Have to complete at lease 10 empirical articles in my educational field. I work with children Kinder – Fifth grade.
SAMPLE ANSWER
Diabetes mellitus Annotated Bibliography
Seino, Y., Nanjo, K., Tajima, N., Kadowaki, T., Kashiwagi, A., & Araki, E. et al. (2010). Report of the Committee on the Classification and Diagnostic Criteria of Diabetes Mellitus. Journal Of Diabetes Investigation, 1(5), 212-228.
The article classifies the two types of diabetes mellitus, type 1, and diabetes type. It also discusses the causes of the various types of diabetes mellitus and the factors that are likely to predispose one to diabetes mellitus. In making the distinction type, I am referred to as insulin dependent diabetes mellitus associated with the destruction of pancreatic beta cells while type 2 is associated with lifestyle changes especially obesity.
Reinehr, T. (2013). Type 2 diabetes mellitus in children and adolescents. World Journal Of Diabetes, 4(6), 270.
The article reviews the causes of type two diabetes mellitus in children. Specifically, it looks at the factors that predispose children to diabetes mellitus type 2 since it’s commonly associated with lifestyle changes. It also looks at the methods for treatment of type 2 diabetes as well as management of children suffering from type 2 diabetes.
Ewald, N. (2013). Diagnosis and treatment of diabetes mellitus in chronic pancreatitis. World Journal Of Gastroenterology, 19(42), 7276.
A review is given on chronic pancreatitis. It should be remembered that diabetes type 1 involves the destruction of the beta cells of the pancreas by autoantibodies.in this case methods for detection of type 1 diabetes mellitus are outlined as well as the treatment.
Buchanan, T., Xiang, A., & Page, K. (2012). Gestational diabetes mellitus: risks and management during and after pregnancy. Nat Rev Endocrinal, 8(11), 639-649.
The article review a different type of diabetes mellitus commonly observed in pregnant women. It is known as gestational diabetes mellitus. It plays an important role in making a woman susceptible to diabetes mellitus type 2. Nutritional effects as wells as the risks associated with gestational diabetes mellitus are reviewed in this article.
Sacks, D., Arnold, M., Bakris, G., Bruns, D., Horvath, A., & Kirkman, M. et al. (2011). Executive Summary: Guidelines and Recommendations for Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus. Lab Med Online, 1(4), 173. http://dx.doi.org/10.3343/lmo.2011.1.4.1
The article looks and compares the different methods that are used to diagnose the different types of diabetes mellitus. Laboratory guidelines and the permitted reference range values of the results are also provided.
Litmanovitch, E. (2015). Short and long-term neurobehavioral alterations in type 1 diabetes mellitus pediatric population. World Journal Of Diabetes, 6(2), 259.
The article reviews the neurological damage that is associated with diabetes mellitus type 1. It also discusses the emerging technology that will assist in reducing the glycemic glucose levels, therefore, reducing the effects of diabetes mellitus, especially to the neural system.
Antonelli, A. (2014). Hepatitis C virus infection and type 1 and type 2 diabetes mellitus. World Journal Of Diabetes, 5(5), 586.
The article identifies the relationship between diabetes mellitus and hepatitis C. the main relationship is associated with viral effects, pro-inflammatory cytokines and insulin resistance in the liver. It also shows how clinical trial conducted on hepatitis c patients has resulted in a decrease in the glucose metabolism providing an important mode of treatment for glycemic patients.
Nauck, M. (2014). Update on developments with SGLT2 inhibitors in the management of type 2 diabetes. DDDT, 1335.
The author discusses the important role that the kidney plays in the maintaining of glucose levels in the body via the sodium glucose transporters type 2. Use of sodium glucose transporters inhibitors reduces the renal reabsorption of glucose, in the long run, decreasing the amount of glucose in the body.
Igwe, M., Uwakwe, R., Ahanotu, C., Onyeama, G., Bakare, M., & Ndukuba, A. (2013). Factors associated with depression and suicide among patients with diabetes mellitus and essential hypertension in a Nigerian teaching hospital. Af Hlth Sci, 13(1). http://dx.doi.org/10.4314/ahs.v13i1.10
The study was conducted in Nigeria to highlight the effects of diabetes mellitus and hypertension to the normal lives of the people. Basically, two concepts were looked at. The role of diabetes mellitus in causing suicidal and depression in patients.
Eisenbarth, G. (2010). Banting Lecture 2009: An Unfinished Journey: Molecular Pathogenesis to Prevention of Type 1A Diabetes. Diabetes, 59(4), 759-774.
The article discusses the metabolic pathways that are involved in diabetes mellitus specifically carbohydrate, fat and protein metabolism. It also discusses how this pathway can be used to block the effects of hyperglycemia in type 1 diabetes mellitus patients.
We can write this or a similar paper for you! Simply fill the order form!
Hi pleaseclick on link above . And log in with my username and u r required to read each module and assessment task Given at the end and write on it in relation my specialty area which was preoperative. And u need to cite whatever u write with peer reviewed articles or references . Make sure u read all the modules before u start writing assignment .
It’s 1000 words altogether (3 modules )
SAMPLE ANSWER
Module 1: legal responsibility in preoperative care
Personnel in the preoperative settings have numerous responsibilities in relation to the legal and ethical responsibilities. This is because their duty of delivering care is deep seated core within the nursing principles and code of conduct. In this context, the documentation of nursing care is a legal responsibility during preoperative care. This is the only proof they can use in their defense that they are not negligent (Litwack, 2010). The documentation process must meet the established practice of documentation. The records must indicates patients preoperative assessment, care provided by the surgical team, the outcomes and evaluation plan conducted as they are used to indicate the procedures that should be used in primary care settings. One of the most important documentation processes in preoperative care is the informed consent (Lim et al., 2010).
The main element of quality care in preoperative department is the issue of informed consent. The general legal principle of preoperative care is that the healthcare provider must obtain a valid informed consent from their patient, before any treatment intervention is put in place. This principle is put in place to ensure that the patient enjoys the right to their health, and to decide what health care practice that takes place in their body. This right is entitled to every patient including the children, but the laws have specific rules that should be followed for these minors, or patient under critical care (Litwack, 2010).
Additionally, patient have right to confidentiality, unless they have allowed their health condition be shared in the consent form. This implies that the patient have a legal right that must be obeyed by the healthcare providers in the preoperative care, if the patient refuses presence of visitors during this phase. The healthcare providers have a legal responsibility of informing all the patient’s visitors and the contractors that the preoperative environment is a very confidential department, and that it is only chaperoned by the staff members assigned in these departments only. If the visitors are present for any reasons, it must be recorded in the theatre record for referencing purposes (Tilse and Wilson, 2013).
Module 2: Dilemma of providing patient information to carers
Patient privacy is important as it upholds patient’s dignity, which is a core nurse principle and fundamental aspect of care. The physicians are often face challenges as patients health deteriorates, especially when they have to deliver relevant information that can be used at home care. More often, doctors face criticism from family relatives and carers for not giving patients adequate information. This is because it is the physician legal obligation to respect and to protect patient information. Traditionally, patient privacy philosophy argues that patient identify the person who can be informed about their health condition, and including if the information can be shared with the friends or the family (Gold et al., 2009).
This theoretical model, which focuses on patient centered care, is not always the clinical reality. The legal obligations demands that such information should be provided is there is explicit permission. This can create huge debate if a relative who have been at the center of delivering care of patient is denied the patient information. On the contrary, if the patient condition does not permit them to make decisions for themselves due to severe illness or dementia, then the family or carer can be integrated in the decision making process. These two scenarios indicate divergent positions in the communication between the patient’s carers and the physicians. This indicates that the culture of patient centered care in some cases can create tensions in healthcare (Atkinson & Coia, 2012).
In reality, the family members and carers are always concerned about the patient health. This is especially important during transition of care from acute settings to homes. In this context, the patients discharged from the hospital are weak and will rely on caregiver for their daily activity. Research indicates that providing patient information to carer is beneficial because it reduces carer anxiety, improve competency, and improve the coping strategies that will facilitate the decision-making processes. These findings have been supported by one studies conducted in cancer patients. From this perspective, then it is true that the carers work is often unrecognized, and often overlooked due to the way the medical ethics and law protects the patient’s information. These individualistic ethics dominating the healthcare practice could be hindering quality care (Gold et al., 2009).
Therefore, it is important to empower the carer with clear and effective communication about the essentials as they undertake the quasi-nurse role. This is because the patient carer knows the patient best. The carer is the constant support in patient’s life, and over time, the patient builds trust. Research indicates that the carer are encouraged and feel appreciated when integrated in decision making processes, as they become aware of the patients physical and psychological demands than when denied access to patient information (Atkinson & Coia, 2012).
Module 3: Reflection
Patient perspective about illness, disease, dying and death is best explained by the Spoon theory developed by Christine Miserandino. According to her, illness especially those diagnosed with chronic illness such as systemic lupus makes the patient have limited expendable energy. This is because even a small activity makes a patient loose a spoon (energy), which is very difficult to retrieve back. Her perspective about systemic lupus and all chronic illnesses are that patients are weak to even to undertake simple daily activities such as taking birth, walking and feeding. This is similar to the daily incidences that we deal with at the perioperative care. Most of the perioperative patients lack the exact words to explain the way they feel or their worries. This narration has helped me in understands the needs, the struggles and the services needed by the patients, especially those under preoperative care (Wagner et al., 2010).
From this narration, I have learnt that the most affected individuals during illness, dying and death are friends and the close relatives. From the narration, it is evident that healthy people are usually distressed and have unimaginable fear about illness, especially in chronic illness such as lupus. For instance, the narration indicates that the patient friend got confused and may felt helpless during the treatment regimes. However, as indicated in Maggie’s case study of hope in recovery, it is important for the family to understand, and to find ways they can meaningfully participate in their patient’s recovery, and to understand that their acceptance positively impact the response of their loved ones. The family have crucial role especially in hospital settings. They must a way to advocate for quality care for the loved ones (Atkinson & Coia, 2012).
As indicated in Maggie’s story of hope in recovery case study and Christine’s story of the twelve spoons, the healthcare role in managing patients goes beyond offering quality care alone. I have learnt that the healthcare providers have additional role to care giving which includes educators, advocates, and counselors. The healthcare staffs have the responsibility of helping the patients to understand the disease they are suffering from, and to ensure they understand and accept the management of their condition. This activity is important as it builds the gap between the healthcare providers and the patient. Additionally, it offers emotional support that will help the patient cope with the illnesses (Bennet et al., 2010).
References
Atkinson,J.M., & Coia, D.A. (2012). Responsibility to carers — an ethical dilemma. Psychiatric Bulletin 11/1989; 13(11):602-604. DOI: 10.1192/pb.13.11.602
Bennet, A., Coleman, E., Parry, C., Bodenheimer, T., and Chen, E. (2010). Health Coaching for Patients With Chronic Illness. Fam Pract Manag. 2010 Sep-Oct;17(5):24-29.
Gold, M., Philip, J., McIver, S., & Komesaroff, P. A. (2009). Between a rock and a hard place: exploring the conflict between respecting the privacy of patients and informing their carers. Internal Medicine Journal, 39(9), 582-587. doi:10.1111/j.1445-5994.2009.02020.x
Litwack, K. (2009). Clinical coach for effective perioperative nursing care. F.A. Davis Company. Philadelphia
Lim, J., Bogossian, F., & Ahern, K. (2010). Stress and coping in Australian nurses: a systematic review. International Nursing Review, 57(1), 22-31. doi:10.1111/j.1466-7657.2009.00765.x
Tilse, C., & Wilson, J. (2013). Recognising and responding to financial abuse in residential aged care. The Journal of Adult Protection, 15(3), 141-152. doi:http://dx.doi.org/10.1108/JAP-11-2012-0025
Wagner, G., Lorenz, K.A., Riopelle, D., Steckart, M.J., Rosenfeld, K. (2010). Provider Communication and Patient Understanding of Life-Limiting Illness and Their Relationship to Patient Communication of Treatment Preferences. Journal of pain and symptom management ; 39(3):527-34. DOI: 10.1016/j.jpainsymman.2009.07.012
We can write this or a similar paper for you! Simply fill the order form!
Impact of Community Health Assessments Order Instructions: please follow all the guidelines attached……
Impact of Community Health Assessments
it’s 1500 words essay and at least 18 APA format references as per guidelines attached…. thanks
Impact of Community Health Assessments Sample Answer
Introduction
Obesity is a major health challenge that is facing Australians. Overweight and obesity is defined as the accumulation of adipose tissue (Dickie et al., 2014). Overweight and obesity is identified as a secondary disease for almost all noncommunicable diseases including cardiovascular disease, Diabetes Type 2, musco-skeletal disorders, psychosocial disorders and cancer. Overweight and obesity is ranked among the leading cause of disability and mortality (Jimenez-Pavon, 2013). This paper reviews the prevalence of overweight and obesity across the Greater Geelong population. The aim of the paper is to assess the health needs, which is vital for targeting strategic interventions and for the evaluation process.
Community health assessments
The overall objective of the Geelong governance is to ensure that the healthcare programs as well as the strategies integrated meet the community local demands. The community assessment conducted by the Needs Assessment Project Group (NAPG) is established to undertake comprehensive assessments of the community needs (Health Together Geelong, 2014). The NAPG provided a comprehensive overview of the health status of the Greater Geelong population in terms of dietary patterns, physical activeness, substance use and community age trends (Health Together Geelong, 2014). The community assessment was conducted on 436 residents in the Geelong community, who were randomly selected. The health surveys were conducted based on community assisted telephone interviews (CATI). Supportive information was obtained from the Victorian Health Information Surveillance systems (VHISS), a website that displays the health indicators (Health Together Geelong, 2014).
From the analysis, it is evident that the obesity and overweight rates in the Geelong community is increasing at alarming rates. The assessment indicated that 56% adults of the Greater Geelong community are either overweight or obese. This indicates that about 90,000 adults in this community are either overweight or obese (Health Together Geelong, 2014). The overweight and obesity is higher in adult females than males Greater Geelong. The demographic pattern indicates that unhealthy weight is most common in the suburbs as compared with that from central Geelong. This is attributed to factors such as poor infrastructures that can facilitate transportation of fresh foods outlets to these regions (Health Together Geelong, 2014).
Additionally, the issue of overweight and obesity are lower in areas where the socio-economic status is low, especially in areas such as Norlane, Whittington, and Corio. However, the obesity and overweight incidence rates are higher in suburbs with higher SES. However, when evaluated separately, it was found that the levels of obesity are high in both high and low SES. Notably, evaluating the impacts of overweight and obesity can mask the differences that prevail between SES (Health Together Geelong, 2014). Thus, obesity is linked with low SES whereas overweight is associated with high SES. Moreover, it was found that the Greater Geelong community dietary programs are unhealthy. From the assessment, only 7.1% of the adults feed on the recommended levels of vegetables and fruits. The data suggested that less than 6,000 people met the requirement of the appropriate dietary requirements (Hamer et al., 2014). Additionally, a higher proportion of the population of the Greater Geelong community engaged in other risky behaviors such as tobacco use and consumption of alcohol. These risky behaviors reduced the ability of the individuals to remain physically active or even to observe their recommended nutrition requirements (Adair et al., 2013).
Impact of health conditions on communities
The impact of these health conditions mentioned above included high rates of obesity and overweight across the Greater Geelong community. The assessment indicated that approximately 56% of people aged 18 years and above is overweight or obese. The analysis also indicated that overweight and obesity rates for males in the Greater Geelong were higher than other states and that the rates had increased by 4 % within a period of 4 years. The trends were similar in females, but the rates had decreased by 5% among the females. Poor feeding habits, particularly poor intake of food and fruits is ranked among the top ten risk factors that would lead to global mortality rates (Health Together Geelong, 2014).
Other impacts identified from the analysis include psychological distress where 59.2% of the populations are diagnosed with psychological distress associated with obesity and overweight. This contributes to high alcohol consumptions among obese and overweight individuals, where the average percentage of adults consuming alcohol is reported at 52.4%. Other possible complications include an increased burden of cardiovascular, diabetes type 2, cancer, orthopedic, renal failure, and disability rates (Grundmann et al., 2013). The economic impact of obesity and overweight in Greater Geelong counties cannot be overlooked, with over $1.3 million being consumed efforts, and programs aimed at intervening on the risk factors that contribute to increased obesity and overweight prevalence’s.
Social determinants of health complications in the society
The health and well being of Geelong community is influenced by the population interactions with their social, economic and physical environments, which vary across the geographic locations and ages (Tamura et al., 2014). These determinants are varying according to the development stages i.e. infancy, childhood, adolescence, and childhood. Social determinant has a great impact on population health (Xiao- Hui, Et al., 2014). It is vital to understand these factors so that they can be applied during decision making on the interventions that can be used to advocate for certain issues and policies (Reiner et al., 2014).
One of the social determinants that influence obesity and overweight in Greater Geelong is poverty. This influences the ability for the population to access basic resources such as shelter, food and other social amenities (Wasenius, et al., 2014). People living in the suburbs have the highest level of obesity because of the high rates of unemployment, limited infrastructure and poor environment. The issue of poverty also influences behavioral problems, where low SES is found to engage in substance use such as alcohol and tobacco use (Zbigniew Et al., 2013). Low SES is also associated with increased psychosocial disorders such as depression and anxiety. Economic equality i.e. the gap between the rich and the poor in the region is high. Social status is associated with the determinants of people’s health where those with less social standing are twice more likely to be obese and overweight than those with higher social standing. This observation is across the society strata i.e. rich or poor (Ryan et al., 2014).
The psychosocial circumstances are associated with obesity and overweight. Society with prolonged anxiety, self esteem, social isolation, insecurity and reduced control of individual’s lives has tremendous effects on a person’s life (Brazeau, A.S., Et al., 2012). Individuals that are stressed are more prone to health complications such as diabetes type 2, heart attack, stroke, aggression and depression (Hu et al., 2010). The foundations of health care and education in early life is also a social indicator of health. Poor development of a child from the fetus stage is associated with high risks of obesity and is more common in low-income households that high-income households (Kaizu et al., 2014). Research indicates that infant development stage and early childhood stages are critical stages that are very vulnerable during their physical, mental and emotional changes (Miriam et al., 2012). For instance, an obese child could with insecure emotions and reduced stimulation level is associated with poor academic achievements (Heather et al., 2012).
Health programs and recommendations for obesity
Healthy Together Geelong (HTG) is the health program utilized by the Greater Geelong community to address the aforementioned key healthcare challenges. This program is jointly funded by the state government and the Australian government in a National partnership agreement preventive Health (NPAPH). This is a partnership between the city of Greater Geelong, Bellarine community and Barwon Health. HTG is working in these partnerships to ensure that their objective of reducing the increase of chronic diseases is achieved; and that there is a lasting improvement in the community health and their wellbeing.
HTG is funded by the state government, where $5.25 M has been saved is the period from 2011 to 2015. The programs have recruited 12 highly experienced individuals, which plan and implement strategies where Geelong community can learn (Marquis et al., 2014). The main challenge is that the funding seems to be rather inadequate to address these community challenges and to fully support programs that support services that will support future local health preventive programs. Additionally, there is no outlined mechanism to achieve their outcome (Blomster et al., 2013). There is a need for exact policies and strategies geared towards achieving their goal of reducing obesity by 5.5 %. These strategies include measures such as subsidizing organic food, improving infrastructure and social amenities to ensure a healthy lifestyle (Brumby et al., 2013).
Impact of Community Health Assessments Conclusion
The papers have described the needs required by the Greater Geelong community to address key lifestyle issues that are related to obesity and overweight. Therefore, it can be concluded that the high quality of health care should address the aforementioned inadequacies. The interventions should establish effective intellectual and social stimulation to promote the cognitive development of the Greater Geelong community. This is because good health habits are associated with appropriate dietary, sensible and regular exercises, which in turn are regulated by positive aforementioned social determinants including improved economic equality, education program, reduced poverty levels and improvement of the community social status.
Impact of Community Health Assessments References
Adair, L.S., Et al. (2013). The emergence of cardio-metabolic disease risk in Chinese children and adults: consequences of changes in diets, physical activity and obesity. Obesity reviews 15; 1, 49-59
Brazeau, A.S., Et al. (2012). Physical activity level and body composition among adults with type1 diabetes. Diabetic medicine 28, 402-408
Brumby, S., Et al. (2013). The effect of physical activity on psychological distress, cortisol, and obesity: results of the farming fit intervention program. BMC Public Health 13; 1018
Blomster, J.I. (2013). The influence of physical activity on vascular complications and mortality in patients with type 2 diabetes mellitus. Diabetes, obesity and metabolism 15; 11, 1008-1012
Dickie, K., Et al (2014). Meeting physical activity guidelines associated with reduced risk for cardiovascular disease in black south African Women; a 5.5year follow up. BMC Public Health 14; 498
Grundmann, N., Et al. (2014). Area deprivation and the prevalence of type 2 diabetes and obesity: analysis at the municipality level in Germany. BMC public health 14, 1264
Hamer, M., Et al. (2014). Watching a sport on television, physical activity and risk of obesity in older adults. BMC Public Health 14; 10
Health Together Geelong, (2014). Greater Geelong Community Health Needs Assessment, 2014. Retrieved from https://www.geelongaustralia.com.au/common/public/documents/8d1e825ea369b3e-Health%20Needs%20Assessment%202014%20PDF.pdf
Heather, J.A., Et al, (2012). An evaluation of the physical activity and health status of British Columbian Aboriginal populations. Appl. Physiol. Nutr. Metab. 37; 127-137
Hu, J., Et al. (2010). Physical activity, obesity, nutritional Health and quality of life in Low income Hispanic adults with diabetes. Journal of community Health nursing 27; 70-83
Jimenez-Pavon, D. (2013). Physical activity and markers of insulin resistance in adolescents: role of cardiorespiratory fitness levels- the HELENA study. Pediatric Diabetes 14; 249-258
Kaizu, S., Et al. (2014). Impact of leisure-time physical activity on glycemic control and cardiovascular risk factors in Japanese patients with Type 2 diabetes mellitus: the Fukuoka Diabetes registry. PLoSONE 9; 6, 98768-98778
Marquis, H., Et al. (2014). Impact of an exercise intervention on physical activity during pregnancy: the behaviors affecting baby and you study. American journal of public health 104; 10, 74-83
Miriam, C., Et al. (2012). Enhanced fitness: A randomized controlled trial of the effects of home-based physical activity counseling on Glycemic control in older adults with pre-diabetes mellitus. The American Geriatrics society60; 9, 1655-1665
Reiner, M., Et al. (2013). Long term health benefits of physical activity- a systematic review of longitudinal studies. BMC Public Health 13; 813
Ryan, J.M., Et al. (2014). Reduced moderate to vigorous physical activity and increased sedentary behavior associated with elevated blood pressure values in children with cerebral Plasy. Physical Therapy 94; 8, 1144-1154
Tamura, K., Et al. (2014). Spatial clustering of physical activity and obesity in relation to build environment factors among older women in three U.S. States. BMC Public Health 14:1322
Wasenius, N., Et al. (2014). The effect of structured exercise interventions on intensity and Volume of total physical activity. Journal of Sport Science and Medicine 13; 829-835
Xiao- Hui, L., Et al. (2014). Effectiveness of a school based physical activity intervention on obesity in school children: a non-randomized controlled trial. BMC Public Health 14; 1282
Zbigniew, K., Et al. (2013). Effects of physical activity on carbohydrate and lipid metabolism in women with abdominal obesity. Trends in sport Science 3; 20, 153-156
Falls Prevention Key Safety and Quality in Healthcare Order Instructions: For this paper, we are to choose a nursing issue that is related to one of the key safety and quality in health care areas.
Falls Prevention Key Safety and Quality in Healthcare
The chosen issue is FALLS PREVENTION; Preventing falls and harms from falls in older people. we need to use (5)five primary and/or secondary peer-reviewed articles/studies related to the chosen issue above and summarise, analyze and critique the literature related to this issue. The following criteria must be successfully addressed; Section 1(statement of the issue addressed, this includes an introduction, background to the issues and importance of the issue). Section 2(Critique the literature, this includes rigorous critical appraisal of the study designs and methods, which studies were more rigorous and why the description of the critical appraisal tool used and why it was the chosen tool. we are to go with the CASP tools.
finally Section 3(Findings) this includes presenting individual study findings as well as being able to synthesize (compare and contrasting)the study findings.
Falls Prevention Key Safety and Quality in Healthcare Sample Answer
Falls Prevention
Falls result in physical injury to patients. At times, the injuries could be severe necessitating hospitalization or even causing death. The elderly have a higher predisposition to falls than their younger counterparts. As people age, their mobility diminishes and when accompanied by events such as deteriorating eyesight, people get an elevated risk of falls and physical injuries (Zhang, Shuai, & Li, 2015). So as to prevent falls, it is necessary to first assess the level of risk that people have to the occurrence. Measures that would prevent falls would be addressing and resolving factors that predispose people to falls. In most cases, interventions work best when they address baseline risk factors.
Falls Prevention Key Safety and Quality in Healthcare Background
The prevention of injury has been a challenge in the care of elderly patients. It is common for old people to experience unintentional falls though most of them are nonfatal (Rosen, Mack, & Noonan, 2013, Pg. 61). Hospitalized elderly patients face a high risk for falls. The state of being ill coupled with the effects of treatment and the unfamiliarity of the environment are the major reasons for the high predisposition of hospitalized patients to falls (Dykes, Carroll, Hurley, Lipsitz, Benoit, Chang, & Middleton, 2010, Pg. 1912). Patients who fall are more likely to experience subsequent falls than those who do not (Leavy, Byberg, Michaëlsson, Melhus, & Åberg, 2015). Patients develop the fear of falling and end up limiting their movement and losing their mobility (Dykes et al., 2010, Pg. 1912). Falls have their associated financial losses in addition to health complications. For instance, there would be a need for extra treatment, and patients may have to stay longer in hospitals hence raising the cost of their care. Previously, people did not address falls as clinical problems worth much space in discussions. Increased awareness that there are significant severe consequences of falls has motivated the emergence of falls prevention programs. Such programs offer suggestions to practices that would minimize the occurrence of falls in high-risk groups (Child, Goodwin, Garside, Jones-Hughes, Boddy, & Stein, 2012).
Importance of Exploring Falls Prevention among Old People
There is significant data indicating that falls are common occurrences among the elderly (Child et al., 2012). On a yearly basis, a third of people aged sixty-five years and above experience at least an instance of a fall (Child et al., 2012). Again, though some programs have initiated various preventive measures, they do not depict the expected results due to various hindrances (Child et al., 2012). It would be important to research on the matter and give a satisfactory response regarding the established and novel methods of preventing falls. The issue is also necessary in the clinical setup considering its broad range of impacts. People may get long-term pain, lose the functionality of their organs, require admission in a care home, and incur financial losses (El-Khoury, Cassou, Charles, & Dargent-Molina, 2013). Exploring preventive measures of falls would be important as it would also facilitate the minimization of the associated undesirable effects of falls.
Falls Prevention Key Safety and Quality in Healthcare Literature Critique
There has been extensive research on falls prevention especially among elderly patients. Some of the studies employed clustered randomized trials where participants were from different settings (Dyke et al., Pg. 1912). Such studies were appropriately described and they had such aims as determining how effectively measures such as health information technology reduced falls in hospital settings. There were also secondary sources that incorporated literature review as their primary sources of data. Such studies had objectives such as that of informing clinicians on practical evidence-based solutions to fall prevention among the aged (Al-Aama, 2011, Pg. 771). The method of research applied fitted the study purpose as it involved reviewing studies to establish practices that reduced the occurrence of falls among the elderly hence being excellent choices for clinicians. The method also allowed the researcher to explore multiple aspects of falls simultaneously. The scientists referred to literature when addressing the pathophysiology of falls, its risk factors, screening and assessment, prevention, as well as its treatment (Al-Aama, 2011). The findings were particularly vital for clinicians.
There were also studies that employed systematic review in their design (Bloch, Thibaud, Dugué, Brèque, Rigaud, & Kemoun, 2010). Studies that employed the technique had objectives such as determining the effectiveness of fall prevention strategies in preventing the occurrence of injuries that result from the falls (El-Khoury et al., 2013). Systematic review studies extracted articles from authoritative databases such as CINAHL, Cochrane library and EMBASE. The studies exploited the most appropriate methods of data synthesis to critique their sources (El-Khoury et al., 2013).
There were secondary sources that focused on the causes of falls. Some of the studies employed a systematic review and referred to previous research studies to generate their conclusions. Such studies were motivated by a high occurrence of falls and its related injuries among other factors. Research indicated that drugs used by patients posed a significant threat to the development of falls in patients (De Jong, Van der Elst, & Hartholt, 2013, Pg. 147). The researcher purposed to examine the epidemiology, risk factors, and treatment strategies (De Jong, Van der Elst, & Hartholt, 2013).
CASP tools served as appropriate approaches to critiquing literature concerning various subjects on fall prevention that researchers had investigated. The tools addressed studies such as randomized trials, systematic reviews, and qualitative studies (CASP, 2013). Different checklists matched the design of research that researchers had applied.
Falls Prevention Key Safety and Quality in Healthcare Findings
Studies offered varied interventions to falls and their associated injuries. Researchers found that people subjected to falls had to embrace the new technology as it led to reduced risks for falls. They found the healthcare demands for falls patients to be above 30% higher than in other patients (De Jong, Van der Elst, & Hartholt, 2013, Pg. 148). The research gave informed discussions of treatment approaches and found them to be active in reducing the impact of injuries resulting from falls. There were also other studies discussing treatment approaches to the problem. The strategies included the use of medications that focused on the etiology of the falls. Cardiac arrhythmias and orthostatic hypotension were examples of conditions whose treatment reduced the risk of falls (Ungar, Rafanelli, Iacomelli, Brunetti, Ceccofiglio, Tesi, & Marchionni, 2013, Pg. 93). Studies that explored the effectiveness of preventive measures found the tools to cause a significant reduction in the cases of falls compared to their absence in management. The results implied that physicians should apply the preventive tool kits so as to lower the risk of falls for their patients (Dykes et al., 2010, Pg. 1912). In the determination of practices that lowered the risk of falls among patients, researchers identified exercises as a crucial factor (Burton, Cavalheri, Adams, Oakley Browne, Bovery-Spencer, Fenton, & Hill, 2015). In the studies concerning barriers to the implementation of preventive strategies, researchers found the process of applying preventive measures to be multifactorial and demanding critical considerations (Child et al., 2012).
Falls Prevention Key Safety and Quality in Healthcare References
Al-Aama, T. (2011). Falls in the elderly: Spectrum and prevention. Canadian Family Physician, 57(7), 771–776.
Bloch, F., Thibaud, M., Dugué, B., Brèque, C., Rigaud, A., & Kemoun, G. (2010). Episodes of falling among elderly people: a systematic review and meta-analysis of social and demographic pre-disposing characteristics. Clinics, 65(9), 895–903. http://doi.org/10.1590/S1807-59322010000900013
Burton, E., Cavalheri, V., Adams, R., Oakley Browne, C., Bovery-Spencer, P., Fenton, A. M., … Hill, K. D. (2015). Effectiveness of exercise programs to reduce falls in older people with dementia living in the community: a systematic review and meta-analysis. Clinical Interventions in Aging, 10, 421–434. http://doi.org/10.2147/CIA.S71691
CASP. (2013). Critical Appraisal Skills Program. Retrieved from http://www.casp-uk.net/#!casp-tools-checklists/c18f8
Child, S., Goodwin, V., Garside, R., Jones-Hughes, T., Boddy, K., & Stein, K. (2012). Factors influencing the implementation of fall-prevention programmes: a systematic review and synthesis of qualitative studies. Implementation Science : IS, 7, 91. http://doi.org/10.1186/1748-5908-7-91
De Jong, M. R., Van der Elst, M., & Hartholt, K. A. (2013). Drug-related falls in older patients: implicated drugs, consequences, and possible prevention strategies. Therapeutic Advances in Drug Safety, 4(4), 147–154. http://doi.org/10.1177/2042098613486829
Dykes, P. C., Carroll, D. L., Hurley, A., Lipsitz, S., Benoit, A., Chang, F., … Middleton, B. (2010). Fall Prevention in Acute Care Hospitals: A Randomized Trial. JAMA : The Journal of the American Medical Association, 304(17), 1912–1918. http://doi.org/10.1001/jama.2010.1567
El-Khoury, F., Cassou, B., Charles, M.-A., & Dargent-Molina, P. (2013). The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: systematic review and meta-analysis of randomised controlled trials. BMJ : British Medical Journal, 347, f6234. http://doi.org/10.1136/bmj.f6234
Leavy, B., Byberg, L., Michaëlsson, K., Melhus, H., & Åberg, A. C. (2015). The fall descriptions and health characteristics of older adults with hip fracture: a mixed methods study. BMC Geriatrics, 15, 40. http://doi.org/10.1186/s12877-015-0036-x
Rosen, T., Mack, K. A., & Noonan, R. K. (2013). Slipping and tripping: fall injuries in adults associated with rugs and carpets. Journal of Injury and Violence Research, 5(1), 61–69. http://doi.org/10.5249/jivr.v5i1.177
Ungar, A., Rafanelli, M., Iacomelli, I., Brunetti, M. A., Ceccofiglio, A., Tesi, F., & Marchionni, N. (2013). Fall prevention in the elderly. Clinical Cases in Mineral and Bone Metabolism, 10(2), 91–95.
Zhang, X.-Y., Shuai, J., & Li, L.-P. (2015). Vision and Relevant Risk Factor Interventions for Preventing Falls among Older People: A Network Meta-analysis. Scientific Reports, 5, 10559. http://doi.org/10.1038/srep10559
he M6A4: case study counts as 10% of your grade for this course.
We suggest that you develop and outline and use the following time-line as your guide for completing your paper:
Week 1: Review the requirements for the paper.
Week 2: Begin developing an outline for your paper.
Week 3: You should have your outline completed.
Week 4: You should be using your outline to write your paper.
Week 5: Continue work on your paper.
Week 6: Finalize your paper and submit by the end of the week.
Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page.
Information on using an outline and writing a scholarly paper is available through the Excelsior College Online Writing Lab (OWL).
If you have questions, reach out to your instructor via My Messages.
linked item M6A4: A Patient with Musculoskeletal Limitations Complicated by a Medical Illness
The Surgical Care Improvement Project (SCIP), was implemented as a commitment to improving the safety of surgical patients by reducing post-operative complications. Although some surgical complications are unavoidable, surgical care can be improved through better adherence to evidence based practice.
Case Study: A 60-year old patient with a long standing history of right knee pain has been diagnosed with osteoarthritis, and has been recommended a total left knee arthroscopy to improve chronic discomfort and improve mobility.
The patient’s past medical history includes hypertension and an irregular heart rate. The patient denies any allergies.
The patient reports to the hospital at 1 p.m. for a left knee replacement. A medication reconciliation is completed, and the patient reports taking the following medications with a sip of water at 8:00 p.m.:
• Lisinopril 10 mg PO daily
• Toprol 25 mg PO daily
• Celebrex 200 mg PO daily
While in the pre-operative holding area, vital signs are taken and are within normal limits. No hair removal was performed. The patient was ordered and received Ancef 1 gram IV mini bag, at 2:30 p.m. The patient was transferred to the operating room, where anesthesia monitoring began at 3:00 p.m., a urinary catheter was placed, and a forced air warming device was placed to maintain the patient’s temperature.
After recovering in the post anesthesia care unit (PACU), the patient was transferred to a surgical floor. Post-operative orders included:
• Ancef 1 gram IV mini bag every 8 hours
• Long leg TED hose and sequential compression stockings to right leg while in bed
• Lovenox 30 mg subcutaneously every morning, starting the following morning
• Urinary catheter to be discontinued at 3:00 p.m. on post-operative day 1
The patient progressed well, both with pain control and mobility. TED hose and sequential compression stockings were worn while in bed. On the first post-operative day, the first dose of Lovenox was administered at 1000 a.m. and the last dose of Ancef was received at 2:30 p.m. The patient was able to void after removal of the urinary catheter. The patient progressed well and was discharged home on post- operative day 5.
Evidence shows that more than 45 million operative procedures are performed in the United States each year. Approximately 40% of operative procedures result in a surgical complication. The Surgical Care Improvement Project (SCIP) was implemented to improve quality of care of surgical patients, by reducing surgical complications. Nurses play an important role in this process by following and adhering to evidence based and best practice protocols.
Using evidence based practice from two professional nursing journals, and/or your nursing textbooks, answer the following questions:
1. Explain one of the SCIP core measures, and how it has impacted the prevention of surgical complications. 2. Explain why no hair removal was required for the surgical procedure. If hair removal were ordered, explain the appropriate technique.
3. What methods were used to ensure that the recommended VTE/DVT prophylaxis was implemented, and why is the timing important? Explain your rationale with evidence.
Using APA format, write a two (2) to three (3) page paper (excluding the cover and reference page) that addresses the case study. A minimum of two (2) current professional references must be provided. Current references include professional nursing publications dated within five (5) years, and/or a textbook(s) used for the course that is no more than one (1) edition old. Websites are not to be used as professional resources or references.
Compose your work using a word processor (or other software as appropriate) and save it frequently to your computer. Use a 12 font size, double space your work and use APA format for citations, references, and overall format. Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page. Assistance with APA format, grammar, and avoiding plagiarism is available for free through the Excelsior College Online Writing Lab (OWL). Be sure to check your work and correct any spelling or grammatical errors before you submit your assignment.
You are required to submit your paper to Turnitin (a plagiarism prevention service) prior to submitting the paper in the course submission area for grading. Access is provided by email to the email address on record in your MyExcelsior account during week 2 of the term. Once you submit your paper to Turnitin check your inbox in Turnitin for the results. After viewing your originality report correct the areas of your paper that warrant attention. You can re-submit your paper to Turnitin after 24-hours and continue to re-submit until the results are acceptable. Acceptable ranges include a cumulative total of less than 15% for your entire paper, and no particular area greater than 2% (excluding direct quotes and/or references).
See the videos below for instructions on how to submit your paper to Turnitin and view your Originality Report.
Video – Submitting a Paper
Video – Viewing Your Originality Report
When you’re ready to submit your work for grading, click Browse My Computer and find your file. Once you’ve located your file click Open and, if successful, the file name will appear under the Attached files heading. Scroll to the bottom of the page, click Submit and you’re done.
This activity will be assessed according to the NUR213 M6A4: Case Study Rubric.
SAMPLE ANSWER
Improvement of Surgical Care
Project Outline
Week 1
In the first week, the learner will focus on understanding the requirement of the paper. The student will understand the presented case scenario and get ready to research on various concepts as the study topic would suggest. The learner will seek clarification from the instructor on areas that may not be clear. So as to acquire all the necessary information, the learner will refer to reliable sources and build up a strong background regarding the study topic. The researcher will figure out the requirements of the paper and purpose to include all vital concepts in the project. The student will design appropriate approaches of answering the questions presented in the paper. Also, the learner will purpose to apply evidence-based techniques to the project. By the end of the week, the researcher will have a comprehensive understanding of the requirements of the paper.
Week 2
The student will start developing an outline of the paper by the second week. The outline should satisfy the requirements of the paper. The learner will set objectives that would be achieved within a given period. The learner will ensure that the objectives are measurable, strategic, applicable, and that they are reliable. The outline should include the major activities that the leaner would engage in. As such, the learner will refer to the outline and the tool will serve the purpose of a reminder. The outline will be set in a way that the completion of a particular task would facilitate that of subsequent ones. The researcher will establish the outline in a way that would be easy to develop it and make changes where necessary. The initial components of the outline will incorporate introductory concepts to the study project.
Week 3
The learner will complete the outline in the third week. The completed outline will serve as a guide in addressing the study problem. The researcher will use the outline to assess different issues and make independent judgments. The outline will summarize the requirements of the paper and match their expected time of completion. The learner will focus on addressing the entries in the outline and make achievements within the specified time. The outline will be organized in such a way that it would be possible to address the requirements of the project strategically. The learner will purpose to apply the completed outline to the presented case study. By the time of completing the outline, the learner will have understood most of the concepts included in the project. The format of the paper will match that of the completed outline both in its arrangement and content.
Week 4
By the fourth week, the learner will start writing the paper while referring to the outline. The student will meet the objectives of the outline when addressing the issues highlighted in the case study. By the fourth week, the learner will have addressed about the first third of the requirements included in the outline. The student will refer to scholarly work when researching the issues highlighted in the timeline. The paper will address various concepts exhaustively and include authoritative references so that readers can easily validate the writer’s strong assertions. The paper will be well-organized and its presentation will be friendly to readers. The concepts addressed in the first part of the paper will later be applied to subsequent parts so that the entire paper will be coherent. Having questions thoroughly addressed will facilitate the handling of subsequent issues in the outline.
Week 5
The learner will continue applying the outline to address issues included in it. By the end of the week, the researcher will have handled about two thirds of the paper. The learner will interlink the topics of week four with those of week five so that the paper would have a high degree of consistency. The student will address the requirements of the paper in such a way that the paper interlinks with the case study and it meets the objectives included in the outline. The paper will reflect a scholarly structure in its organization and format. Concepts addressed in week five will apply to the subsequent week, and it would be necessary to make validated assertions. The student will ensure that the paper maintains high quality mainly by enhancing its consistency with the outline and the case study.
Week 6
It will be the last week of the paper, and the learner will complete the remaining part of the task. The student will merge different sections of the paper so that they are in a presentable format. The learner will go through the whole paper and ensure that it is coherent from the beginning. The student will correct any errors that may have occurred and ensure that the general presentation of concepts meets scholarly standards. The learner will make a summary of the addressed issues since the first week to the sixth. The summary will be tied to the outline developed at the beginning of the project. The researcher will also make a conclusion at the end of the paper regarding the studied topic. The researcher will then present the paper to the instructor for marking.
Improvement of Surgical Care
Care for the patient in the case study was directed toward the prevention of acquisition of surgical site infections. The involved health professional was directed by the guidelines of Surgical Care Improvement Project (SCIP). Some of the practices performed were the core measures advocated by SCIP (Weston, Caldera, & Doron, 2013).
Core Measure: the Prophylactic Administration of an Antibiotic Medication within an Hour to Surgical Operation
The patient in the case study received a dose of intravenous cefazolin (Ancef) prior to undergoing the operation. The drug is a cephalosporin and it works against a wide range of bacteria. Therefore, the medication would protect the patient from acquiring bacterial infections that would be most possible when bacterial colonies get into contact with open surgical wounds. SCIP measures recommend the application of antimicrobial medications at most an hour to the first incision or performance of surgery. The early administration of the agent gives it enough time to establish and attain a bactericidal serum concentration by the time of the operation (Goede, Lovely, Thompson, & Cima, 2013, Pg. 563). Untimely application of prophylactic antimicrobials would raise the risk of patients acquiring nosocomial infections regardless of whether they receive the medication or not (Turk, Karagulle, Serefhanoglu, Turan, & Moray, 2013, Pg. 583). Studies relate longer time durations between antibiotic treatment and the beginning of surgery to a high likelihood of acquiring bacterial infections.
The practice had beneficial yields as the patient did not report complications after the operation (Weston, Caldera, & Doron, 2013). In addition to promoting patient safety, the move was also important in upholding hospital guidelines of standard care. Guidelines specifying the procedural activities involved and the specific antimicrobials for use would promote the development of a healthy culture in the healthcare institution (Wang, Chen, Ward, & Bhattacharyya, 2012).
The Basis for Avoiding Hair Removal during the Operation
Hair removal is not always necessary when performing a surgical operation (Poggio, 2013, Pg. 171). There is substantial scientific evidence against hair removal under certain circumstances. Previously, the activity was understood to improve hygiene at the surgical site hence protecting patients from infections. Later understandings revealed possibilities that the practice predisposed people to disease infections (Poggio, 2013, Pg. 171). Usually, hair removal creates an avenue for the entry of bacteria into the body. Bacteria get entry into the body through abrasions and microscopic nicks created after hair removal. It was necessary to avoid the practice so as to maintain the integrity of the patient’s skin and promote his safety.
Had hair removal been ordered, it would have been necessary to perform it in the safest way possible. The practice should have been performed in a way that it does not create abrasions that would later be the entry points of bacteria into the body. The practitioner would have considered shaving the surgical site approximately twelve hours to the operation rather than just before it. The clinician would also have used electric clippers rather than manually operated shaving razors (Crolla, van der Laan, Veen, Hendriks, van Schendel, & Kluytmans, 2012). Clippers are not as much likely to cause many tears as razors would have resulted. Other reasons for the selection of electrical clippers at the expense of the manually operated ones include patients would not experience razor burns, and instead, the method would leave hair stubbles on the skin surface. It is conclusive that use of electric clippers would place patients at reduced risks of infections than would have been the case had manual razors been the choice.
Methods that Ensured the Implementation of VTE/DVT Prophylaxis
There are several practices in the case study involving the prevention of deep vein thrombosis and venous thromboembolism. They include the use of compression stockings as approaches to preventing DVT and VTE. The TED hose applied on the patient in the case scenario prevent the occurrence of DVT by facilitating venous blood flow and lymphatic drainage in the legs of the patients. The stockings would work best when patients are lying as in the case study. Usually, the stockings are supposed to compress blood vessels from the ankle up the legs to facilitate the return of blood to the heart. They therefore overcome the risk of developing DVT whose pathophysiology entails poor blood flow to the lower limbs, blood pooling, and the eventual formation of emboli. Compression stockings are usually made of elastic material and fiber and clinicians should ensure that they recommend the use of compressional stockings of the appropriate strength.
There were also pharmacological approaches applied to prevent the two complications in patients. Lovenox is an effective medication in the prevention and management of DVT (Pannucci, Wachtman, Dreszer, Bailey, Portschy, Hamill, & Wilkins, 2012, Pg. 165). The agent prevents the formation of blood clots and so emboli. It was necessary to administer the drug to the patient as surgical patients have a high predisposition to the development of blood clots and embolism. Before administering lovenox, prescribers should first assess the patient for indications suggesting that they have a low count of platelets. 2the use of the drug in such patients could have severe adversities such as prolonged bleeding. The drug works well in patients undergoing surgical treatment and its use in the case study was appropriate.
References
Crolla, R. M. P. H., van der Laan, L., Veen, E. J., Hendriks, Y., van Schendel, C., & Kluytmans, J. (2012). Reduction of Surgical Site Infections after Implementation of a Bundle of Care. PLoS ONE, 7(9), e44599. http://doi.org/10.1371/journal.pone.0044599
Goede, W. J., Lovely, J. K., Thompson, R. L., & Cima, R. R. (2013). Assessment of Prophylactic Antibiotic Use in Patients with Surgical Site Infections. Hospital Pharmacy, 48(7), 560–567. http://doi.org/10.1310/hpj4807-560
Pannucci, C. J., Wachtman, C. F., Dreszer, G., Bailey, S. H., Portschy, P. R., Hamill, J. B., … Wilkins, E. G. (2012). The effect of post-operative enoxaparin on risk for re-operative hematoma. Plastic and Reconstructive Surgery, 129(1), 160–168. http://doi.org/10.1097/PRS.0b013e318236215c
Poggio, J. L. (2013). Perioperative Strategies to Prevent Surgical-Site Infection. Clinics in Colon and Rectal Surgery, 26(3), 168–173. http://doi.org/10.1055/s-0033-1351133
Turk, E., Karagulle, E., Serefhanoglu, K., Turan, H., & Moray, G. (2013). Effect of Cefazolin Prophylaxis on Postoperative Infectious Complications in Elective Laparoscopic Cholecystectomy: A Prospective Randomized Study. Iranian Red Crescent Medical Journal, 15(7), 581–586. http://doi.org/10.5812/ircmj.11111
Wang, Z., Chen, F., Ward, M., & Bhattacharyya, T. (2012). Compliance with Surgical Care Improvement Project Measures and Hospital-Associated Infections Following Hip Arthroplasty. The Journal of Bone and Joint Surgery. American Volume, 94(15), 1359–1366. http://doi.org/10.2106/JBJS.K.00911
Weston, A., Caldera, K., & Doron, S. (2013). Surgical Care Improvement Project in the Value-Based Purchasing Era: More Harm Than Good? Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America, 56(3), 424–427. http://doi.org/10.1093/cid/cis940
We can write this or a similar paper for you! Simply fill the order form!
What Are the Social Reasons for Class Differences in Health?
Order Instructions:
In this regard, it would be useful to discuss several different (social) explanations of health inequality that sociologists have put forward to explain health differences on the basis of social class.
Then use some examples to explore class differences in health – you will find empirical examples in the John Germov chapter from ‘John Germov (ed.) 2014, Second opinion, 5th edn, Oxford University Press, South Melbourne’. which you can follow-up the original references, Social Science & Medicine is especially useful for articles on class differences in health and illness.
SAMPLE ANSWER
Social Reasons for Class Differences in Health
What Are the Social Reasons for Class Differences in Health?
Introduction
Health disparity based on class difference is a phenomenon that remains prevalent, despite improvement in health provision over the years. Studies have indicated differences in health aspects among different classes, including life expectancy, maternal and infant mortality as well as the general aspects of health. This result from characteristics within different classes based on wealth, status, employment, background and culture. It can therefore be concluded that an individual’s social class plays an important role in impacting their physical health and access to medical care, which in effect determines their life expectancy. This paper is a discussion of the social reasons surrounding differences in health based on class.
Discussion
Socioeconomic factors
A majority of explanations on health disparities lean towards the socioeconomic or ‘material’ explanation and this has been identified as the major determining factor in health care access among individuals. Researchers argue that poverty, low health resources, poor living standards and housing and high risk occupations among other material factors are responsible for the poor state of health in lower classes. This could explain why life expectancy is significantly different between the rich and poor. Ullits, et al (2015, p. 2) note that people in lower socioeconomic quartiles often experience greater levels of health problems. They are not in a position to access regular health care and when they do, it is often of lower quality. Pais (2014, p. 1732-33) also notes that children from low income households are more likely to accumulate adverse health conditions as they grow older; thus leading to lower life expectancy. This is unlike children from richer backgrounds who have access to quality health, including regular check-ups, access to medication and preventive measures. In a study of social factors influencing TB infection, poverty is rated among the main causes. Infection rate is higher among the poor because they are more likely to live in overcrowded and poorly ventilated areas. In addition, they more disadvantaged as far as accessing health care and treatment are concerned (Hargreaves, et al, 2011, p. 655). Socioeconomic factors therefore influence differences in health based on access to health and quality of health.
Health literacy
Education and health literacy play an important role in health seeking behavior and are therefore considered social health determinants. The higher the level of education, the more an individual is capable of making decisions about their health and this consequently influence their well-being. Educated people are more likely to have knowledge on various issues as well as diseases and thus able to determine when they need to seek medical intervention (Prins, E, & Mooney, 2014, p. 25). They are also more aware of health risks that could affect them and are therefore more likely to take preventive measures, compared to their uneducated counterparts. The level of education also determines an individual’s socioeconomic level, mostly because employment and wages are based on the level of education. This means that individuals with lower levels of education are less likely to have well-paying jobs, adequate to cater for their health needs, unlike educated individuals who are likely to have white collar jobs. Burgard and Lin (2013, p. 1108)makes the same observation, noting that the lower class citizens often have less education and thus undertake jobs that have little or no health benefits. Such jobs are also likely to be more risky, hence exposing them to injuries. This differs from middle and higher class individuals who are more likely to enjoy medical insurance for themselves and their families; hence creating a significant difference in health status.
Health literacy differs across social classes and demographics as identified by Prins and Mooney (2014, p. 27). Based on income, groups earning lower income have low health literacy (LHL) compared to higher income earners. Adults with high school education and above have better health literacy than those with education below high school. In terms of race and ethnicity, minority groups are known to have significantly lower health literacy skills compared to whites. Age also determines literacy level and research indicates that adults aged 65 and above have lower health literacy than younger individuals. These demographic characteristics signify that health differences are largely influenced by social factors. This in turn influences health seeking behavior, in that, the higher the health literacy, the more likely an individual is likely to identify disease signs, seek treatment or take preventive measures. In essence, the quality of life and health status would depend on an individual’s health literacy level and the various demographic factors play a major role in determining health literacy (Prins and Mooney, 2014, p. 25-27).
Cultural factors
Cultural differences are also associated with health variation. Khanna, Kaushik and Kaur (2012, p. 50-51) individuals in lower classes may have preference for less healthy lifestyles and are likely to eat more unhealthy foods and exercise less as opposed to those in high and middle class. This may be attributed to lack of enough money to buy healthy food or due to lack of knowledge on healthy living. Khanna, Kaushik and Kaur (2012, p. 50) in another view explain that people who work in offices are more likely to suffer from lifestyle diseases because of their inactive lifestyles. Their schedule revolves around reporting to work early in the morning, working while seated most of the day and going home in the evening to rest. Despite eating during the day and at night, they rarely have enough time to exercise. In addition, they are more likely to eat unhealthy because they barely have time to cook, such that they turn to fast food for quick meals.
Nature of employment
A closer look at forms of employment indicates that working conditions contribute to disparities in health. Burgard and Lin (2013, p. 1107) notes that social factors within the work environment may influence exposure to various health risks and thus disparities in health. These may include both physical and psychosocial factors. Physical risks including exposure to harmful radiation, heights, dangerous machines and poisonous chemicals for example, means that, an individual is more likely to face a health risk. On the other hand, individuals working in offices have less exposure to occupational risks, giving them an upper hand in terms of health. Depending on the working conditions, employees may benefit from various types of benefits at work, such as medical cover. This means that individuals with high status job benefits are more likely to access quality medical care than those working in poor employment backgrounds (Burgard and Lin, 2013, p. 1112). Lastly, psychosocial factors including stress at work and perceived job insecurity among others may affect an individual’s health status. People in more secure jobs are known to have lower stress levels as opposed to individuals with low job security, hence better mental stability.
Social status
Status and power are a major cause of health inequity. Ullits, et al (2015, p. 4) argue that depending on one’s position in the society, the availability of health services is likely to differ. Individuals who are highly placed in the society are likely to access better health services than those in lower ranks or ordinary citizens because they are more likely to command respect in any setting in the society and are more likely to be endowed financially. This however goes beyond availability of money because a highly placed individual can easily access health services during an emergency, with the promise of paying later; yet an individual with no status in the society may find it difficult to access health care without finances. The possibility of a highly placed individual finding sponsors, to supplement hospital bills is also higher than for a person who is barely known. This explains why people with higher social status can afford to seek the highest level of medical care, even travelling abroad to treat chronic diseases which would otherwise kill a common citizen due to lack of finances and quality health care.
Minority status
It is generally observable that race and ethnicity can influence the access to quality health. Shepherd and Zubrick (2012, p. 108) note that minority groups tend to access lower quality health than native citizens, mostly because of lower income levels and low levels of education. Collins and Rocco (2014, p. 5-8) note that health disparities based on race are mostly influenced by labor force participation differences influenced by racial differences. These health differences are further exhibited by the association between employment and health. While low income restricts an individual’s access to quality health, low levels of education mean that an individual has low health literacy level and thus less likely to maintain health seeking behavior.
The disabled as a minority group, are considered to have higher health risks than normal individuals; a factor that creates a health difference between these groups. They are more prone to accidents and falls and this is particularly risky if they do not have an assistant. The fact that a disabled individual may not be able to go to a hospital unassisted also means that they are more disadvantaged, especially in emergency situations. Delays in accessing health care while waiting for a caregiver or assistant puts disabled persons at a higher health risk. In addition, most disabled individuals are not in a position to work or find employment in high level jobs, thus limiting their ability to obtain quality health services.
Gender differences
Gender is a health determinant and research has shown that males and females are exposed to different health risks. Men are known to take up more risky professions than women and this exposes them to a greater variety of health problems. Women on the other hand are more prone to psychological health factors than men, despite having a longer life expectancy (Malmusi, et al (2014, p. 1). The life expectancy among men may be influenced by biological differences, risk-taking behavior and health seeking behavior. In their research, Malmusi, et al (2014, p. 4) establish that women are disadvantaged in terms of access to the labor market and often end up with lower income than their male counterparts. This to a large extent explains inequality among genders in terms of health. It is also notable that different ailments are likely to affect one gender compared to the other, thus creating health differences. While women may be more prone to breast cancer for example, men have a lower risk and hence this is a major difference in health.
Environmental factors
The environment in which an individual lives, including their neighborhood can influence their health significantly. This explains why individuals living in deprived neighborhoods such as slums are likely to encounter more health risks than those living in up market residential areas. Hargreaves, et al (2011, p. 656) for example note that population density in congested urban residents to a significant extent exposes residents to higher risk of contracting tuberculosis. Bac, Andersen and Dokkedal (2015, p. 317) introduce the concept of self-rated health and study the role played by individuals’ neighborhoods in determining their self-rated health. The study which focuses on deprived neighborhoods concludes that individuals living in rural settings reported higher self-rated health position than those living in deprived neighborhoods in urban settings.
Conclusion
This discussion establishes that social class is directly correlated with health differences in the society. Socioeconomic class differences appear to take a central role in determining access to health, information and preventive measures. This is is because access to health, including quality health is determined by a prrson’s ability to pay. The rich are therefore likely to access better health services than the poor. Other parameters influence access to health including social class differences brought about by culture, race and ethnicity, age, gender, social status, education and health literacy and employment background among other factors. Each social factor is associated with a certain level of health disparity in terms of access, knowledge in health matters and quality of health individuals in a certain class can acquire. Despite government attempts to equate health care access, there will always be differences pegged on social class. It can therefore be concluded that social class plays an imperative role in explaining health disparities.
Burgard, S, & Lin, K 2013, ‘Bad Jobs, Bad Health? How Work and Working Conditions Contribute to Health Disparities’, American Behavioral Scientist, 57, 8, pp. 1105-1127, Professional Development Collection, EBSCOhost, viewed 29 September 2015. http://eds.a.ebscohost.com/ehost/detail/detail?sid=d89bc410-425d-4eae-93ba-
Hargreaves, J, Boccia, D, Evans, C, Adato, M, Petticrew, M, & Porter, J 2011, ‘The Social Determinants of Tuberculosis: From Evidence to Action’, American Journal Of Public Health, 101, 4, pp. 654-662, Professional Development Collection, EBSCOhost, viewed 29 September 2015.
Transitional Management for Adult Patients of Chronic Obstructive Pulmonary Disease (COPD)
Order Instructions:
Using APA format ,write six (6) to ten page paper (excludes covers and references pages) that addresses the disease management needed of adult patients with COPD for a safe transition between the acute care setting and home and the role of the interdisciplinary team in that transition.
SAMPLE ANSWER
Transitional Management for Adult Patients of COPD
Chronic Obstructive Pulmonary Disease (COPD) is an incurable medical condition that is more prevalent in older people than in the young. Even though COPD is incurable, it is possible to minimize the severity of its symptoms by structuring optimal management techniques. Such practices should minimize the rate of disease progress and offer patients a chance to lead high-quality lives. However, it is often challenging to ensure that patients receive optimal management for the disease, more so when they are leaving acute care centers for their homes. There are important approaches to consider in ensuring that patients practice the recommended strategies for managing COPD at their homes. The activity would involve an interdisciplinary collaboration between professionals in the healthcare setup.
Part 1: The Use of Bronchodilators and Corticosteroids in the Management of COPD
Why They are Used
Bronchodilators and corticosteroids are effective in the alleviation of clinical symptoms of COPD. Bronchodilators such as salmetrol, formoterol, and tiotropium work on a long-term basis to enhance lung functionality and reduce the occurrence and severity of exacerbations, hence improving patient’s quality of life. The drugs also enhance patient’s tolerance to exercises and improve protect them from lung hyperinflation as well as dyspnea (Tashkin, & Ferguson, 2013). Drugs such as indacaterol and aclidinium are new developments that require less dosage frequencies hence reducing chances of drug non-adherence among patients. Other bronchodilators with lengthy frequencies of intake include glycopyrrolate, vilanterol, and olodaterol (Tashkin, & Ferguson, 2013).
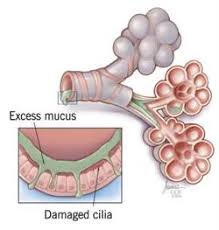
Corticosteroids are also important medications in the management of exacerbations experienced in COPD. Nebulized budesonide is not only a primary care corticosteroid in managing OCPD in adults, but it is also the drug of choice for children with COPD. Clinicians prefer the drug on the basis of its considerably less severe side effects compared to those associated with the use of other steroids (Gaude, & Nadagouda, 2010, Pg. 230). Timely administration of corticosteroids also results in improved functionality of the lungs. Some glucocorticoids also find use in reducing inflammation. They act by inhibiting the genetic pathway leading to the production of inflammatory mediators such as chemokines and cytokines (Gaude, & Nadagouda, 2010, Pg. 231). Instead, they promote the production of anti-inflammatory molecules such as beta-2 adrenoceptors. Through such a mechanism, glucocorticoids reduce swelling and exudation on the airway hence enhancing the respiratory system.
Side Effects of Corticosteroids and Bronchodilators
The use of corticosteroids has adverse effects such as sleep abnormalities, exaggerated appetite, and weight gain. They also subject adult users to ailments such as osteoporosis, diabetes, pneumonia, hypertension, cardiac anomalies, cataracts, and peptic ulcers (Gaude, & Nadagouda, 2010, Pg. 232). The side effects are severer when patient are on oral and parenteral treatment with corticosteroids as compared to when they take inhaled and nebulized formulations. The prevalence of the undesirable effects also increases with the dosage amount. Bronchodilators also have associated adversities. They include muscle crumps, headache, dizziness, nausea, vomiting, palpitations, and cardiac abnormalities (Cleveland Clinic, 2014a). Patients should report severe critical side effects so that prescribers can substitute their regimens with others that have minimal adversities. Occurrences such as hypertension, severe headaches, persistent vomiting are worth reporting as they may indicate the development of other critical conditions such as cardiac diseases and peptic ulcers. Patients may not have to report effects such as dizziness, nausea, and minor headaches as such complications are common with most medications. Besides, such symptoms are often temporary, and they would rarely indicate serious clinical adverse conditions.
Special Instructions Regarding Drug Use
Both bronchodilators and corticosteroids require special directions for their use. For instance, health professionals should advise their patient to take bronchodilators before taking other inhaled medications such as corticosteroids. Again, it is important to inform patients that they do not have to chew bronchodilator tablets, and instead, they should swallow them as whole. It is also necessary to inform patients on the purpose of each medication. For instance, patients should know that bronchodilators help them overcome shortness of breath associated with COPD. Some of the additional directions also apply to the use of corticosteroids. For instance, patients would always require taking bronchodilators first when they are co-administered with steroids. For corticosteroids, patients should know that they require rinsing their mouth with clean water to minimize the occurrence of side effects such as nausea. Also, it is important to inform the patient that unlike bronchodilators, corticosteroids take a considerably longer time to work, and they are not applicable for instant relief of COPD symptoms. Again, patients should know that corticosteroids may not stop attacks that have already started (Cleveland Clinic, 2014b).
An Important Healthcare Discipline that would Facilitate Medication Adherence
Medication adherence entails the degree of compliance with the recommended drug use practices. So as to ensure optimal treatment adherence among patients, various healthcare disciplines should collaborate. Among such disciplines are the nursing and pharmacy departments. Nurses have most interactions with patients as their primary role is to monitor patients. On the other hand, pharmacists are the custodians of drug use, and they would be relevant in promoting adherence to medications. Pharmacists should cooperate with nurses to schedule follow up activities to monitor drug use among patients (Jimmy, & Jose, 2011, Pg. 156). They should for instance establish strong interactions with patients, teach them on how to use devices such as inhalers, and monitor their use of adherence devices such as calendars and reminders.
Part 2: Dietary Modification in the Management of COPD
The Role of Diet in Managing COPD
Diet is a crucial consideration in the management of COPD. Either form of malnutrition, be it excessive nutrient consumption, or low intake of the same has an undesirable impact on the pathogenesis of COPD. Dieting habits that promote the development of conditions such as obesity have severe impact on COPD development. Usually, obesity leads to other respiratory abnormalities that worsen the condition of COPD patients. Such illnesses include asthma, hypoventilation, and pulmonary embolism (Hanson, Rutten, Wouters, & Rennard, 2014, Pg. 724). On the other hand, COPD patients with advanced disease experience pulmonary cachexia, a state in which their body weight is abnormally low, and their free fatty mass is extremely reduced.
Dietary modifications would be necessary to enhance the nutritional status of patients. Malnourished COPD patient would have to rely on dietary supplements to boost their health. Alternatively, patients would have to include high-calorie foods and beverages in their dietary plans. Studies indicate that lean COPD patients should maximize their fat intake at the expense of carbohydrates (Itoh, Tsuji, Nemoto, Nakamura, & Aoshiba, 2013, Pg. 1318). Some cultures encourage consumption of meat while others discourage it. Likewise, cultures have varying influences regarding intake of fruits and vegetables.
Possible Obstacles to Dietary Modification
Patients may find it hard to adopt new dietary practices. Also, people’s living conditions may influence their ability to adopt certain therapeutic dietary approaches. Patients from poor economic backgrounds may not access the recommended dietary practices. Cultural beliefs may also influence the adoption of dietary changes. Some cultures may not encourage certain recommended dietary approaches. Patients’ taste and preferences may also hinder the adoption of dietary changes. Some nutrients are only abundant in foods that some patients may be unwilling to take. Such foods include fish and mushrooms, both which are sources of vitamin D, an element crucial for COPD patients (Itoh et al., 2013, Pg. 1320).
An Important Healthcare Discipline in Facilitating Dietary Modifications
Nurses should seek the collaboration of dieticians in promoting effective dietary modifications. COPD patients experience important nutritional complications such as appetite loss. Medical dieticians are best placed to inform patients on practices that would promote their appetite. They should offer nutrition therapy to protect patients from weight loss and attacks by COPD Comorbidities (Seo, 2014, Pg. 151). Likewise, the professionals would advise obese persons on measures they should take to avoid worsening their health status. Dieticians should also collaborate with the families of patients by advising them on the foods that their patients may need as well as the ones they should avoid.
Part 3: Physical Activity in COPD Management
The Role of Physical Activity in COPD Management
While it is advisable for people to engage in physical exercises, COPD patients should maintain their level of involvement to a certain level. Too much strenuous activities may have adverse consequences in the population. The pathophysiology of COPD involves dyspnea, a condition that may worsen with engagement in exercises. Simple exercises are however necessary to ensure that patient’s respiratory system is strengthened. Energy conservation is crucial in COPD patients both in the sense that the victims could easily ran malnourished and also considering the appropriate management of dyspnea. Recommended physical exercises for the group include diaphragmatic and pursed-lip forms of breathing techniques (Broward Health, 2015). COPD patients also require physical exercises for psychological health. There are multiple factors that would predispose the group to stress, depression, and anxiety. The knowledge of having a chronic ailment is among such factors. Also, experiences of dyspnea and its associated discomfort would easily trigger anxiety. Patient would need keeping themselves busy through exercises so as to overcome such events.
The Role of RN in Promoting Effective Physical Practices in COPD Management
Registered nurses prioritize on the welfare of patients. They should structure an exercise strategy that would not harm but benefit patients. They would do so by warning patients against engagement in strenuous activities and advise them on appropriate activities they should explore. Nurses should also monitor the performance of their patients to help them maintain healthy physical conditions. Nurses should educate patients on activities that would promote their pulmonary system. Such advice should also entail practices that patients should engage in so as to overcome symptoms such as dyspnea. Also, nurses should advise patients on relaxation strategies that would promote healthy air flow in their systems.
An Essential Healthcare Discipline in Facilitating the Healthy Physical Activities
Physical therapists would be relevant professionals in enhancing the effectiveness of physical activity in the management of COPD patients. The specialists should collaborate with nurses in ensuring that COPD patients are at their optimum physical health. Physical therapists should teach patients on how to perform various exercises in a safe manner. COPD patients often have a delicate physical health, and the specialists should purpose to promote their (patients’) stability. Also, it is important for physical therapists and nurses to engage patients’ family members in strategizing physical activities for their patients. They should encourage patients’ family members to support their loved ones in exercising. Families would do so by monitoring their patients as they engage in various activities. They could also contribute by helping patients to undertake manual activities that could otherwise trigger hypoventilation and dyspnea in the high-risk group.
Part 4: Conclusion
The Effectiveness of an Interdisciplinary Team in Managing COPD
It is important to maintain the quality of care for COPD patients at a high level, especially during transitions from hospital care to home-based attendance. The process involves various considerations ranging from medication adherence, dietary practices, and the performance of physical activities. As such, the process would require various clinical professionals to cooperate for high-quality outcomes. Engaging nursing care and other relevant specialties in the transition would be a promising move. The team should work jointly with the common goal of bettering patient outcomes. A team involving specialties from the most relevant departments and professions would be effective in achieving utmost patient satisfaction and fetching desirable outcomes. It is also vital that such a team involve the families of patients. The extent of patient satisfaction would be a reflection of the ultimate achievements of the interdisciplinary team involved in the entire process.
Gaude, G. S., & Nadagouda, S. (2010). Nebulized corticosteroids in the management of acute exacerbation of COPD. Lung India : Official Organ of Indian Chest Society, 27(4), 230–235. http://doi.org/10.4103/0970-2113.71957
Hanson, C., Rutten, E. P., Wouters, E. F., & Rennard, S. (2014). Influence of diet and obesity on COPD development and outcomes. International Journal of Chronic Obstructive Pulmonary Disease, 9, 723–733. http://doi.org/10.2147/COPD.S50111
Itoh, M., Tsuji, T., Nemoto, K., Nakamura, H., & Aoshiba, K. (2013). Undernutrition in Patients with COPD and Its Treatment . Nutrients, 5(4), 1316–1335. http://doi.org/10.3390/nu5041316
Jimmy, B., & Jose, J. (2011). Patient Medication Adherence: Measures in Daily Practice. Oman Medical Journal, 26(3), 155–159. http://doi.org/10.5001/omj.2011.38
Seo, S. H. (2014). Medical Nutrition Therapy based on Nutrition Intervention for a Patient with Chronic Obstructive Pulmonary Disease. Clinical Nutrition Research, 3(2), 150–156. http://doi.org/10.7762/cnr.2014.3.2.150
Tashkin, D. P., & Ferguson, G. T. (2013). Combination bronchodilator therapy in the management of chronic obstructive pulmonary disease. Respiratory Research, 14(1), 49. http://doi.org/10.1186/1465-9921-14-49
We can write this or a similar paper for you! Simply fill the order form!
Use a 12 font size, double space your work and use APA format for citations, references, and overall format. Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page. Assistance with APA format, grammar, and avoiding plagiarism is available for free through the Excelsior College Online Writing Lab (OWL). Be sure to check your work and correct any spelling or grammatical errors before you submit your assignment.
You are required to submit your paper to Turnitin (a plagiarism prevention service) prior to submitting the paper in the course submission area for grading. Access is provided by email to the email address on record in your MyExcelsior account during week 2 of the term. Once you submit your paper to Turnitin check your inbox in Turnitin for the results. After viewing your originality report correct the areas of your paper that warrant attention. You can re-submit your paper to Turnitin after 24-hours and continue to re-submit until the results are acceptable. Acceptable ranges include a cumulative total of less than 15% for your entire paper, and no particular area greater than 2% (excluding direct quotes and/or references).
See the videos below for instructions on how to submit your paper to Turnitin and view your Originality Report.
Video – Submitting a Paper
Video – Viewing Your Originality Report
When you’re ready to submit your work for grading, click Browse My Computer and find your file. Once you’ve located your file click Open and, if successful, the file name will appear under the Attached files heading. Scroll to the bottom of the page, click Submit and you’re done.
SAMPLE ANSWER
The Patient with Musculoskeletal Limitations Complicated by a Medical Illness
Question one
Surgical care improvement project (SCIP) is an initiative aimed at providing healthcare for patients who have just undergone surgical procedures. It is estimated that more than 40% of operative procedures normally end up in post-operative complications. However, the introduction of the improvement project serves to significantly reduce the resulting complications. The SCIP is based on several core measures to assist in the reduction of post-operative complications. The ten core measures are based on prophylactic antibiotic treatment in pre and post-operative procedures. Also, antibiotics are given to the patient during the treatment process(‘SCIP core measures’, 2011). Another measure is the use of urinary catheter and hair removal strategies for patients. Other measures involve temperature management and the elimination of blood clots that would cause thrombosis in the veins also referred to as venous thromboembolism. The major aspect that has assisted in the reduction of surgical site infection has been the use of antibiotics. It is widely known that knee procedures such as knee arthroscopy involve the exposure of the knee tissues to the environment(‘SCIP core measures’, 2011). The environment contains numerous microbes that are opportunistic and take advantage of any opening on the skin surface. However, the presence of antibiotics serves to eliminate the microbes that ultimately serve to be the major causes of disease infection after operation procedures. Certain precautions have to be taken before the administration of the antibiotics(Drake, 2011). The drugs used should not have side effect to the patients. Neither are the antibiotics supposed to evoke the immune responses.in the case of the 60 year old woman, she had associated allergies with penicillin. The woman had taken certain drugs associated with the treatment of osteoarthritis which was also being examined by the medical procedure. Lisiprinol, lebrax and Celebrex were the drugs used by the old lady in the treatment of her conditions. Lisiprinol lowers blood pressure since the patient has hypertension. The drugs are administered after six hours when their effect is non-interfered by the other drugs. Additionally, the drug used is a cephalosporin and has no effect or similar effect as penicillin since it would not evoke an allergic reaction. The use of antibiotics in the surgical care processes has significantly reduced surgical site infections(‘SCIP core measures’, 2011). Ancef is an antibiotic of cephalosporin activity. Similarly other drugs have been used to reduce chances of infection after the surgical procedures(Drake, 2011). Nurses have to administer the drugs at specific times for the drugs to be able to function effectively.
Question two
The surgical care improvement method outlines measures involved in the removal of hair. Use of shaving or clippers to remove hairs would result in skin abrasions which would ultimately result in infections of the skin. Such infections would result in complications after surgical procedures. In the case of the sixty old woman, less hair is found around the knee region and since the knee is one of the common areas where skin abrasions can result in infection sites for microbes (Anderson, 2010).
In case there was excessive hair in the knee region it would be clipped off. However, the removal of the hair in this case shall not be by the use of a razor blade or other abrasive methods to the skin which end up affecting the skin by leaving infection sites that can easily be accessible to microbes. However electric clippers can be used in the removal of hair around the knee region since they are non-abrasive(Drake, 2011). If there were previous hair removal, the data abstractors supposed to look at the alternative methods. Also if the patient had in any way clipped hair from their skin, the data abstractor should seek methods that would not complicate the current status. The data abstractor can obtain the information about the patient from previous records especially the nurse’s report and mark at the appropriate hair removal method that had been initially used. This would assist the surgeons in knowing the appropriate method of hair removal that they can rely on the removal of hair especially at the knee(Anderson, 2010).
Question three
Venous thromboembolism is one of the common surgical complications after operative surgeries. Exposure of the skin directly activates clotting factors forming clots .This mechanism is used by the body to prevent entry of foreign microbes and over bleeding that would result in high pressure and loose of oxygen in the body. However, after forming clots, it is necessary that the initial clots formed in the blood would be dissolved by plasmin via plasminogen activating factors. However, sometimes the rate of clot formation during certain surgical procedures becomes greater compared to the rate of clot dissolution. The end result in this case would be blocking of the veins by clot or thrombus. The ultimate result of this is blockage of the blood supply by the thrombus ultimately resulting in what is commonly referred to venous thromboembolism commonly abbreviated as VTE. A major common form of VTE is DVT which in full means deep venous thromboembolism( Mont et al., 2014).
Surgical care improvement project involves the use of lovenox an anticoagulant. The anticoagulant has the ability to break down all the clots that have been formed in the body making blood to flow properly through the body. As a result, major complication issues such as venous thromboembolism are all avoided. However, in the administration of lovenox timing of the drug plays a very important role. Very late delay in the administration of the drug after surgical processes would directly be of no use since the process of clot formation would have already taken place and the administration of the drug would not be effective as anticipated before. Therefore it is necessary that the nurse ensures that the patient in this case the sixty old woman takes the drug at the required time to avoid formation of clots. In this case the drug was administered earlier the day after the surgical operation. The use of the leg attached to the hose pipe in the upright direction also assist the floor of blood from the surgical site and therefore the drug would efficiently remove the clots (Drake, 2011).
In conclusion the use of surgical care improvement projects has over the years reduced the associated surgical difficulties and complications that are normally as a result of surgical processes. The use of antibiotics has significantly reduced infection via sites while the application of certain drugs which are anticoagulants have effectively removed the thrombus that are as a result of clots formed during the surgical processes. Generally use of the SCIP has reduced the number of post complications and deaths that would be as a result of procedures. Although the process is being implemented, proper care and timing is important in meeting the set objectives relating to better health for patients (Kinnier, Barnard & Bilimoria, 2014).
Physical Health Considerations Prior to Further Assessments
Physical Health Considerations Prior to Further Assessments
Order Instructions:
You need to respond to following case study and provide a 1000 word medication management plan for the individual.
CASE STUDY 2: Rebecca
Rebecca is a 30 year old woman who is married with twelve month old daughter. Rebecca has had two (2) previous admissions to the mental health unit after attempting suicide, this is her third admission. Her husband Paul rang the triage team expressing concern that Rebecca was relapsing, he reported that she had been staying in bed saying she was tired all the time, crying and unable to care for their daughter. Rebecca’s husband reports their relationship is under strain. Both sets of parents are helping with the care of their child.
Family History
Rebecca is the youngest child of three siblings with two older brothers aged 39 and 36 years; her parents are very supportive and have a good relationship with Rebecca and her husband. Rebecca’s maternal grandmother and her aunt have a diagnosis of major depression. Rebecca and Paul live in the same suburb as her parents. Rebecca’s parents are active members of the carer’s group run by the local Mental Health service. Rebecca is to be discharged next week.
Medical History
– Nil physical problems
Psychiatric History
Rebecca was first diagnosed with Major Depressive Disorder at the age of 25 and has had three admissions to inpatient care in the past 5 years. Rebecca is currently being managed on mianserin hydrochloride – 120mg PO daily.
Current Mental State Examination Appearance & Behaviour:
– Looks stated age of 30
– Average height and weight
– Black hair, unkempt
– Dressed appropriate to weather, slightly dishevelled
– Has scars on both wrists
– Reluctant to be involved in conversation with intermittent eye contact
Cognition:
-Orientated to time, place and person. Not able to maintain concentration throughout interview.
Mood:
– Rebecca says she is very sad and tired
Affect:
– Congruent when discussing events leading to admission
Speech:
– Slow with monosyllabic responses
Form of thought:
– Logical and sequential
Content of thought:
– Believes that her husband and daughter would have a better life if she wasn’t
around. She states that she is not a good mother.
Perception:
– No perceptual disturbances elicited
Insight:
– Moderate insight into illness, states she knows she has depression and will take medication but doesn’t believe that it will do any good.
Judgement:
– Judgement is poor, however, she is willing to take medication, and try to stay well. – Is accepting of the need for case-management, has agreed to attend counselling
with her husband.
Please do NOT seek out medication management plan templates from the web. The assignment is to be presented in a question/answer format, No dot points and not as and essay (i.e. no introduction or conclusion). Each answer must be supported with citations.
You will need to reference according to APA referencing.(valid in Australia only articles and journals minimum 10. )
These are the question
Q1. What physical health considerations should be undertaken prior to giving this medication to the consumer?
Q2. Provide rationales for the use of this medication in this consumer.
Q3. What are the side effects / adverse effects of this medication? Indicate the management strategies that would be used to deal with these effects?
Q4. Discuss the relationship between medication management and recovery principles in mental health.
I AM ATTACHING THE MARKING GUIDE PLEASE FOLLOW THAT OR ESSAY WILL BE RETURNED TO FIX.
SAMPLE ANSWER
Physical Health Considerations Prior to Further Assessments
Despite the fact that physical and mental health conditions may be deemed as separate, research has proved that they are indeed interrelated and that the treatment of one may exacerbate the extent of severity in the other. The reverse is also true (NICE, 2009). The statement, therefore, explicitly suggests that in patients that have been diagnosed with both physical and mental problems, a great risk emanating from assessment and treatment of depression exists (Collinwood, 2013).
Therefore, treatment of depression disorders cannot be done in absentia. For instance, a study carried out by Moy et al., (2009) found that about 22% of patients diagnosed with Severe Chronic Pulmonary Disease had some form of mild depression. The treatment for depression may come under strain considering that some forms of antidepressant medications may or may not be effective depending on the type of physical complications present or the extent of it (Goldberg, 2010). Therefore, it may be impossible to rank the effectiveness of one antidepressant drug over another.
Rebecca’s case is one that meets the current diagnosis for depression threshold by satisfying both ICD-10 and DSM-IV systems. These symptoms include her constant complaints of lack of energy, loss of interest, low moods, poor judgment, being disheveled, and loss of self-worth—to the extent of making a third attempt at suicide. The fact that her condition is not linked to any physical problems makes it far easier to diagnose. However, her treatment alternatives implore the consideration of her past family history of depression as both her maternal grandmother and Aunt were previously diagnosed with depression at some point in their lives.
Rationale for Antidepressant Use on Rebecca
As is standard, medical guidelines implore for a thorough and comprehensive background assessment on patients to be performed so as to arrive at the best alternative for depression management. According to the National Institute for Health and Care Excellence (2009), a general practitioner must carry out case identification and recognition to ascertain the current state of the patient. The specificities that entail of this stage includes the identification of possible comorbid diseases that may act as risk factors preceding the occurrence of depression. However, because Rebecca had no prior physical ailments, it was imperative to go-on to the next stage.
The next stage of diagnosis as is, is to assess the risk factors such as ascertaining past first-degree relatives histories of previous cases of depression diagnosis. As was the finding, Rebecca’s relatives—her maternal grandmother and Aunt—had previous histories of psychotic disorders. Lastly, the assessment must factor in the extent to which this psychotic disorder was recurrent. In Rebecca, the rate of recurrence of depression is quite evident. She had had two previous admissions to the mental health unit following failed suicide attempts.
According to Gelenberg et al., (2010), the prescription of antidepressants must be within the confines of the patient’s profile as well a complete analysis of therapeutic response from prescription. Also, the prescription must not be in conflict with other prescription drugs; Selective Serotonin Reuptake Inhibitors (SSRIs) have been proven to raise the risks involved when administered in the presence of other drugs (Fournier et al., 2010). It has been shown that this puts patients at greater risks of complications such as gastrointestinal bleeding in analgesics and increase in plasma concentration of procyclidine in antimuscarinics among others (USPSTF, 2010).
The Side Effects of Prescription Drug and Management Strategies
Currently, Rebecca is being managed on Mianserin Hydrochloride and is on a dosage of 120mg PO daily. While these medications may offer therapeutic aid to the patient with regards to depression management, these prescriptions may breed other side effects. The extent of effects may depend on the actual prescription administered i.e. Tricyclic, Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin and Noradrenaline Reuptake Inhibitors (SNRIs), Reversible Inhibitors of Monoamine Oxidase A (RIMA’s), and Monoamine Oxidase Inhibitors (MAOIs) (ASHSP, 2009).
These side effects may range from: nausea, diarrhea, headaches, insomnia, weight gain, withdrawal symptoms, sexual dysfunctions, tremors, diabetes, and serotonin syndrome (Anderson, 2009; Sweitzer and Maguire, 2009). The continued use of SSRIs such as Mianserin Hydrochloride may lead to the occurrence of heightened suicidal tendencies amongst drug users. The most common methods that can be employed to manage these symptoms include for cases such as insomnia, adding small doses of trazodone may ease the side effects; for Akathesia inclusion of clonazepam; for sexual dysfunction considering the use of Bupropion. All these are included to act as panaceas for these side effects. However, this must be done considerately of the fact that certain drugs may conflict with the antidepressant prescribed.
Relationship between Medication Management and Recovery Principles in Mental Health
It has been shown that recovery from mental illnesses varies from different unique experiences of each individual (Richard, 2011). Therefore, there have to be different recovery management plans to satisfy unique individualistic needs. And with such, cases such as relapsing are avoided. Adherence to the principles of mental health management ensures efforts channeled to treatment, with regards to medication administration, complement each other. These principles extend to changing attitudes in mental patients, evaluating other forms of medication through constant reviewing of current medication plans and ensuring social interaction by building support systems around these patients (Anthony and Farkas, 2011)). In Rebecca’s case; therefore, a constant review of her medical progress ought to be reviewed periodically as well as encouraging her and her family to build stronger support systems to aid in her recovery.
Andersohn, F., Schade, R., Suissa, S. & Garbe, E. (2009). Long-term use of antidepressants for depressive disorders and the risk of diabetes mellitus. The American Journal of Psychiatry, 155 (5), 591-598
Anthony, W. & Farkas, M. (2011). The Essential Guide to Psychiatric Rehabilitation Practice. Boston: Boston University Center for Psychiatric Rehabilitation.
Fournier JC, DeRubeis RJ, Hollon SD, Dimidjian S, Amsterdam J.D., Shelton, R.C., Fawcett, J. (2010) Antidepressant drug effects and depression severity: a patient-level meta-analysis. JAMA, 303:47–53 [E]
Gelenberg AJ, Freeman MP, Markowitz JC, et al. (2010). Practice guideline for the treatment of patients with major depressive disorder. American Journal of Psychiatry, 167.
Goldberg D. (2010). The Detection and Treatment of Depression in the Physically Ill. World Psychiatry, Vol. 9, February 2010, pp. 16-20.
National Institute for Health and Care Excellence. (2009). Depression in Adults with A Chronic Physical Health Problem Treatment and Management. Retrieved from: https://guidance.nice.org.uk/cg91
Schweitzer, I., Maguire, K. & Ng, C. (2009). Sexual side effects of contemporary antidepressants: review. Australian and New Zealand Journal of Psychiatry, 43, 795-808.
United States Preventive Services Task Force. (2009). Screening For Depression in Adults. Annals of Internal Medicine, 2009; 151:784-792.
Richard, D. (2011). Prevalence and Clinical Course of Depression: A Review. Clinical Psychology Review, Vol. 31 (7) 1117.
Moy, M. L. et al. (2009). Multivariate Models of Determinants of Health-Related Quality Of Life in Severe Chronic Obstructive Pulmonary Disease. The Journal of Rehabilitation Research and Development, Vol. 46, 2009, pp. 643-54.
We can write this or a similar paper for you! Simply fill the order form!
Take the role of a clinician who is building a health history for one of the following new patients.
pre-school aged white female living in a rural community
With the information presented in chapter 1 of Ball et al. 2015) do the following:
1) How would your communication and interview techniques for building a health history differ with each patient?
2) How might you target your questions for building a health history based on the patient’s age, gender, ethnicity, or environment?
3) What risk assessment instruments would be appropriate to use with each patient?
4) What questions would you ask each patient to assess his or her health risks?
5) focus your discussion on patient above (pre-school aged white female in rural community)
6) Identify any potential health-related risks based upon the patient’s age, gender, ethnicity, or environmental setting that should be taken into consideration.
7) Select one to the risk assessment instruments presented in chapter one or 26 of the course text, or another tool with which you are familiar, related to selected patient.
8) Develop at least 5 targeted questions you would ask your selected patient to assess his or her health risks and begin building a health history.
***ONE REFERENCE HAS TO BE THIS ONE AND YOU MAY SELECT 2 MORE*********
The interview technique and communication will be selected cautiously because the patient is a child and from rural community. The interview technique applied is oral interview skills using open-ended communication. Additionally, purposeful silence, and active listening will be applied. This will help building a trustful patient-physician relation, thereby improving communication. The target questions will be assessed to avoid misinterpretation and miscommunication especially when dealing with concepts such as the patient age, gender, ethnic background and the environment. These include patient’s age, gender, medical history and their environment (Ball et al., 2015).
The risk assessment instruments that is appropriate for this patient is the AHRQ clinical care tools, particularly the Put Prevention into Practice (PPIP). This tool is chosen because it captures patient’s experiences as well as their lifestyles. This facilitates the assessment of the patient’s health condition. The five-targeted questions for this patient (pre-school aged white woman from a rural community) will mainly be addressed to the parent, as the child cannot express herself appropriately (Keeton, Soleimanpour, & Brindis, 2012). These include;
What are the child’s name, age, and ethnic background?
What are your child’s basic meals?
Is the child exposed to smoking?
Has the parent noticed any lost of interest to things that the child enjoyed in the recent past?
Has the child been hospitalized for any health reasons in the last three months? Explain the reason.
From the analysis, the following potential health related risk factors are identified; the first risk factor is obesity. The child is lives a sedentary life, and her diet is mainly fast food with high fat content. The child is also likely to suffer from respiratory disorders and cardiovascular disorders such as asthma and hypertension respectively.
Keeton, V., Soleimanpour, S., & Brindis, C. (2012). School-Based Health Centers in an Era of Health Care Reform: Building on History. Current Problems In Pediatric And Adolescent Health Care, 42(6), 132-156. https://www.doi:10.1016/j.cppeds.2012.03.002
We can write this or a similar paper for you! Simply fill the order form!