Discussion on Response to Posts in Medicine Order Instructions: The writer will have to read each of these articles and react to them by commenting, analyzing and supporting with relevant articles.
Discussion on Response to Posts in Medicine
The writer will have to read carefully before giving constructive comments on the article. The writer should write one paragraph of at least 150 words. APA and in-text citation must be used as each respond to the two articles must have in-text citations. The writer will have to use an article to supports his comments in each of the articles. Address the content of each article below in one paragraph each, analysis and evaluation of the topic, as well as the integration of relevant resources.
the details will be sent via email
Discussion on Response to Posts in Medicine Sample Answer
Discussion: Response to Posts
Response to Article 1
Fantastic post! Hyperlipidemia is among the common abnormalities placing a significant portion of the American population at the risk of severe diseases, and an approach to research on it is commendable (Centers for Disease Control and Prevention [CDC], 2015). There have been various agencies that have worked jointly in addressing hyperlipidemia, and the results of their partnership are standardized guidelines for the management and prevention of the condition (Stone, Robinson, Lichtenstein, Merz, Blum, Eckel, & Wilson, 2014). These guidelines are usually evidence-guided and they suggest multidisciplinary approaches to various aspects of hyperlipidemia management. However, it is always important that one refers to the most recent guidelines when undertaking research on a particular disease given that as time goes by, some of the previously embraced techniques become irrelevant or are proved wrong. These include treatment therapies applied as well as tools used for the disease.
Response to Article 2
Wonderful post! Health literacy is not only a right for patients, but it is also an effective means of facilitating care delivery, enhancing the effectiveness of treatment, and optimizing chances for desirable clinical outcomes (The Joint Commission, 2015). Various practices in disease management require a certain level of education including the ability to read and understand directions. When patients are educated, they would also have access to services such as health information and stand ineffective positions in safeguarding their health and get themselves involved effectively in health management. For instance, health literacy would be indispensable for patients with chronic ailments that would require self-care strategies. The approach to research on health literacy as it pertains to medication adherence and treatment compliance is encouraging. There is sufficient evidence linking health literacy, medication adherence, and treatment outcomes to each other (Adams, 2010, p. 65).
Discussion on Response to Posts in Medicine References
Adams, R. J. (2010). Improving health outcomes with better patient understanding and education. Risk Management Health Policy, 2010(3), 61-72.
Centers for Disease Control and Prevention (CDC). (2015). High cholesterol facts. Retrieved from http://www.cdc.gov/cholesterol/facts.htm
Stone, N. J., Robinson, N. G., Lichtenstein, A. H., Merz, N. B, Blum, C. B., Eckel, R. H., & Wilson, P. W. F. (2014). 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Retrieved from http://circ.ahajournals.org/content/129/25_suppl_2/S1.full.pdf
The Joint Commission. (2015). What did the doctor say? Improving health literacy to promote patient safety. Retrieved from http://www.jointcommission.org/assets/1/18/improving_health_literacy.pdf
Patient Medication Adherence Response to Articles Order Instructions: The writer will have to read each of these articles and react to them by commenting, analyzing and supporting with relevant articles.
Patient Medication Adherence Response to Articles
The writer will have to read carefully before giving constructive comments on the article. The writer should write one paragraph of at least 150 words. APA and in-text citation must be used as each respond to the two articles must have in-text citations. The writer will have to use an article to supports his comments in each of the articles. Address the content of each article below in one paragraph each, analysis and evaluation of the topic, as well as the integration of relevant resources.
Patient Medication Adherence Response to Articles Sample Answer
Response to Articles
Article 1
Great article! Compliance with treatment and adherence to medication affects the ultimate outcome of disease management. Usually, poor treatment outcomes do not only affect patients but also the health care system including nursing practice. In most cases, poor medicine use is associated with unnecessary expenditures hence raising the cost of disease management. as Jimmy and Jose wrote, there are various ways of improving patient adherence to medications, and nurses, pharmacists, physicians, as well as other clinicians play centrally in implementing them (2011, p. 155). Enhancing patient literacy is one of such approaches. As Brown and Bussell asserted, illiteracy is a crucial patient factor that results in poor medicine use and compliance with treatment (2011, p. 304). It is also true that the proper use of medicines would rely on effective communication between health care providers and their clients. As such, nurses should ensure that their clients understand treatment instructions and directions.
Article 2
Fantastic! As an evidence-based practice nurse, one should prioritize on patient treatment and management approaches that yield the best results. One of the opportunities available in promoting desirable treatment outcomes includes facilitating the accessibility of health information to patients, enhancing the usability of such information, and prioritizing on the quality of education that patients get regarding their health (Schardt, 2011, p.1). Health literacy would be effective in helping patients to make appropriate clinical decisions. It should be noted that terminally ill patients such as those with diabetes would indispensably require information concerning their health for them to exploit measures that would promote the quality of the lives that they would lead. For this group, critical information includes that concerned with self-management, self-care, and self-efficacy (Cavanaugh, 2011, p. 191). Patient education should also include issues such as risk factors to diseases and ways of overcoming them.
Patient Medication Adherence Response to Articles References
Brown, M. T., & Bussell, J. K. (2011). Medication adherence: WHO cares? Mayo Clinic Proceedings, 86(4), 304–314.
Cavanaugh, K. L. (2011). Health literacy in diabetes care: explanation, evidence, and equipment. Diabetes Management (London, England), 1(2), 191–199.
Jimmy, B., & Jose, J. (2011). Patient medication adherence: Measures in daily practice. Oman Medical Journal, 26(3), 155–159.
Schardt, C. (2011). Health information literacy meets evidence-based practice. Journal of the Medical Library Association : JMLA, 99(1), 1–2.
Harwood Medical Instruments Case Study Analysis Order Instructions: This case asks you to evaluate an new bonus plan that was designed to specifically address the perceived shortcomings of a previous plan. In particular you should consider:
Harwood Medical Instruments Case Study Analysis
•The purpose of changing the system
•The calculated bonuses for the managers
•How well the new plan is working
Harwood Medical Instruments Case Study Analysis Sample Answer
Case Study Analysis Background
The case study of Harwood Medical Instruments provides a description of a company whose management has a serious concern on the inclusion of the operating profit measure in the bonus plan/system of the company as been too narrowly focused. This was subsequently followed by the implementation of a new bonus plan/system that led to a reduction of the weighting of significance given to the operating profit in addition to the inclusion of more measures, including sales returns, on-time deliveries, scrap and rework costs, patent applications as well as customer satisfaction. Presumably, there was a consideration of these factors as factors that critically influence success.
Question 1 Answer
The purpose of making the change mainly because there was believe among the managers that the operating income inclusion in the bonus calculation was not a good representative as a short-term measure of financial performance.
Question 2 Answers
The calculation of the bonuses that were awarded to the managers in each division including the base bonus, sales return bonus as well as scrap/rework bonus for each six-month period is shown in the tables presented below.
Question 3 Answers
Evidence exists to show that some of the desired effects have been produced by the new bonus plan/system. In both divisions i.e. surgical instruments division and ultrasound diagnostic equipment division, as the division managers have become accustomed to the new bonus system/plan, there is a decline in sales returns, increase in patent applications, a decline in the level of scrap and rework as well as an increase in customer satisfaction levels. Furthermore, there has also been an increase in on-time deliveries in the surgical instruments division; however, this increase in on-time deliveries was not present in the division of ultrasound diagnostic equipment. As a result, this evidence of desire effects led to a significant increase in the bonuses to be paid in the second half of that financial year.
In evaluating this new bonus system/plan, it is imperative to consider if the improvement that resulted from its implementation was really good. By doing so, it will be possible to evaluate the new bonus system/plan in order to determine if the improvement is good particularly if the added performance factors and/or measures to the plan can considered to be critical factors that truly determine success (Anthony & Govindarajan, 2007). However, the small incremental bonuses that the managers got paid would without any doubts seem to be money that was spent well for the overall benefit of the company. Thus, the money given to the managers in form of bonuses in this new system should be considered very essential to the division managers, hence, leading to improvement in motivation levels, yet not incurring significant expenses levels for the company. Moreover, since the outcomes of including these factors into the bonus plan or system seem quite different between the two divisions, it is then quite important to consider if the same factors need to be applied to the two divisions as well as in the same weightings of significance (Chenhall, 2003; Otley, 2004).
In order to determine whether there are any changes that would be suggested to the new bonus plan, each of the performance factors or measures ought to be subjected to a detailed and critical scrutiny to succinctly know its benefits and undoing for the new bonus plan. For example, patents are not actually important for the surgical instruments division that usually sells such mundane products as clamps, scissors, surgical blades and bowls, among other products. This is attributable to the fact that, the inclusion of patents applications in the surgical instrument division may just encourage patents applications that even if are approved do not result to any significant economic benefit both to the division as well as the company as a whole (Chenhall, 2003). However, in the ultrasound diagnostic equipment division which is high-technology dependent and has high potential for development of new diagnostic technologies, patents applications should be encouraged because approval of a single patent application may contribute to significant economic benefit both to the division as well as the company as a whole. This economic benefit may not only financial but also increased customer satisfaction as well as high quality products (Horngren, Sundem & Stratton, 2005). Furthermore, there should be a change on the specific performance constraints on customer satisfaction and on-time deliveries which for the bonus to be awarded are set at an average of 90% and 95% for customer satisfaction and on-time deliveries respectively. On the two performance factors or measures, the bonus plan or system should be changed from awarding bonuses on basis of arbitrary performance constraints functions into a linear bonus awarding function (Chenhall, 2003; Otley, 2004). This is attributed by the fact that, through adoption of a linear function in awarding bonuses there will no constraints or cutoff target meaning the divisions will strive to achieve the highest level they could since the bonuses payoff will be directly proportional to the levels achieved in these performance factors (Anthony & Young, 2009; Vera & Kuntz, 2014).
Harwood Medical Instruments Case Study Analysis References
Anthony, R. & Govindarajan, V. (2007). Management Control Systems. Boston, MA: McGraw-Hill.
Anthony, R. & Young, D. (2009). Management control in nonprofit organizations. Boston, MA: McGraw-Hill.
Chenhall, R. (2003). Management control system design within its organizational context: Findings from contingency-based research and directions for the future. Accounting, Organizations and Society, 28(2-3), 127-168.
Horngren, C., Sundem, G., & Stratton, W. (2005). Introduction to Management Accounting. Hoboken, NJ: Pearson.
Otley, D. (2004). Management control in contemporary organizations: towards a wider framework. Management Accounting Research, 5(2), 289-299.
Vera, A. & Kuntz, L. (2014). Finance-oriented vs. operations-oriented management control in public hospitals. Journal of Hospital Administration, 3(6), 190-204.
This assessment aims to apply the principles of effective leadership and change theory to a change or performance improvement strategy which is professionally relevant to the learner. The assessment needs to consider the implications for workforce development and the ways in which organizational culture may enhance or hinder the capacity to achieve sustainable change outcomes. It is asked to consider the role of the leader in developing workplaces which are able to meet the demands for change.
This is a formal academic essay where it is required to demonstrate a capacity to critically discuss either a change management process or performance improvement strategy. (**Remarks: use Hong Kong health care practice)
Essay topics:
Performance improvement
Choose one area that requires performance improvement within an area of health care practice (clinical- e.g. a skill or clinical process, managerial – e.g. leadership issue or team building, or education- e.g. related program to a particular performance/ activity you would like to see improved.)
Analyze & critically discuss the following key points:
The area of an organizational performance that is of concern and how it relates to the organization’s strategic goals and objectives.
The steps required to implement a process for improving this aspect of organizational performance
The approach best suited to improving performance in this instance.
The type of performance indicators or measures selected.
Strategies for motivating and engaging stakeholder in ongoing performance improvement.
Thanks!
SAMPLE ANSWER
Performance improvement plans or action plans help give struggling employees get the opportunity to succeed and at the same time make them accountable for their past performance. The poor performance of clinicians is not smooth on the presence of it. Various reasons can be brought forward on the reasons for poor performance. This can be whether the clinician received the appropriate training and their knowledge of the expectations of the job. Any unforeseen roadblocks for future achievements also facilitate performance improvement plans (Bonow, et al., 2012).
It is, therefore, critical for the departments of a healthcare practice to give room for an open dialog and feedback directly from employees. This helps in the determination of the extent to which employees are provided with the sufficient resources and tools necessary for their success. Performance improvement can be used to address the failures that are arising to issues related to performance and behavior. The outcome of the performance improvement plan can be improved the performance of the health workers in Hong Kong. Also, training gaps and recognition of skills of employees can be evaluated. Employment related issues that may result can lead to the demotion of individual employees, transfer of some and demotion of underperforming employees.
In Hong Kong health care practice, an employee who does not perform well to meet expectations can be corrected by their supervisors. The performance improvement plan can be used to replace the disciplinary processes. This helps correct workplace behaviors that affect productivity given that any action taken earlier is better compared to waiting for the result. The presence of employee relations staff help in consultation and providing any technical assistance to health supervisors and other clinical employees and services. Training can also be supplied in the course of the performance improvement plan (Ferrer, et al., 2014).
Area of organizational Improvement
People who practice medicine have a high potential in assisting patients to stop smoking. Deficits have been found concerning the amount and type of training these people receive when undertaking smoking cessation counseling whereby they little consider the training. This area ought to be improved in health care facilities so as to improve the levels of service delivery in health systems. Trials should be conducted to examine the relativity of effective Quality improvement. The difference in educational programs of Departments of health care of Hong Kong in teaching smoking cessation skills help in achieving this noble course of improving performance.
Quality improvement works as a systems and processes. To make improvements, the health care and clinical departments need to have a clear understanding of their systems and delivery of services. Quality improvement takes into account the relationship between the resources of the organization and the activities carried out will help achieve improved health care quality. The service delivery in health is typically straightforward, and an example in a dental clinic and on the other hand, a large managed care hospital requires complex systems (Eijkenaar, et al., 2013).
The senior trained medical students and practitioners should demonstrate their efforts in improving the performance through their intervention to reduce smoking. The educational purposes of medical students should expose them to smoking cessation and the efforts to help smoking patients. Specific training should be provided in order to increase the rate of success of the nursing students. Traditional methods will not be effective and embracing teachings of that are appropriate in nature in all levels of education will help the students achieve this noble course.
Focus on patients: This is another area of measuring quality improvement and the level to which smoking cessation is effectively done. Patient’s needs ought to be met in health care, and the society and beneficiaries of the clinical area can be that there should be systems that affect the level of access by patients. Patients do not expect to queue for long due to slow systems. Patients also expect to receive care from the clinics that are based on evidence. The health practitioners can be trained so that they are well conversant with the type of treatment that they provide as per the DOME clinical skills. Evidences on successful cessation can be used. (Hamric, et al., 2013).
Patients also should expect safety at the premises and, therefore, need to assure them of safety by ensuring that medical practitioners observe security in their areas of service. Safety can be both physical and provision of quality medicines. Support for the engagement of patients in the treatment process is critical because patients can be able to express their problems directly. Care is communicated and coordinated with other parts or departments of the health care system. Another measure could be to ensure cultural competence in the assessment of the literacy levels of patients and to ensure that care is linguistically appropriate to ensure client satisfaction.
Focus on being part of the team: Quality improvement is a team process, and thus, knowledge and skills are brought together. Differences in thoughts of individuals are combined to obtain lasting solutions, and this approach is most useful when the process of quality improvement is complicated, and not even one person has the clinical skills or issue at hand. Also, it is useful when the process involves more than one discipline or work area and thus leading to the creation of creativity so as to establish a lasting solution (Nicolay, et al., 2012).
Let us say an organization wishes to reduce smoking cessation by reducing the patient wait time in the health care, the efforts presented by a team will help the health care facility achieve a lasting solution to these problems. All individuals should contribute to the team to ensure proper analysis as per the DOME clinical skills. Members bring in different perspectives on an issue and on how to sustain the improvements. Quality improvement and the participation of the teams highly depend on the availability of infrastructure. These can be team leadership and procedures plus the policies of undertaking each activity (Hermann, et al., 2014).
Focus on use of data: The major activity in quality improvement of services in Healthcare is data because it mainly describes how well the existing systems to reduce smoking are working. It is also an indication of the outcomes of applying a new change and is useful when noting a success in performance. The use of data helps in separating what is happening actually from what people think. For example, the level of attendance of patients to the available number of clinical officers. Data is useful in setting up a baseline whereby performance at that baseline is acceptable and deemed fit. Scoring low at the first episode can be accepted with an anticipated improvement in subsequent results. It also helps in the reduction of solutions not useful from being placed be the supervisors.
Procedural changes can easily be monitored, and this helps make sure that the resulting improvements can be sustained. The clinicians and nurse should be able to cope with the improvements in helping smoking patients and give an indication if the changes affected have shown any improvement in their service delivery. Performance can easily be compared to all the departments, and, therefore, patients and staff satisfaction surveys can easily be conducted (Witter, et al., 2012). Quality improvement will help achieve improved health of patients and efficiency in managerial and clinical processes. It also helps avoid costs that are associated with failure of processes and errors thus leading to a balance of quality in Hong Kong health care services (Unützer, et al., 2012).
Steps to implement the process
The first step is to document the performance issues. The issue being a quality improvement in health care, it is good to develop a format or use existing ones to ensure that consistency of values is observed. This helps protect the clinical heads if any legal claims are made in expectations. The performance plan will include information about the staff. These are their skills and training received to handle patients. Also, the dates should be expected and any performance gap should be indicated. Expected performance is described and compared with the actual performance and the plan of action designed by the team stated clearly.
The second step is to develop an action plan in the process of quality improvement. The quality of service provision is desired to be improved to match the DOME clinical skills and thus need to create a plan that suits those standards. An action plan can be established by the supervisors and request an expression of interests from employees to ensure that everyone agrees to it. Collaborative engagement makes it easy to solve issues and thus, creating database requires employee participation (Murray, et al., 2013). Some of the nursing and clinical tools can be included while others can be excluded depending on the mutual decisions. The consequences of not meeting the objectives are also set.
The third step is reviewing the performance plan in the organization. Quality improvement in the clinical case engages the top management and the supervisors. The director of a department should seek guidance from the senior manager or directors of health on matters documentation of the performance plan. This will help ensure that all the parties to the quality improvement project adhere to the requirements of the program and hence instill disciplinary activities to lazy clinical workers. It should be specific, attainable and relevant (Jha, et al., 2012).
The fourth step is meeting with the employees and, if possible, the other stakeholders including patients. A program might be in the process of its quality improvement, but the patients feel that lack sufficient knowledge of how to use the service. Here, the action plan can be modified to include specifications and proposals from the stakeholders. The nurses and clinical officers can then sign the personal improvement plan forms.
The fifth stage involves making follow ups. Both the employees and the supervisors should be holding meetings on designed basis to evaluate the level of improvement of the quality of service. The meeting should include discussions concerning the objectives and any matters arising are documented. The employees are expected to ask questions and go further to seek guidance on a particular step, for example, the introduction of online medicine payment and the establishment of booking systems. The nurses and clinicians are motivated towards producing the best in quality improvement (Santiago, et al., 2014).
The last step is concluding the process whereby non-performing employees who do not follow the quality improvement plan will experience poor performance. This is because the new system is taking over slowly. This can be a high time for him or her to request for reassignment to other departments of the clinic such as social work or can choose to be transferred. When the goals have been reached, the quality improvement plan can be done periodic reviews to ensure its flexibility in service provision and health care practices.
Approaches to Performance Improvement
Not all quality improvement strategies are successful although health care facilities seek to improve performance. The first approach is through the system view. The best acceptable approach in quality improvement should be taken using Systems Thinking techniques that help in the identification of activities that are reducing the ability of the clinical skills from being achieved. Operations analysis can be used to ensure the maximum improvement of quality all through the performance improvement phases. This will enable focus on development that brings change to the health care departments (Toussaint, et al., 2013, January).
People involvement is an approach because any quality improvement’s success depends on the efforts of people at all the improvement levels. All the employees including the social workers and nurses plus clinical officers should be at the front line and involved in the decision-making process. Most of the failed quality improvements as per DOME clinical skills is as a result of ignorance. The lead supervisors should include other employees in the decisions to undertake quality improvement. This results in failed efforts of the management. Engaged workers will feel the ownership of the quality improvement process and thus enabling them to become owners of the project (Haas, et al., 2013).
Another approach to ensuring quality in health care is improved is to focus on the process involved. Focusing on the process is the best approach compared to building up blames due to lapses. Maybe some of the health workers and clinicians do not come to their jobs on a daily basis which is an indicator of failed implementations. The new process will help promote the operations and patient attendance and achieving the quality improvement goals. The improvements in quality require that people within the health care change their behavior and focus on the process to suit the new quality improvement plans for the clinics.
The purpose of the quality improvement should be evaluated and defined. Here, it is to improve service delivery to the patients while reducing the queuing of these patients. The process involves all the levels of management in Hong Kong health care, and thus, definition of the existing system and the available staff plus patients is important. The value of service offered by the clinic is critical and customer satisfaction should be measured. In a clinical case, the primary customers are patients and therefore there is a need to ensure that the level of services offered to them is satisfactory (DeRenzi, et al., 2012, March).
The value stream is important in the determination of the entity’s value creation to the patients through the existing Value Stream Analysis set aside by the quality improvement team. At a strategic level, the firm is analyzed and compared to the tactical level of individual departments in the clinical case. People performing value stream such as nurses should be included, and this carries a short period.
An improvement plan will be produced by the value stream whereby actions are categorized according to the ability of undertaking. Others can just be done while others will follow the rapid improvement events. The achievement of these goals should include involvement in the process of implementing the quality improvement to people. It values the current ways of job performance while reducing the discrepancies in the process of improving the quality of health care services. The last approach base is to sustain the improvements in the quality of services. Key metrics plus the loops for controlling quality improvement are planned with an aim of ensuring that health workers adapt to the new changes in the system (Källander, et al., 2013).
Performance Indicators
Monitoring the quality improvement is facilitated by the indicators, and they help to create the basis for improving the quality of health care practice and the modified system. The indicators need to be designed and defined so as to enable its implementation in agreement with medical practices. A rate based index will use the data concerning the events unfolding and their occurrence at the same frequency. These are the rates and proportions with which the quality improvement project has satisfied the patients in the hospital. The trends over the years will indicate the speed with which the performance improvement has been active (Kern, et al., 2014).
The sentinel indicators will help in identifying the individual events such as patient waiting time and its improvements. This helps in triggering further alterations to the performance improvement plan of quality. It will show the poor performance as a comparison to the past clinical skills performance. Process indicators will show the actual performances and what has been done while giving and receiving care by patients and clinicians. It helps indicate what the clinicians attended to the patients and the quality it was done. The care that health care provider’s accord to patients and the limits of the stipulated period all through the process according to dome clinical skills are included (Unützer, et al., 2014).
Structural indicators such as health system characteristics and quality improved will affect the quality of the improved system to meet the needs of healthcare of patients. It will help in describing the amount of resources used by the quality improvement system of the organization in delivering the services and programs. These systems are directly related to the health care performance improvement system and are affected by the number of the staff dispatched to the new system. Resources concerning money, the beds in the health care and the supplies plus the wards or buildings for in-patients are analyzed (Jha, et al., 2012). This will help in judging the quality of care provision under conducive to the quality of health provision in Hong Kong.
Outcome indicators assist in showing the health states and events that follow the quality improvement program in the health care system. This includes the possible effects of the new system on both patients and the health workers. It captures the potential impact of the policy on the health improvement and performance of patients. The worst outcome of the quality improvement is death. This results from untimely or naive implementation. Another outcome is the possibility of disease outbreak and its symptoms and abnormalities. Discomfort can result from the quality improvement process, and these may include nausea and dyspnea. Disability is another possible outcome, and it can present itself in the form of impaired recreation. The patients can also be dissatisfied with the quality of service and can lead to persistent complaints.
Adjusting to these indicators can involve the factors that are contributing to the survival of patients in the clinical process and the outcomes of the health quality improvement. The results of the quality improvement can be adjusted in comparison to other factors not within the health care system through quality assessment and other factors or components that are about quality health care. Demographic factors of the patients such as age and sex are considered. The lifestyle of the patients and psychosocial factors plus compliance to the prescribed medication can affect the quality of outcome. The severity of the illness and its comorbidity should be considered in the outcome evaluation (Groves, et al., 2013). The quality of treatment and the competence plus technical equipment available and the evidence-based treatment can affect quality. Adherence to using the clinical guidance available and cooperation from the top medical stakeholders is essential.
Strategies for Motivating and Engaging Stakeholders
Despite the advances in the quality improvement through healthcare in performance improvement, there is a failure in reliability from the customers as a result of health care. The systematic increase in health workers’ complexity and hard work does not guarantee efficiency in health care provision. Fixing these problems require transformations in systems to a team-based services aimed at satisfying the customers.
Engagement in the shared purpose of the quality improvement in clinical skills involves leaders’ shift of conversation to achieving the articulated visions and improved patient care. The need for sacrifice should be embraced because the performance improvement process can reduce autonomy and income levels of physicians. Leaders should encourage health workers to change the mentality of maintaining the status quo to advanced medical services (Friedberg, et al.,2014). The needs of the patients need to be prioritized, and doctors cannot be shielded from this.
Consensus needs to be built to allow the views that are varied to be articulated. An appeal to self-interest is essential given that physicians need to be motivated through financial incentives. The measures of performance should be realistic and non-biased o reinforce engagement of the health workers. The compensation can be pledged depending on the quality of improvements per individual. The successful health workers can be communicated to through earning them respect from their duties. Role play is appreciated through the positive feedback from the top management as no employee yearns to lose respect from colleagues.
The tradition of the health care and clinical practice of the physicians should be valued as a member of the health care system. They are given motivation so that they can adhere to the standards and traditions of the organization. Dome clinical skills tradition has been followed by doctors, and they are required to wear hosiery for female physicians and neckties for male medical practitioners (Reeves, et al., 2013). The patients can be engaged by the provision of training on the ease of access to certain technological improvements. Mass education can be carried out and the patients given sessions to express their levels of satisfaction. With this, the entire process of quality improvement in performance improvement of health care can be achieved.
References
Bonow, R. O., Ganiats, T. G., Beam, C. T., Blake, K., Casey, D. E., Goodlin, S. J., … & Masoudi, F. A. (2012). ACCF/AHA/AMA-PCPI 2011 Performance Measures for Adults With Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures and the American Medical Association–Physician Consortium for Performance Improvement. Journal of the American College of Cardiology, 59(20), 1812-1832.
Ferrer, R., Martin-Loeches, I., Phillips, G., Osborn, T. M., Townsend, S., Dellinger, R. P., … & Levy, M. M. (2014). Empiric Antibiotic Treatment Reduces Mortality in Severe Sepsis and Septic Shock From the First Hour: Results From a Guideline-Based Performance Improvement Program*. Critical care medicine, 42(8), 1749-1755.
Eijkenaar, F., Emmert, M., Scheppach, M., & Schöffski, O. (2013). Effects of pay for performance in health care: a systematic review of systematic reviews. Health policy, 110(2), 115-130.
Hamric, A. B., Hanson, C. M., Tracy, M. F., & O’Grady, E. T. (2013).Advanced practice nursing: An integrative approach. Elsevier Health Sciences.
Nicolay, C. R., Purkayastha, S., Greenhalgh, A., Benn, J., Chaturvedi, S., Phillips, N., & Darzi, A. (2012). Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. British Journal of Surgery, 99(3), 324-335.
Hermann, R. C., & Palmer, R. H. (2014). Common ground: a framework for selecting core quality measures for mental health and substance abuse care.Psychiatric Services.
Witter, S., Fretheim, A., Kessy, F. L., & Lindahl, A. K. (2012). Paying for performance to improve the delivery of health interventions in low-and middle-income countries. Cochrane Database Syst Rev, 2(2), CD007899.
Unützer, J., Chan, Y. F., Hafer, E., Knaster, J., Shields, A., Powers, D., & Veith, R. C. (2012). Quality improvement with pay-for-performance incentives in integrated behavioral health care. American Journal of Public Health,102(6), e41-e45.
Murray, C. J., Richards, M. A., Newton, J. N., Fenton, K. A., Anderson, H. R., Atkinson, C., … & Braithwaite, T. (2013). UK health performance: findings of the Global Burden of Disease Study 2010. The lancet, 381(9871), 997-1020.
Jha, A. K., Joynt, K. E., Orav, E. J., & Epstein, A. M. (2012). The long-term effect of premier pay for performance on patient outcomes. New England Journal of Medicine, 366(17), 1606-1615.
Santiago, J. M. (2014). Use of the balanced scorecard to improve the quality of behavioral health care. Psychiatric Services.
Toussaint, J. S., & Berry, L. L. (2013, January). The promise of Lean in health care. In Mayo Clinic Proceedings (Vol. 88, No. 1, pp. 74-82). Elsevier.
Haas, L., Maryniuk, M., Beck, J., Cox, C. E., Duker, P., Edwards, L., … & McLaughlin, S. (2013). National standards for diabetes self-management education and support. Diabetes care, 36(Supplement 1), S100-S108.
DeRenzi, B., Findlater, L., Payne, J., Birnbaum, B., Mangilima, J., Parikh, T., … & Lesh, N. (2012, March). Improving community health worker performance through automated SMS. In Proceedings of the Fifth International Conference on Information and Communication Technologies and Development (pp. 25-34). ACM.
Källander, K., Tibenderana, J. K., Akpogheneta, O. J., Strachan, D. L., Hill, Z., ten Asbroek, A. H., … & Meek, S. R. (2013). Mobile health (mHealth) approaches and lessons for increased performance and retention of community health workers in low-and middle-income countries: a review.Journal of medical Internet research, 15(1).
Kern, R. S., Liberman, R. P., Kopelowicz, A., Mintz, J., & Green, M. F. (2014). Applications of errorless learning for improving work performance in persons with schizophrenia. American Journal of Psychiatry.
Unützer, J., Schoenbaum, M., Druss, B. G., & Katon, W. J. (2014). Transforming mental health care at the interface with general medicine: report for the presidents commission. Psychiatric Services.
Groves, P., Kayyali, B., Knott, D., & Van Kuiken, S. (2013). The ‘big data’revolution in healthcare. McKinsey Quarterly.
Reeves, S., Perrier, L., Goldman, J., Freeth, D., & Zwarenstein, M. (2013). Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev, 3.
We can write this or a similar paper for you! Simply fill the order form!
A patient has been admitted to the mental health unit with a diagnosis of bi-polar disorder. During a meeting the family inquires about the use of alternative therapies. Based on your readings and knowledge discuss what the RN would teach the patient and family and incorporate modalities, usefulness, effectiveness and how to increase compliance with therapeutic modalities
Alzheimer’s is a condition that is increasing in incidence in our population. There is no differential diagnosis so the start of the disease may go unnoticed. Once the manifestations become more apparent it often places a tremendous strain on the caregiver. Caregiver role strain is a nursing diagnosis that is frequently applied in the situation. Since patient wandering and confusion are common for the patient with Alzheimer’s disease what would the RN teach the family about maintaining a safe environment? Discuss the support systems that are available to families
SAMPLE ANSWER
Mental Health: Alzheimer’s Disease
Memory loss is a critical manifestation of Alzheimer’s syndrome. The condition places patient at the risk of harm from the environment. For instance, impaired memory would predispose people to practices such as leaving their electrical appliances running and unattended. Teaching care givers on approaches of protecting their patients would be a necessary health management plan.
Registered nurses should teach families of Alzheimer’s patients to keep abreast with their loved ones. Families should know their role on monitoring their patients so that they do not hurt themselves when performing basic duties such as cooking and driving. Also, families would be advised to promote the safety of their patients’ environment by installing appliances that can shut automatically when left unattended (US National Institute of Health, 2010, Pg. 14). The nurses would also advise patient families to limit the exposure of their loved ones to wandering as the practice would place them at the dangers of getting lost or encountering accidents. Families would do so by providing the needs that would motivate patients to wander.
Caring for Alzheimer’s disease patients is often challenging for families. It is therefore necessary for them to seek support systems for the activity. Available support systems include voluntary groups and friends who would offer to help for services such as cleaning and shopping for the patients (Robinson, Wayne, & Segal, 2015). Healthcare professionals would also be of substantial support as they would help families to monitor the progress of their patients. In addition, families could exploit support systems such as workshops that train people on care giving skills (Robinson, Wayne, & Segal, 2015). Other approaches include exploring online materials and books that address the management of Alzheimer’s disease.
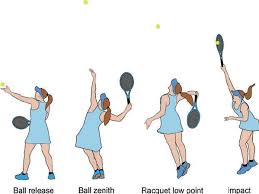
Paper instruction : Tennis serve
Descrition of the Motor skill : Beginning Phase, Middle Phase, Final Phase( Anatomical analysis:Muscle participation and form of contractions. )
*NO Websites and online database (wikipedia) are accepted; Google scholar web search preferred.
*No Instruction No conclusion needed. Just directly talk about the subject in detail.
SAMPLE ANSWER
Anatomical Analysis of Tennis Serve
The Beginning Phase
The stage involves player’s preparation for the serve. Different muscle activities take place in four phases. At the initial phase, there is minimal involvement of the shoulder and scapular muscles (Kovacs & Ellenbecker, 2011, Pg. 506). The player proceeds to the release phase where there is little activation of the left erector spinae but increasing participation of the right erector spinae muscles. Trunk stabilization is crucial at the stage and lower trunk muscles are activated to stabilize the lumbar spine. Muscles activated include rectus abdominis and internal and external oblique muscles. In the third phase, the player generates potential energy by properly positioning the feet. The foot-up and foot-back techniques are the commonest techniques, and they involve knee joint extensor muscles to a significant extent. In the foot-up technique, the posterior compartment of lower limb muscles offers upward and forward drive for the player. On the other hand, the anterior compartment offers stability for rotational momentum (Kovacs & Ellenbecker, 2011, Pg. 506). The same events occur in the foot-back technique, but there is more contraction of the knee joint extensors than in the foot-up technique. The third phase also involves a lateral rear tilt of the pelvis and the shoulder. The activity generates angular momentum for lateral flexion of the trunk. For right-handed servers, the ipsilateral erector spinae muscle activation is higher than that of contralateral erector spinae (Kovacs & Ellenbecker, 2011, Pg. 506). The left lateral erector spinae plays significantly in lateral flexion of the trunk during the third phase. Iliocostalis and longisimus dorsi are also active during the phase. They contract unilaterally to flex the lumbar vertebral laterally. The fourth phase begins with the activation of serratus anterior (Kibler, Chandler, Shapilo, & Conuel, 2010, Pg. 747). The upper trapezius muscle is then activated resulting in acromion elevation and stabilization of the scapular. The activation of the lower trapezius later enhances scapular stabilization and elevation of the acromion (Kibler et al., 2010, Pg. 747). The deltoid and supraspinatus are also activated to depress the head of the humerus and control external rotation.
The Middle Phase
The phase involves acceleration, and muscle activity exceeds the one in the beginning phase (Kibler et al., 2010, Pg. 747). For the internal humeral rotation, activated muscles include the serratus anterior, latissimus dorsi, subscapularis, and pectoralis major (Kovacs & Ellenbecker, 2011, Pg. 507). The first phase of the middle phase ends with the activation of the gastrocnemius, vastus medialis, and vastus lateralis. Both the trunk and legs coordinate to generate the greatest kinetic energy for the middle phase. The last stage of the middle phase involves minimal extension of the knee, wrist, and elbow joints. Rectus abdominis participates actively during this phase (Chow, Park, & Tillman, 2009). The phase also involves increased activation of rectus abdominis and external oblique muscles that are mostly involved in trunk flexion. Internal oblique is mostly activated during twisting of the trunk.
The Final Phase
The stage involves deceleration and follow-through. The infraspinatus is activated, and it contributes as an assistive muscle for humeral deceleration and distraction of the shoulder joint (Kibler et al., 2010, Pg. 747). The posterior rotator cuff is also activated together with biceps brachii, serratus anterior, latissimus dorsi and deltoid. The right erector spinae is also more active than the left erector spinae during deceleration. Deactivation of the anterior deltoid precedes that of other muscles. During the final phase, internal rotation and horizontal adduction are not needed. The serratus anterior and upper trapezius muscles are the next on the trend and their deactivation occurs as the acromial elevation decreases (Kibler et al., 2010, Pg. 747). The deactivation of infraspinatus occurs as humeral rotation decreases. Complete restoration of posture results following the activity of the lower trapezius for the scapular, supraspinatus and teres minor for the humeral head, and posterior deltoid for the upper arm (Kibler et al., 2010, Pg. 747).
References
Chow, J. W., Park, S.-A., & Tillman, M. D. (2009). Lower trunk kinematics and muscle activity during different types of tennis serves. Sports Medicine, Arthroscopy, Rehabilitation, Therapy, and Technology : SMARTT, 1, 24. http://doi.org/10.1186/1758-2555-1-24
Kibler, W. B., Chandler, T. J., Shapilo, R., & Conuel, M. (2010). Muscle activation in coupled scapulohumeral motions in the high performance tennis serve. British Journal of Sports Medicine, 41(7), 745-749.
Kovacs, M., & Ellenbecker, T. (2011). An 8-Stage Model for Evaluating the Tennis Serve: Implications for Performance Enhancement and Injury Prevention. Sports Health, 3(6), 504–513. http://doi.org/10.1177/1941738111414175
We can write this or a similar paper for you! Simply fill the order form!
Have to complete at lease 10 empirical articles in my educational field. I work with children Kinder – Fifth grade.
SAMPLE ANSWER
Diabetes mellitus Annotated Bibliography
Seino, Y., Nanjo, K., Tajima, N., Kadowaki, T., Kashiwagi, A., & Araki, E. et al. (2010). Report of the Committee on the Classification and Diagnostic Criteria of Diabetes Mellitus. Journal Of Diabetes Investigation, 1(5), 212-228.
The article classifies the two types of diabetes mellitus, type 1, and diabetes type. It also discusses the causes of the various types of diabetes mellitus and the factors that are likely to predispose one to diabetes mellitus. In making the distinction type, I am referred to as insulin dependent diabetes mellitus associated with the destruction of pancreatic beta cells while type 2 is associated with lifestyle changes especially obesity.
Reinehr, T. (2013). Type 2 diabetes mellitus in children and adolescents. World Journal Of Diabetes, 4(6), 270.
The article reviews the causes of type two diabetes mellitus in children. Specifically, it looks at the factors that predispose children to diabetes mellitus type 2 since it’s commonly associated with lifestyle changes. It also looks at the methods for treatment of type 2 diabetes as well as management of children suffering from type 2 diabetes.
Ewald, N. (2013). Diagnosis and treatment of diabetes mellitus in chronic pancreatitis. World Journal Of Gastroenterology, 19(42), 7276.
A review is given on chronic pancreatitis. It should be remembered that diabetes type 1 involves the destruction of the beta cells of the pancreas by autoantibodies.in this case methods for detection of type 1 diabetes mellitus are outlined as well as the treatment.
Buchanan, T., Xiang, A., & Page, K. (2012). Gestational diabetes mellitus: risks and management during and after pregnancy. Nat Rev Endocrinal, 8(11), 639-649.
The article review a different type of diabetes mellitus commonly observed in pregnant women. It is known as gestational diabetes mellitus. It plays an important role in making a woman susceptible to diabetes mellitus type 2. Nutritional effects as wells as the risks associated with gestational diabetes mellitus are reviewed in this article.
Sacks, D., Arnold, M., Bakris, G., Bruns, D., Horvath, A., & Kirkman, M. et al. (2011). Executive Summary: Guidelines and Recommendations for Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus. Lab Med Online, 1(4), 173. http://dx.doi.org/10.3343/lmo.2011.1.4.1
The article looks and compares the different methods that are used to diagnose the different types of diabetes mellitus. Laboratory guidelines and the permitted reference range values of the results are also provided.
Litmanovitch, E. (2015). Short and long-term neurobehavioral alterations in type 1 diabetes mellitus pediatric population. World Journal Of Diabetes, 6(2), 259.
The article reviews the neurological damage that is associated with diabetes mellitus type 1. It also discusses the emerging technology that will assist in reducing the glycemic glucose levels, therefore, reducing the effects of diabetes mellitus, especially to the neural system.
Antonelli, A. (2014). Hepatitis C virus infection and type 1 and type 2 diabetes mellitus. World Journal Of Diabetes, 5(5), 586.
The article identifies the relationship between diabetes mellitus and hepatitis C. the main relationship is associated with viral effects, pro-inflammatory cytokines and insulin resistance in the liver. It also shows how clinical trial conducted on hepatitis c patients has resulted in a decrease in the glucose metabolism providing an important mode of treatment for glycemic patients.
Nauck, M. (2014). Update on developments with SGLT2 inhibitors in the management of type 2 diabetes. DDDT, 1335.
The author discusses the important role that the kidney plays in the maintaining of glucose levels in the body via the sodium glucose transporters type 2. Use of sodium glucose transporters inhibitors reduces the renal reabsorption of glucose, in the long run, decreasing the amount of glucose in the body.
Igwe, M., Uwakwe, R., Ahanotu, C., Onyeama, G., Bakare, M., & Ndukuba, A. (2013). Factors associated with depression and suicide among patients with diabetes mellitus and essential hypertension in a Nigerian teaching hospital. Af Hlth Sci, 13(1). http://dx.doi.org/10.4314/ahs.v13i1.10
The study was conducted in Nigeria to highlight the effects of diabetes mellitus and hypertension to the normal lives of the people. Basically, two concepts were looked at. The role of diabetes mellitus in causing suicidal and depression in patients.
Eisenbarth, G. (2010). Banting Lecture 2009: An Unfinished Journey: Molecular Pathogenesis to Prevention of Type 1A Diabetes. Diabetes, 59(4), 759-774.
The article discusses the metabolic pathways that are involved in diabetes mellitus specifically carbohydrate, fat and protein metabolism. It also discusses how this pathway can be used to block the effects of hyperglycemia in type 1 diabetes mellitus patients.
We can write this or a similar paper for you! Simply fill the order form!
Hi pleaseclick on link above . And log in with my username and u r required to read each module and assessment task Given at the end and write on it in relation my specialty area which was preoperative. And u need to cite whatever u write with peer reviewed articles or references . Make sure u read all the modules before u start writing assignment .
It’s 1000 words altogether (3 modules )
SAMPLE ANSWER
Module 1: legal responsibility in preoperative care
Personnel in the preoperative settings have numerous responsibilities in relation to the legal and ethical responsibilities. This is because their duty of delivering care is deep seated core within the nursing principles and code of conduct. In this context, the documentation of nursing care is a legal responsibility during preoperative care. This is the only proof they can use in their defense that they are not negligent (Litwack, 2010). The documentation process must meet the established practice of documentation. The records must indicates patients preoperative assessment, care provided by the surgical team, the outcomes and evaluation plan conducted as they are used to indicate the procedures that should be used in primary care settings. One of the most important documentation processes in preoperative care is the informed consent (Lim et al., 2010).
The main element of quality care in preoperative department is the issue of informed consent. The general legal principle of preoperative care is that the healthcare provider must obtain a valid informed consent from their patient, before any treatment intervention is put in place. This principle is put in place to ensure that the patient enjoys the right to their health, and to decide what health care practice that takes place in their body. This right is entitled to every patient including the children, but the laws have specific rules that should be followed for these minors, or patient under critical care (Litwack, 2010).
Additionally, patient have right to confidentiality, unless they have allowed their health condition be shared in the consent form. This implies that the patient have a legal right that must be obeyed by the healthcare providers in the preoperative care, if the patient refuses presence of visitors during this phase. The healthcare providers have a legal responsibility of informing all the patient’s visitors and the contractors that the preoperative environment is a very confidential department, and that it is only chaperoned by the staff members assigned in these departments only. If the visitors are present for any reasons, it must be recorded in the theatre record for referencing purposes (Tilse and Wilson, 2013).
Module 2: Dilemma of providing patient information to carers
Patient privacy is important as it upholds patient’s dignity, which is a core nurse principle and fundamental aspect of care. The physicians are often face challenges as patients health deteriorates, especially when they have to deliver relevant information that can be used at home care. More often, doctors face criticism from family relatives and carers for not giving patients adequate information. This is because it is the physician legal obligation to respect and to protect patient information. Traditionally, patient privacy philosophy argues that patient identify the person who can be informed about their health condition, and including if the information can be shared with the friends or the family (Gold et al., 2009).
This theoretical model, which focuses on patient centered care, is not always the clinical reality. The legal obligations demands that such information should be provided is there is explicit permission. This can create huge debate if a relative who have been at the center of delivering care of patient is denied the patient information. On the contrary, if the patient condition does not permit them to make decisions for themselves due to severe illness or dementia, then the family or carer can be integrated in the decision making process. These two scenarios indicate divergent positions in the communication between the patient’s carers and the physicians. This indicates that the culture of patient centered care in some cases can create tensions in healthcare (Atkinson & Coia, 2012).
In reality, the family members and carers are always concerned about the patient health. This is especially important during transition of care from acute settings to homes. In this context, the patients discharged from the hospital are weak and will rely on caregiver for their daily activity. Research indicates that providing patient information to carer is beneficial because it reduces carer anxiety, improve competency, and improve the coping strategies that will facilitate the decision-making processes. These findings have been supported by one studies conducted in cancer patients. From this perspective, then it is true that the carers work is often unrecognized, and often overlooked due to the way the medical ethics and law protects the patient’s information. These individualistic ethics dominating the healthcare practice could be hindering quality care (Gold et al., 2009).
Therefore, it is important to empower the carer with clear and effective communication about the essentials as they undertake the quasi-nurse role. This is because the patient carer knows the patient best. The carer is the constant support in patient’s life, and over time, the patient builds trust. Research indicates that the carer are encouraged and feel appreciated when integrated in decision making processes, as they become aware of the patients physical and psychological demands than when denied access to patient information (Atkinson & Coia, 2012).
Module 3: Reflection
Patient perspective about illness, disease, dying and death is best explained by the Spoon theory developed by Christine Miserandino. According to her, illness especially those diagnosed with chronic illness such as systemic lupus makes the patient have limited expendable energy. This is because even a small activity makes a patient loose a spoon (energy), which is very difficult to retrieve back. Her perspective about systemic lupus and all chronic illnesses are that patients are weak to even to undertake simple daily activities such as taking birth, walking and feeding. This is similar to the daily incidences that we deal with at the perioperative care. Most of the perioperative patients lack the exact words to explain the way they feel or their worries. This narration has helped me in understands the needs, the struggles and the services needed by the patients, especially those under preoperative care (Wagner et al., 2010).
From this narration, I have learnt that the most affected individuals during illness, dying and death are friends and the close relatives. From the narration, it is evident that healthy people are usually distressed and have unimaginable fear about illness, especially in chronic illness such as lupus. For instance, the narration indicates that the patient friend got confused and may felt helpless during the treatment regimes. However, as indicated in Maggie’s case study of hope in recovery, it is important for the family to understand, and to find ways they can meaningfully participate in their patient’s recovery, and to understand that their acceptance positively impact the response of their loved ones. The family have crucial role especially in hospital settings. They must a way to advocate for quality care for the loved ones (Atkinson & Coia, 2012).
As indicated in Maggie’s story of hope in recovery case study and Christine’s story of the twelve spoons, the healthcare role in managing patients goes beyond offering quality care alone. I have learnt that the healthcare providers have additional role to care giving which includes educators, advocates, and counselors. The healthcare staffs have the responsibility of helping the patients to understand the disease they are suffering from, and to ensure they understand and accept the management of their condition. This activity is important as it builds the gap between the healthcare providers and the patient. Additionally, it offers emotional support that will help the patient cope with the illnesses (Bennet et al., 2010).
References
Atkinson,J.M., & Coia, D.A. (2012). Responsibility to carers — an ethical dilemma. Psychiatric Bulletin 11/1989; 13(11):602-604. DOI: 10.1192/pb.13.11.602
Bennet, A., Coleman, E., Parry, C., Bodenheimer, T., and Chen, E. (2010). Health Coaching for Patients With Chronic Illness. Fam Pract Manag. 2010 Sep-Oct;17(5):24-29.
Gold, M., Philip, J., McIver, S., & Komesaroff, P. A. (2009). Between a rock and a hard place: exploring the conflict between respecting the privacy of patients and informing their carers. Internal Medicine Journal, 39(9), 582-587. doi:10.1111/j.1445-5994.2009.02020.x
Litwack, K. (2009). Clinical coach for effective perioperative nursing care. F.A. Davis Company. Philadelphia
Lim, J., Bogossian, F., & Ahern, K. (2010). Stress and coping in Australian nurses: a systematic review. International Nursing Review, 57(1), 22-31. doi:10.1111/j.1466-7657.2009.00765.x
Tilse, C., & Wilson, J. (2013). Recognising and responding to financial abuse in residential aged care. The Journal of Adult Protection, 15(3), 141-152. doi:http://dx.doi.org/10.1108/JAP-11-2012-0025
Wagner, G., Lorenz, K.A., Riopelle, D., Steckart, M.J., Rosenfeld, K. (2010). Provider Communication and Patient Understanding of Life-Limiting Illness and Their Relationship to Patient Communication of Treatment Preferences. Journal of pain and symptom management ; 39(3):527-34. DOI: 10.1016/j.jpainsymman.2009.07.012
We can write this or a similar paper for you! Simply fill the order form!
Medication Adherence and Disease Management Order Instructions: We suggest that you develop and outline and use the following time-line as your guide for completing your paper: Week 1: Review the requirements for the paper.
Medication Adherence and Disease Management
Week 2: Begin developing an outline for your paper.
Week 3: You should have your outline completed.
Week 4: You should be using your outline to write your paper.
Week 5: Continue work on your paper.
Week 6: Finalize your paper and submit by the end of the week.
Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page.
Information on using an outline and writing a scholarly paper is available through the Excelsior College Online Writing Lab (OWL).
If you have questions, reach out to your instructor via My Messages.
linked item M6A3: Making a Safe Transition Paper
In December 2014, changes were made in Medicare payment rules. Hospitals are now penalized when a patient returns within 30 days for treatment of the same problem. One of the targeted medical diagnoses for this payment change is chronic obstructive pulmonary disease (COPD). Therefore, it is essential that the interdisciplinary team be utilized to ensure a safe transition between the acute care setting and home for the patient with COPD.
Using APA format, write a six (6) to ten (10) page paper (excludes cover and reference page) that addresses the disease management needs of adult patients with COPD for a safe transition between the acute care setting and home and the role of the interdisciplinary team in that transition.
A minimum of three (3) current professional references must be provided. Current references include professional publications or valid and current websites dated within five (5) years. Additionally, a textbook that is no more than one (1) edition old may be used.
The paper will consist of four (4) parts and must be submitted by the close of week 6.
Parts 1, 2, and 3 will focus on a disease management issue for the patient with COPD and the role of the interdisciplinary team in this issue.
Part 4 is the conclusion and needs to evaluate the effectiveness of the interdisciplinary team in making this a safe transition for the patient with COPD.
Part 1: Medication Adherence
Medication Adherence and Disease Management Essay Paper Guidelines
Part 1 must include the following:
Two common classes of medications used to manage COPD are bronchodilators and corticosteroids. Why are these medications used to manage COPD?
What are some common side effects of these classes of medications? Which of these side effects would be reported and why? Which side effects would not be reported and why?
Describe any special instructions that would be included with each class of these medications. For example, food-drug interactions and medications that should be avoided.
Which health care discipline, in addition to the RN, is best suited to help with medication adherence? How will this team member collaborate with the RN, the patient and the family to help promote medication adherence and a safe transition to home?
Part 2: Dietary Modifications
Part 2 must include the following:
What is the role of diet in managing COPD? What changes need to be made to the present diet? What role does culture play with diet?
What obstacles might be encountered when informing the patient about the changes in diet?
Which health care discipline, in addition to the RN, is best suited to help with dietary modifications? How will this team member collaborate with the RN, the patient and the family to help promote healthy eating and a safe transition to home?
Part 3: Physical Activity
Part 3 must include the following:
What is the role of physical activity in managing COPD?
How would the RN promote adherence to a daily activity routine?
Which health care discipline , in addition to the RN, are best suited to help with physical activity? How will this (these) team member collaborate with the RN, the family and the patient to help promote physical activity and a safe transition home?
Part 4: Conclusion
Part 4 must include the following:
A detailed conclusion that includes an evaluation of the effectiveness of the interdisciplinary team in making a safe transition for the patient with COPD.
Compose your work using a word processor (or other software as appropriate) and save it frequently to your computer. Use a 12 font size, double space your work and use APA format for citations, references, and overall format.
Medication Adherence and Disease Management Sample Answers
Introduction
Changes have been done in the public medical cover including Medicare and Medicaid rules. This includes the penalizing of hospitals whenever a patient is readmitted within one month of treatment of the health complication. One of the health care medications impacted by this change is Chronic Obstructive Pulmonary Disease (COPD). This calls for utilization interdisciplinary strategies to ensure that COPD patients have a safe transition from acute care settings to home (Bryant t al., 2013). This paper addresses these strategic interdisciplinary interventions that focus on the disease management including medication adherence, dietary modifications, and physical activity. The paper concludes by evaluating the effectiveness of the interdisciplinary team in ensuring safe transition.
Medication adherence
According to statistics from the World Health Organization (WHO), 210 people are diagnosed with COPD. Research estimates that COPD prevalence rates are 9-10%, which is expected to increase by three folds by 2030. This is attributable to the increase in the aging population and tobacco use. Evidence based research indicates that interdisciplinary management of COPD improves patients quality of life, and reduces the progression of the disease considerably. The main challenge in the management of COPD is medication adherence, which often gets suboptimal (Troosters Et al., 2013).
The common medication used to manage COPD includes bronchodilator drugs. This class of medication aids by making it easier to breath. The medication action involves the widening of the lungs and relaxation of the bronchi. The main goal of this treatment is to relief disease symptoms by treating flare-ups. The short acting bronchodilators include pirbuterol, albuterol and ipratropium. The drug offers quick relief of breath shortness. The Long acting bronchodilators include tiotropium and formoterol (Bryant t al., 2013). Beta 2 agonists and anti-cholinergic are the most common types of bronchodilators and the anti-cholinergic. The Beta 2 agonist mechanism of action is through the stimulation of the beta 2 receptor cells in the airways muscles, making them to relax and dilate. Anti-cholinergic blocks the cholinergic nerves responsible for secretion of bio-molecules, which causes the bronchi muscles tighten. Examples include glycopyrronium. The side effects of the bronchodilators vary according to each medication, but the general side effects are dryness in the mouth, diarrhea, palpitations, headaches and muscle cramps (Balsamo, Lanata & Egan, 2010).
Corticosteroids are also effective in the management of COPD. This is medication is particularly important in the management of the inflamed airways and increased mucus production. Examples of corticosteroids include prednisione, prednisolone and methylprednisolone. The medication mechanism of action is through anti-inflammatory action, particularly by redistributing granulocytes. Additionally, the drug regulates protein synthesis responsible for metabolic functions that often lead to inflammation. This causes reversal of mucosal edema, reducing the secretion of secretagogue, which in turn reduces the vascular permeability by inhibiting LTC4 and LTD4. This causes reliefs the disease symptoms. The general side effects include weigh gain, mood swings, acne, high blood pressure, and osteoporosis (Adams, 2010).
These medications effectively work if coupled with other disease management strategies such as dietary modifications. The patient is expected to take balanced diets. The patient diet should consume low fats but with high protein content. The COPD patient is encouraged to take whole grain meals such as oats, bran and brown rice, because they have high mineral content. The patient should also take many fruits including tomatoes, asparagus, and bananas. The diets restricted in both medications are use of salt, and reduction of taking caffeinated drinks, tobacco use, and alcohol. Despite the advantages of milk, in COPD patients increases mucus production. Therefore, dairy products should be minimized in COPD patients. Crucifeoru vegetables, especially from the cabbage families should be avoided as they cause bloating, which causes it difficult to breath. Fried foods should also be limited to minimize the bloating incidents. This is similar with carbonated beverages, which can reduce gas. This is because the interaction of the medication with these restricted substances at molecular level causes toxic reaction (Bryant t al., 2013).
Other than dietary, medication adherence is key factor in ensuring management of COPD. Non-adherence is the leading cause for readmission among the COPD patient. Most of the non-adherence is unintentional and intentional because of patient knowledge deficit. Therefore, the registered nurses have a huge role to play in ensuring that patients are empowered. This involves patient and caregiver education on the objectives of treatments and disease impact on medication non-adherence. Other than registered nurses, patient caregivers and relatives have important role in ensuring that medication is administered and adhered to, as required. These people should be integrated when planning for COPD disease and the implementation of the care plan. This will ensure that patient adheres to medication even at their home place, thus promoting a safe transition from acute setting to home (Adams, 2010).
Dietary modifications and Medication Adherence and Disease Management
Dietary is one of the main aspects of health care management strategies. Proper medication is important because it reduces the levels of carbon dioxide levels, thus aids in easy breathing. COPD patients should be advised to focus on the ratio of fat, protein and carbohydrate contents in their diets. This is because these medications influence the respiratory quotient i.e. the ratio of oxygen and carbon dioxide. This is because these fats undergo aerobic respiration, where they are converted to energy, carbon dioxide, and water. The RQ for carbohydrates, fats, and proteins is 1, 0.7, and 0.8 respectively. The highest carbon dioxide yield is associated with high intakes of carbohydrates, thus COPD patient diets should have low amounts of carbohydrates. Some medications such as prednisone have impacts on COPD patient appetite. Therefore, patients should seek advice from their physicians if feeding change is observed (Yamalz et al., 2015).
Patients are also encouraged to take high intakes of fluids, about 6 to 8 ounces of water every day. These fluids should not be carbonated or caffeinated. This is to reduce stomach upset and mucus concentration respectively, making it easy for the patients to cough up and to breathe with ease. Additionally, these fluids interfere with the medication molecular level. Patients should take high vegetable, whole grain and legumes as described previously. This is to minimize heartburns, bloating and shortness of breath. COPD patients should avoid intake of salts as it alters the homeostatic condition, causing high retention of fluid in the lungs, which causes difficulty in breathing. The patients should also avoid taking food that causes allergic reaction as they could lead to bloating making it difficult to inhale. The patient should also be given potassium, calcium and Magnesium (Bryant et al., 2013).
These dietary guidelines face various challenges including economic constraints. The best dietary diets recommended for COPD patient are organic foods. These feeds are costly and may not be affordable and easily accessible. The cultural barriers and knowledge deficit are other challenges faced by COPD patient. This is because the patient lacks information of cheap organic alternatives. In some cultures, some food products such as dairy products are used in all dishes. The most recommended cultural food is the Mediterranean diets (Adams, 2010).
The RN should work in partnership with the patient’s caregiver, relatives and healthcare nutritionist can improve COPD patients in identifying the right dietary that is individualized. This way, the patient gets empowered and even as he or she is undergoing transition for acute settings to home is safe and effective (Kuzma et al., 2008).
Medication Adherence and Disease Management and Physical activity
Physical activeness is important in the management of COPD. This is because physical activeness is associated with the rehabilitation of the pulmonary. Pulmonary rehabilitation describes the process where patients are shown activities that make it easier to breathe. This process involves counseling as well as training on the techniques that aid in breathing technique. This includes activities such as Aerobic exercises, which facilitates blood circulation, ensuring that all vital organs have ample supply of oxygen. Physical activeness also reduces cholesterol levels, hypertension and enhances the flexibility of joints. Physical activeness is associated with improved self-image and self esteem (Gimeno-Santos et al., 2014).
The most common physical activities include stretching four limbs. This improves activity, and reduces muscles injuries and muscles strains. Cardiovascular training strengthens the heart activity and the lungs activity. This improves the rates oxygen utilization reducing breath shortness (Kuzma et al., 2008).
The registered nurses should work in partnership with the physiotherapy to understand the patient’s physiological function, which can be used when designing individualized care plan. This helps in identifying the activity that the COPD patient can manage with ease, and address barriers to physical activeness. The Physical activity therapist is able to identify the subjective and objective measures that can used on patients, and to ensure that they comply with the care plan. The caregivers and relatives can also help the COPD patients take short walks around the neighborhood, swimming, and jogging. This ensures that physical activeness is maintained even at home, thus facilitating safe transition process (Adams, 2010).
Medication Adherence and Disease Management Conclusion
COPD disease is life threatening, but it can be managed and prevented. The underlying concept of COPD exacerbation is due to unhealthy lifestyles including poor dietary, smoking, and physical inactivity. From systematic analysis of management of COPD diseases, the most intervention recommended includes behavioral modifications including healthy diets, increase in physical activity and reduction of tobacco use and alcohol. Thus, it can be concluded that COPD exacerbation is attributable to habitual factors, and thus to effectively manage safe acute settings and home transition of COPD patients, multi-factorial approach is effective strategic. This is because COPD is incurable, chronic, and most importantly, it affects the vital organs of the body (Troosters Et al., 2013).
This also calls for working in partnership among various healthcare stakeholders including pharmacists, patients, RN, occupation therapists, respiratory physicians, and nutritionists. They should work towards achievement of one goal, which is improving patient quality of life. This minimizes medication errors and reinforces on individualized patient’s care plan. Therefore, the aforementioned multidisciplinary effectiveness should be evaluated at every treatment, and based on the findings; the interventions can be modified to meet the patient demands (Kuzma et al., 2008).
Medication Adherence and Disease Management References
Adams, S. (2010). Integrated management strategies for chronic obstructive pulmonary disease. Journal of Multidisciplinary Healthcare, p.181.
Balsamo, R., Lanata, L. and Egan, C. (2010). Mucoactive drugs. European Respiratory Review, 19(116), pp.127-133.
Bryant, J., McDonald, V., Boyes, A., Sanson-Fisher, R., Paul, C. and Melville, J. (2013). Improving medication adherence in chronic obstructive pulmonary disease: a systematic review. Respiratory Research, 14(1), p.109.
Gimeno-Santos, E., Frei, A., Steurer-Stey, C., de Batlle, J., Rabinovich, R., Raste, Y., Hopkinson, N., Polkey, M., van Remoortel, H., Troosters, T., Kulich, K., Karlsson, N., Puhan, M. and Garcia-Aymerich, J. (2014). Determinants and outcomes of physical activity in patients with COPD: a systematic review. Thorax, 69(8), pp.731-739.
Kuzma, A., Meli, Y., Meldrum, C., Jellen, P., Butler-Lebair, M., Koczen-Doyle, D., Rising, P., Stavrolakes, K. and Brogan, F. (2008). Multidisciplinary Care of the Patient with Chronic Obstructive Pulmonary Disease. Proceedings of the American Thoracic Society, 5(4), pp.567-571.
Troosters, T., van der Molen, T., Polkey, M., Rabinovich, R., Vogiatzis, I., Weisman, I. and Kulich, K. (2013). Improving physical activity in COPD: towards a new paradigm. Respiratory Research, 14(1), p.115.
Yalmaz, D., Ãapan, N., Canbakan, S. and Besler, H. (2015). Dietary intake of patients with moderate to severe COPD in relation to fat-free mass index: a cross-sectional study. Nutr J, 14(1).
Transitional Management for Adult Patients of Chronic Obstructive Pulmonary Disease (COPD)
Order Instructions:
Using APA format ,write six (6) to ten page paper (excludes covers and references pages) that addresses the disease management needed of adult patients with COPD for a safe transition between the acute care setting and home and the role of the interdisciplinary team in that transition.
SAMPLE ANSWER
Transitional Management for Adult Patients of COPD
Chronic Obstructive Pulmonary Disease (COPD) is an incurable medical condition that is more prevalent in older people than in the young. Even though COPD is incurable, it is possible to minimize the severity of its symptoms by structuring optimal management techniques. Such practices should minimize the rate of disease progress and offer patients a chance to lead high-quality lives. However, it is often challenging to ensure that patients receive optimal management for the disease, more so when they are leaving acute care centers for their homes. There are important approaches to consider in ensuring that patients practice the recommended strategies for managing COPD at their homes. The activity would involve an interdisciplinary collaboration between professionals in the healthcare setup.
Part 1: The Use of Bronchodilators and Corticosteroids in the Management of COPD
Why They are Used
Bronchodilators and corticosteroids are effective in the alleviation of clinical symptoms of COPD. Bronchodilators such as salmetrol, formoterol, and tiotropium work on a long-term basis to enhance lung functionality and reduce the occurrence and severity of exacerbations, hence improving patient’s quality of life. The drugs also enhance patient’s tolerance to exercises and improve protect them from lung hyperinflation as well as dyspnea (Tashkin, & Ferguson, 2013). Drugs such as indacaterol and aclidinium are new developments that require less dosage frequencies hence reducing chances of drug non-adherence among patients. Other bronchodilators with lengthy frequencies of intake include glycopyrrolate, vilanterol, and olodaterol (Tashkin, & Ferguson, 2013).
Corticosteroids are also important medications in the management of exacerbations experienced in COPD. Nebulized budesonide is not only a primary care corticosteroid in managing OCPD in adults, but it is also the drug of choice for children with COPD. Clinicians prefer the drug on the basis of its considerably less severe side effects compared to those associated with the use of other steroids (Gaude, & Nadagouda, 2010, Pg. 230). Timely administration of corticosteroids also results in improved functionality of the lungs. Some glucocorticoids also find use in reducing inflammation. They act by inhibiting the genetic pathway leading to the production of inflammatory mediators such as chemokines and cytokines (Gaude, & Nadagouda, 2010, Pg. 231). Instead, they promote the production of anti-inflammatory molecules such as beta-2 adrenoceptors. Through such a mechanism, glucocorticoids reduce swelling and exudation on the airway hence enhancing the respiratory system.
Side Effects of Corticosteroids and Bronchodilators
The use of corticosteroids has adverse effects such as sleep abnormalities, exaggerated appetite, and weight gain. They also subject adult users to ailments such as osteoporosis, diabetes, pneumonia, hypertension, cardiac anomalies, cataracts, and peptic ulcers (Gaude, & Nadagouda, 2010, Pg. 232). The side effects are severer when patient are on oral and parenteral treatment with corticosteroids as compared to when they take inhaled and nebulized formulations. The prevalence of the undesirable effects also increases with the dosage amount. Bronchodilators also have associated adversities. They include muscle crumps, headache, dizziness, nausea, vomiting, palpitations, and cardiac abnormalities (Cleveland Clinic, 2014a). Patients should report severe critical side effects so that prescribers can substitute their regimens with others that have minimal adversities. Occurrences such as hypertension, severe headaches, persistent vomiting are worth reporting as they may indicate the development of other critical conditions such as cardiac diseases and peptic ulcers. Patients may not have to report effects such as dizziness, nausea, and minor headaches as such complications are common with most medications. Besides, such symptoms are often temporary, and they would rarely indicate serious clinical adverse conditions.
Special Instructions Regarding Drug Use
Both bronchodilators and corticosteroids require special directions for their use. For instance, health professionals should advise their patient to take bronchodilators before taking other inhaled medications such as corticosteroids. Again, it is important to inform patients that they do not have to chew bronchodilator tablets, and instead, they should swallow them as whole. It is also necessary to inform patients on the purpose of each medication. For instance, patients should know that bronchodilators help them overcome shortness of breath associated with COPD. Some of the additional directions also apply to the use of corticosteroids. For instance, patients would always require taking bronchodilators first when they are co-administered with steroids. For corticosteroids, patients should know that they require rinsing their mouth with clean water to minimize the occurrence of side effects such as nausea. Also, it is important to inform the patient that unlike bronchodilators, corticosteroids take a considerably longer time to work, and they are not applicable for instant relief of COPD symptoms. Again, patients should know that corticosteroids may not stop attacks that have already started (Cleveland Clinic, 2014b).
An Important Healthcare Discipline that would Facilitate Medication Adherence
Medication adherence entails the degree of compliance with the recommended drug use practices. So as to ensure optimal treatment adherence among patients, various healthcare disciplines should collaborate. Among such disciplines are the nursing and pharmacy departments. Nurses have most interactions with patients as their primary role is to monitor patients. On the other hand, pharmacists are the custodians of drug use, and they would be relevant in promoting adherence to medications. Pharmacists should cooperate with nurses to schedule follow up activities to monitor drug use among patients (Jimmy, & Jose, 2011, Pg. 156). They should for instance establish strong interactions with patients, teach them on how to use devices such as inhalers, and monitor their use of adherence devices such as calendars and reminders.
Part 2: Dietary Modification in the Management of COPD
The Role of Diet in Managing COPD
Diet is a crucial consideration in the management of COPD. Either form of malnutrition, be it excessive nutrient consumption, or low intake of the same has an undesirable impact on the pathogenesis of COPD. Dieting habits that promote the development of conditions such as obesity have severe impact on COPD development. Usually, obesity leads to other respiratory abnormalities that worsen the condition of COPD patients. Such illnesses include asthma, hypoventilation, and pulmonary embolism (Hanson, Rutten, Wouters, & Rennard, 2014, Pg. 724). On the other hand, COPD patients with advanced disease experience pulmonary cachexia, a state in which their body weight is abnormally low, and their free fatty mass is extremely reduced.
Dietary modifications would be necessary to enhance the nutritional status of patients. Malnourished COPD patient would have to rely on dietary supplements to boost their health. Alternatively, patients would have to include high-calorie foods and beverages in their dietary plans. Studies indicate that lean COPD patients should maximize their fat intake at the expense of carbohydrates (Itoh, Tsuji, Nemoto, Nakamura, & Aoshiba, 2013, Pg. 1318). Some cultures encourage consumption of meat while others discourage it. Likewise, cultures have varying influences regarding intake of fruits and vegetables.
Possible Obstacles to Dietary Modification
Patients may find it hard to adopt new dietary practices. Also, people’s living conditions may influence their ability to adopt certain therapeutic dietary approaches. Patients from poor economic backgrounds may not access the recommended dietary practices. Cultural beliefs may also influence the adoption of dietary changes. Some cultures may not encourage certain recommended dietary approaches. Patients’ taste and preferences may also hinder the adoption of dietary changes. Some nutrients are only abundant in foods that some patients may be unwilling to take. Such foods include fish and mushrooms, both which are sources of vitamin D, an element crucial for COPD patients (Itoh et al., 2013, Pg. 1320).
An Important Healthcare Discipline in Facilitating Dietary Modifications
Nurses should seek the collaboration of dieticians in promoting effective dietary modifications. COPD patients experience important nutritional complications such as appetite loss. Medical dieticians are best placed to inform patients on practices that would promote their appetite. They should offer nutrition therapy to protect patients from weight loss and attacks by COPD Comorbidities (Seo, 2014, Pg. 151). Likewise, the professionals would advise obese persons on measures they should take to avoid worsening their health status. Dieticians should also collaborate with the families of patients by advising them on the foods that their patients may need as well as the ones they should avoid.
Part 3: Physical Activity in COPD Management
The Role of Physical Activity in COPD Management
While it is advisable for people to engage in physical exercises, COPD patients should maintain their level of involvement to a certain level. Too much strenuous activities may have adverse consequences in the population. The pathophysiology of COPD involves dyspnea, a condition that may worsen with engagement in exercises. Simple exercises are however necessary to ensure that patient’s respiratory system is strengthened. Energy conservation is crucial in COPD patients both in the sense that the victims could easily ran malnourished and also considering the appropriate management of dyspnea. Recommended physical exercises for the group include diaphragmatic and pursed-lip forms of breathing techniques (Broward Health, 2015). COPD patients also require physical exercises for psychological health. There are multiple factors that would predispose the group to stress, depression, and anxiety. The knowledge of having a chronic ailment is among such factors. Also, experiences of dyspnea and its associated discomfort would easily trigger anxiety. Patient would need keeping themselves busy through exercises so as to overcome such events.
The Role of RN in Promoting Effective Physical Practices in COPD Management
Registered nurses prioritize on the welfare of patients. They should structure an exercise strategy that would not harm but benefit patients. They would do so by warning patients against engagement in strenuous activities and advise them on appropriate activities they should explore. Nurses should also monitor the performance of their patients to help them maintain healthy physical conditions. Nurses should educate patients on activities that would promote their pulmonary system. Such advice should also entail practices that patients should engage in so as to overcome symptoms such as dyspnea. Also, nurses should advise patients on relaxation strategies that would promote healthy air flow in their systems.
An Essential Healthcare Discipline in Facilitating the Healthy Physical Activities
Physical therapists would be relevant professionals in enhancing the effectiveness of physical activity in the management of COPD patients. The specialists should collaborate with nurses in ensuring that COPD patients are at their optimum physical health. Physical therapists should teach patients on how to perform various exercises in a safe manner. COPD patients often have a delicate physical health, and the specialists should purpose to promote their (patients’) stability. Also, it is important for physical therapists and nurses to engage patients’ family members in strategizing physical activities for their patients. They should encourage patients’ family members to support their loved ones in exercising. Families would do so by monitoring their patients as they engage in various activities. They could also contribute by helping patients to undertake manual activities that could otherwise trigger hypoventilation and dyspnea in the high-risk group.
Part 4: Conclusion
The Effectiveness of an Interdisciplinary Team in Managing COPD
It is important to maintain the quality of care for COPD patients at a high level, especially during transitions from hospital care to home-based attendance. The process involves various considerations ranging from medication adherence, dietary practices, and the performance of physical activities. As such, the process would require various clinical professionals to cooperate for high-quality outcomes. Engaging nursing care and other relevant specialties in the transition would be a promising move. The team should work jointly with the common goal of bettering patient outcomes. A team involving specialties from the most relevant departments and professions would be effective in achieving utmost patient satisfaction and fetching desirable outcomes. It is also vital that such a team involve the families of patients. The extent of patient satisfaction would be a reflection of the ultimate achievements of the interdisciplinary team involved in the entire process.
Gaude, G. S., & Nadagouda, S. (2010). Nebulized corticosteroids in the management of acute exacerbation of COPD. Lung India : Official Organ of Indian Chest Society, 27(4), 230–235. http://doi.org/10.4103/0970-2113.71957
Hanson, C., Rutten, E. P., Wouters, E. F., & Rennard, S. (2014). Influence of diet and obesity on COPD development and outcomes. International Journal of Chronic Obstructive Pulmonary Disease, 9, 723–733. http://doi.org/10.2147/COPD.S50111
Itoh, M., Tsuji, T., Nemoto, K., Nakamura, H., & Aoshiba, K. (2013). Undernutrition in Patients with COPD and Its Treatment . Nutrients, 5(4), 1316–1335. http://doi.org/10.3390/nu5041316
Jimmy, B., & Jose, J. (2011). Patient Medication Adherence: Measures in Daily Practice. Oman Medical Journal, 26(3), 155–159. http://doi.org/10.5001/omj.2011.38
Seo, S. H. (2014). Medical Nutrition Therapy based on Nutrition Intervention for a Patient with Chronic Obstructive Pulmonary Disease. Clinical Nutrition Research, 3(2), 150–156. http://doi.org/10.7762/cnr.2014.3.2.150
Tashkin, D. P., & Ferguson, G. T. (2013). Combination bronchodilator therapy in the management of chronic obstructive pulmonary disease. Respiratory Research, 14(1), 49. http://doi.org/10.1186/1465-9921-14-49
We can write this or a similar paper for you! Simply fill the order form!