases storage of glucose in the form of glycogen. These processes decrease blood glucose levels.
Glycogen metabolism traps glucose within liver cells and increases storage of glucose in the form of glycogen. These processes increase blood glucose levels.
Glycogen metabolism releases glucose within liver cells and increases storage of glucose in the form of glycogen. These processes decrease blood glucose levels.
None of the above
Chemistry
Carbon monoxide binds tightly to the heme groups of hemoglobin and myoglobin. How does this affinity reflect the toxicity of carbon monoxide?
Since carbon monoxide binds the heme groups of hemoglobin, it is easily removed or replaced by oxygen. As a result, the effects of oxygen enhancement result in what divers call the “bends.”
Because carbon monoxide binds the heme groups of hemoglobin, it is easily removed or replaced by oxygen. As a result, the effects of oxygen deprivation result in suffocation.
Because carbon monoxide binds tightly to the heme groups of hemoglobin, it is not easily removed or replaced by oxygen. As a result, the effects of oxygen deprivation result in suffocation.
None of the above
Pathophysiology
Which of the following may be a reason to order an ABG on a patient?
The patient suddenly develops shortness of breath
An asthmatic is starting to show signs of tiring
A diabetic has developed Kussmaul’s respirations
All of the above
Pharmacology
How do sulfa drugs selectively kill bacteria while causing no harm to humans?
Folic acid is a vitamin required for the synthesis of a coenzyme needed to make the amino acid methionine and the purine and pyrimidine nitrogenious bases for DNA and RNA and folic acid is produced by humans.
Sulfa drug binds to the enzyme, no product is formed, folic acid is made and the biosynthesis of methionine and nitrogenous bases increases.
Humans are not harmed because they do not synthesize their own folic acid. It is obtained in the diet.
None of the above
Pharmacology
What occurs when glycogen metabolism is stimulated by insulin?
Insulin stimulates glycogen synthase, the first enzyme in glycogen synthesis.
Insulin stimulates glycogen synthase, the first enzyme in glycogen synthesis. It also stimulates removal of glucose from the bloodstream into cells and phosphorylation of glucose by the enzyme glucokinase.
Insulin stimulates glycogen synthase, the first enzyme in glycogen synthesis. It also stimulates uptake of glucose from the bloodstream into cells and phosphorylation of glucose by the enzyme glucokinase.
All of the above
Pharmacology
What is the medical application of cortisone? Cortisone is used to treat:
Rheumatoid arthritis, asthma, gastrointestinal disorders, and a variety of skin conditions.
Kidney disease, high blood pressure, and osteoporosis.
Muscle disorders, tuberculosis, and thyroid disorder.
All of the above
Anatomy
Oxygen saturation is likely to be lowest when an asthmatic with a diagnosis of pneumonia is positioned:
In a high Fowler position
Lying on the left side
Lying on the right side
Lying supine with the head of the bed flat
Chemistry
Laboratory test results indicative of thrombocytopenia, in addition to a low platelet count, would be:
Increased PT
Prolonged bleeding time and poor clot retraction.
Increased aPTT
Decreased RBC count.
Pharmacology
The purposes of epinephrine injection include all of the following except:
Stabilizing mast cell membranes.
Relaxing bronchial smooth muscle.
Supporting arterial blood pressure.
Blocking histamine receptors.
Pharmacology Therapeutic interventions focused on increasing the oxygen supplied to the heart and decreasing the heart’s demand for oxygen include:
Antiplatelet drugs
Anticoagulants
Morphine sulphate
Thrombolytic drugs
Pharmacology An intervention that would contribute toward the healing of a peptic ulcer is:
Steroid administration
Blocking or neutralizing of acid secretion
Surgical removal of the ulcer
Intravenous nutritional support
Pharmacology Aspirin and NSAIDs are causative factors for the development of peptic ulcer disease because they:
Increase acid secretion
Allow proliferation of H. pylori
Damage the mucosal barrier
Alter platelet aggregation
Pharmacology Your patient is interested in trying medication to improve low mood/depression. All of the following medications might be appropriate except:
Prevention of Type 2 Diabetes in Adolescent Navajo Indians
Prevention of Type 2 Diabetes in Adolescent Navajo Indians
Order Instructions:
Please take note that I will send two document for this assignment , which will include the letter to the stakeholder, and a promotional pamphlet which the writer is to use for this paper. also he has to search online for additional information on this particular case study as require by the assignment . He should pay attention to all details and respond to all questions in the case study clearly as the prof will asses to see that all questions where responded to. They are 5 key questions in the case study, so the writer must provide 5 key sections clearly responding to this 5 questions
Case Study: Prevention of Type 2 Diabetes in Adolescent Navajo Indians
Directions
For this assignment please follow these instructions in sequence.
– Complete all assigned reading noted in the resource section at the end of the questions before attempting this assignment.
– Review the two promotional documents provided for the launch of the community health promotion ( letter to stakeholders and Promotional Pamphlet).
– Locate data and documents necessary to answer the case study questions from the internet.
Case Study Questions:
a. As a key stakeholder, were you swayed to support this community health Initiative? Please support your yes or no answer with rationale
b. Was the data presented sufficient to support this community health proposal?
c. Identify at least four strengths of this proposal?
d. Identify at least four weaknesses of this proposal?
e. For the weaknesses identified propose valid solutions with supporting rationales
These answers should be contained in a paper no longer than 3 pages, excluding title page and references. The document should be in appropriate 6th edition APA format.
Resources to aid in the paper.
Health Promotion in Nursing Practice
• Chapters 4, 5, 6, 7 and 9
Benjamins, M. R., & Whitman, S. (2010). A Culturally Appropriate School Wellness Initiative: Results of a 2-Year Pilot Intervention in 2 Jewish Schools. Journal Of School Health, 80(8), 378-386.
It is important that writer read and reference to the above readings for this paper.
SAMPLE ANSWER
Prevention of Type 2 Diabetes in Adolescent Navajo Indians
Was the stakeholder swayed?
There are high chances that the key stakeholder will be swayed based on the fact that this is meant to create awareness. On the contrary, the matter is very critical and requires immediate and solid support and attention. It was important to point out that diabetes was infrequent among the Navajo youths who were less than ten years. On the contrary, the incidence and prevalence of the disease was extremely high among the older youths. This would have been very vital in ensuring that the main stakeholder supported the program at Gallup, New Mexico and beyond. Moreover, if aware of the seriousness of the disease though the incidence, prevalence, and impacts among the adolescent Navajo youths, he would also support the proposed prevention and management strategies.
Sufficiency of the data
The data provided was not adequate to support the proposal. It was important to present the facts regarding the prevalence, incidence, factors contributing to the disease, and the effects the disease has on the adolescent Navajo Indians. This would have emphasized the gravity of the issue and, thereby, ensuring more support of the proposal. Emphasizing how critical a matter is among a certain target group as well as how the disease impacts on the affected can go a long way in ensuring that the program is supported as needed.
Strengths
The proposal is prepared by professional nurses from Gallup Indian Medical Center. In this case, the school community has higher chances of accepting the proposal based on credible professionalism. Moreover, the proposal was written by the lead designer of the proposal. Second, the proposal is relevant to the challenges facing the Navajo Indians (Work group for community health and development at the University of Kansas, 2012). The community health proposal addresses prevention of diabetes types 2 among the adolescent Navajo Indians. This is based on the fact that the prevalence of the disease is high among the adolescents and, therefore, many other stakeholders are likely to support the community health proposal since it addresses an actual community challenge (Tran et al., 2014).
Third, the target group chosen for the community health proposal is fit. It was strategic for the proposal proponents to choose a middle school system (5TH, 6TH, 7TH, or 8TH grade students) in Gallup New Mexico since these basically constitute of the affected adolescents. It was easier to locate the target group from a school. Fourth, the proposal will first be presented to the school board meeting. This is very crucial in ensuring that the school management supported the proposal and encouraged the students to enroll for the program.
Weaknesses
The proposal is lacking in that the seriousness of the cause has not been emphasized. There was a great need to indicate the actual figures (prevalence and incidence) of the disease (Dabelea et al., 2014). This would have ensured that the proposal was supported by the key as well as other stakeholders. In the proposal, it is stated that a community health proposal was developed and aimed at students who were then in middle school system in relation to type 2 diabetes prevention. However, there is no mention of why this was important for this target group. What effects does the disease affect this age group?
The diabetes type 2 community health proposal also lacks in that there is no mention of why prevention is being advocated for. There are other approaches that could have been taken including management, treatment, awareness creation, or control of the disease. However, since the proponents have settled on prevention, it is important to mention why this is the approach they consider more proper (Imperatore et al., 2012). Not only does the proposal fail to point out the significance of the matter to the key stakeholders, the promotional pamphlet is also not convincing. Seeing such a promotional pamphlet, many adolescents who are not aware of the diabetes type 2 concern among the adolescent Navajo Indians will ignore it (Work group for community health and development at the University of Kansas, 2012).
Valid solutions for the weaknesses
The prevalence and incidence of diabetes type 2 among the adolescent Navajo Indians should be highlighted and compared to statistics of other adolescents elsewhere. This would emphasize on the gravity of the matter. It is also important to mention why this target group is important as far as the disease and adolescent Navajo Indians are concerned. The proposal should have elaborated in detail why this age group was particularly of concern
The proponent of the proposal should mention and explain the benefits or advantage of preventing diabetes type 2. This is based on the fact that they could have adopted other approaches. But since they settled on prevention, there is a need to mention how prevention of the disease is useful (Benjamins & Whitman, 2010). The promotional pamphlet should have at least indicated how serious the matter is among these adolescents through a mention of the incidence and prevalence. Moreover, there should be a mention of why prevention is important. This measure would go a long way in ensuring that many adolescents enrolled for the program.
References
Benjamins, M. R., & Whitman, S. (2010). A Culturally Appropriate School Wellness Initiative: Results of a 2-Year Pilot Intervention in 2 Jewish Schools. Journal Of School Health, 80(8), 378-386.
Tran, F., Stone, M., Huang, C. Y., Lloyd, M., Woodhead, H. J., Elliott, K. D. & Craig, M. E. (2014). Population‐based incidence of diabetes in Australian youth aged 10–18 yr: increase in type 1 diabetes but not type 2 diabetes. Pediatric diabetes.
Dabelea, D., Mayer-Davis, E. J., Saydah, S., Imperatore, G., Linder, B., Divers, J. & Hamman, R. F. (2014). Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA, 311(17), 1778-86.
Imperatore, G., Boyle, J. P., Thompson, T. J., Case, D., Dabelea, D., Hamman, R. F. & Standiford, D. (2012). Projections of Type 1 and Type 2 Diabetes Burden in the US Population Aged< 20 Years Through 2050 Dynamic modeling of incidence, mortality, and population growth. Diabetes Care, 35(12), 2515-2520.
We can write this or a similar paper for you! Simply fill the order form!
Order instructions
Differential Diagnosis for Skin Conditions
Properly identifying the cause and type of a patient’s skin condition involves a process of elimination known as differential diagnosis. Using this process, a health professional can take a given set of physical abnormalities, vital signs, health assessment findings, and patient descriptions of symptoms, and incrementally narrow them down until one diagnosis is determined as the most likely cause.
In this Discussion, you will examine several visual representations of various skin conditions, describe your observations, and use the techniques of differential diagnosis to determine the most likely condition.
To prepare:
• Review the Skin Conditions document provided (the picture of different skin condition document will be uploaded for you), and select two conditions to closely examine for this Discussion.
• Consider the abnormal physical characteristics you observe in the graphics you selected. How would you describe the characteristics using clinical terminologies?
• Explore different conditions that could be the cause of the skin abnormalities in the graphics you selected.
• Consider which of the conditions is most likely to be the correct diagnosis, and why.
1) Post on or before Day 3 a description of the two graphics you selected (identify each graphic by number).please use the document of the skin condition uploaded.
2) Use clinical terminologies to explain the physical characteristics featured in each graphic.
3) Formulate a differential diagnosis of three to five possible conditions for each.
4) Determine which is most likely to be the correct diagnosis, and explain your reasoning.
Readings/Recommended References (you may choose your own textbook or articles for this paper)
• Seidel, H. M., Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (2011). Mosby’s guide to physical examination (7th ed.). St. Louis, MO: Elsevier Mosby.
o Chapter 8, “Skin, Hair, and Nails” (pp. 150–212)
This chapter reviews the basic anatomy and physiology of skin, hair, and nails. The chapter also describes guidelines for proper skin, hair, and nails assessments.
• Dains, J. E., Baumann, L. C., & Scheibel, P. (2012). Advanced health assessment and clinical diagnosis in primary care (4th ed.). St. Louis, MO: Mosby, Elsevier.
o Chapter 25, “Rashes and Skin Lesions” (pp. 303–320)
This chapter explains the steps in an initial examination of someone with dermatological problems, including the type of information that needs to be gathered and assessed.
• LeBlond, R. F., Brown, D. D., & DeGowin, R. L. (2009). DeGowin’s diagnostic examination (9th ed.). New York, NY: McGraw Hill Medical.
o Chapter 6, “The Skin and Nails”
In this chapter, the authors provide guidelines and procedures to aid in the diagnosis of skin and nail disorders. The chapter supplies descriptions and pictures of common skin and nail conditions.
• Chadha, A. (2009). Assessing the skin. Practice Nurse, 38(7), 43–48.
Retrieved from a Library databases.
In this article, the author explains how to take a relevant skin health history. In addition, the article defines common terms used to describe skin lesions and rashes.
• Ely, J. W., & Stone, M. S. (2010). The generalized rash: Part I. Differential diagnosis. American Family Physician, 81(6), 726–734.
Retrieved from http://www.aafp.org/afp/2010/0315/p726.html
This article focuses on common, uncommon, and rare causes of generalized rashes. The article also specifies tests to diagnose generalized rashes.
• Ely, J. W., & Stone, M. S. (2010). The generalized rash: Part II. Diagnostic approach. American Family Physician, 81(6), 735–739.
Retrieved from http://www.aafp.org/afp/2010/0315/p735.html
This article revolves around the diagnosis of generalized rashes. The authors describe clinical features that may help in distinguishing generalized rashes.
• Document: Skin Conditions (Word document)
This document contains five images of different skin conditions. You will use this information in this week’s Discussion.
SAMPLE ANSWER
Differential Diagnosis for Skin Conditions
Introduction
Just like any other part of the human organic system, diagnosis of different skin conditions often involves a history, examination and additional tests of the skin. The more the skin is visible to the naked eye, the easier it will be for the diagnosis to be made. This will also allow the skin specialist to label the type of disease process being considered (LeBlond, Brown, & DeGowin, 2009). Skin diagnosis will also involve the use of different visual clues that include; individual lesion morphology, body color, site distribution, arrangement of lesions and body scaling. At some point the recognition of the skin pattern may become complex especially when the skin components are analyzed separately (Seidel, Ball, Dains, Flynn, Solomon, & Stewart, 2011). Other factors that the skin specialist will also look at will be the histopathology examination of skin biopsies and the causes. Most skin conditions rely on the presence of a constellation of histopathological, immunopathological or clinical genetic features. This is even common in diseases such as psoriasis.
Case analysis
The skin condition that has been illustrated in the picture attached is known as Eczema. The most possible type of this skin condition atopic Eczema due to the fact that the condition may have been caused by other underlying illnesses such as hay fever or asthma (Seidel, Ball, Dains, Flynn, Solomon, & Stewart, 2011).
Graphic classification of the skin condition will look at the type of lesion being treated. For example, if the skin condition has moist weeping lesions then wet dressing changes or lotions will be of good help due to the fact that it will assist in drying up the dermatitis as it provides for a cool and soothing relief. However if the graphic presents acute exudative dermatoses, then bland treatment in liquid vehicles will be most recommended (Dains, Baumann, & P.Scheibel, 2012). If the graph presents chronic psoriasis then a lot of therapy involving creams and ointments will be vital to retaining native moisture and provide relief to the pruritic and dry skin condition.
Atopic Eczema of this kind came about due to genetic defect in proteins that support the epidermal barrier. During treatment, the patient will have to undergo a process that is aimed at reducing pruritus and dermatitis from spreading, reduction of excerbations and also reduce the risk of the whole therapy. Usually the treatment will be centered on the use of topical anti-inflammatory moisturization of the skin (LeBlond, Brown, & DeGowin, 2009). However, if the condition is more serious than the patient will require phototherapy.
Eczema skin condition is usually caused by various factors, however the most known is the overactive response to the body immune system to an irritant which eventually causes the skin condition. Also families that have a history of a person suffering from eczema are most likely to contact the skin condition too. Other symptoms may include ‘flare-ups’ of an itchy rash due to irritation of a certain substance. Other people contact the skin condition due to the weather or being exposed to certain house hold products (LeBlond, Brown, & DeGowin, 2009).
Conclusion
Up to this moment there is no cure for the eczema skin condition, however the disease can be well managed through a proper medical treatment plan. The condition is not also contagious meaning it cannot spread from one person to the other. In addition the person also needs to stay away from irritating places as this could make it worse.
References
Dains, J., Baumann, L., & P.Scheibel. (2012). Advanced health assessment and clinical diagnosis in primary care . St. Louis: MO: Mosby, Elsevier.
Note: I attached the article for the research paper, it’s the main article. please read and write a research about it. the main idea should be from the
main article. the other references should support or against the idea of the mail article.
Supporting general knowledge information can be obtained from properly cited textbooks, encyclopedias,internet sites(not Wikipedia). Most of your information should come from recent peer-reviewed scientific journals not less than 5 years old.
Your assignment must follow these formatting requirements:
Be typed, double spaced, using Times New Roman font (size 12), with one-inch margins on all sides; citations and references must follow APA or school-specific format. Check with your professor for any additional instructions.
Include a cover page containing the title of the assignment, the student’s name, the professor’s name, the course title, and the date. The cover page and the reference page are not included in the required assignment page length.
We can write this or a similar paper for you! Simply fill the order form!