In this assignment, you will consider how workforce issues impact on patient safety.
Discussion Question 1
Using the an Online Library, research workforce issues and patient safety.
Based on your research, complete the following tasks:
•Identify and describe the research problems, purpose, objectives, and hypothesis of the research.
•Evaluate the credibility and validity of the study.
Discussion Question 2
Read the following titles of research studies from an Online Library. Identify the type of research used in each study (qualitative or quantitative). Provide a rationale for your selection.
•A study of the effects of cardiac rehabilitation exercise program on the morale and motivation of persons recovering from recent heart attacks.
•An exploratory ethno-botanical study of medicinal plants used by the Turks in the treatment of eye disorders.
•A study of the impact of different dietary patterns on breast cancer patients.
•The effectiveness of the acquired immunodeficiency syndrome (AIDS) Drug Assistance Program (ADAP).
•A study of the effects of different types of music on sleeping patterns of elderly insomnia patients.
•A study of the impact of political and social trends on the direction of nursing research.
Suggested References:
Shisana, O., Rice, K., Zungu, N., & Zuma, K. (2010). Gender and poverty in South Africa in the era of HIV/AIDS: A quantitative study. Journal of Women’s
Health (15409996), 19(1), 39–46.
Ko, E., Nelson-Becker, H., Park, Y., & Shin, M. (2013). End-of-Life decision making in older Korean adults: Concerns, preferences, and expectations. Educational
Gerontology, 39(2), 71–81.
Witzke, J., Rhone, R., Backhaus, D., & Shaver, N. (2008). How sweet the sound: Research evidence for the use of music in Alzheimer’s dementia. Journal of Gerontological Nursing, 34(10), 45–52.
Sandvik, A., Melender, H., Jonsén, E., Jönsson, G., Salmu, M., & Hilli, Y. (2012).
Nursing students’ experiences of the first clinical education: A nordic quantitative study. Nordic Journal of Nursing Research & Clinical Studies /Vård I Norden, 32(3), 20–25.
Cooper, C., Taft, L., & Thelen, M. (2004). Examining the role of technology in learning: An evaluation of online clinical conferencing. Journal of Professional Nursing, 20(3), 160–166.
Roulston, A., Bickerstaff, D., Haynes, T., Rutherford, L., & Jones, L. (2012). A pilot study to evaluate an outpatient service for people with advanced lung cancer. International Journal of Palliative Nursing, 18(5), 225–233.
SAMPLE ANSWER
Workforce Issues on Patient Safety
Discussion question 1
Patient safety in many health institutions faced challenges that relates to workforce issues. Various studies demonstrate that in deed measures are required to make some improvements in the workforce to enhance the level of patient safety. In the study, “The effects of workforce issues on patient safety” by Gelinas and David (2004) it is clear that there are number of issues that relates to the workforce that affects the safety of patients in the health centers.
The research problem in this study is lack of focus to relevant workforce issues hence leading to injuries and poor patient safety. The purpose of the study was to provide an insight on the failures in the health facilities such as staff retention, competency development and orientation and training issues that compromise on the patient safety. The objectives of the study were to provide amicable solutions to the problems that face workforce in health care. Other objective is to ensure that there is good leadership in the hospitals to provide motivation to the workforce. Cultural aspects as well require a redress to enhance transformation in health facilities to enhance patient safety. The study hypothesis is inferred and is to promote positive values among workforce and motivate them to reduce patient injury.
Validity and credibility of a study matters a lot credibility of the study compels people to adopt the study as they have confidence in it. The study is credible as it incorporates credible sources of reference. It is well supported with statistic from other studies that makes it credible. Professionals as well carried out the study. The study as well incorporated evidences from various public reports, which makes it credible (Gelinas & David, 2004). The study validity is as well evident with the use of authoritative information and models. Information is well researched and proved. The fact the study was approved to be included in the database, is a clear indication that it meet the threshold of validity and credibility.
Discussion Question 2
Researchers decide to adopt to different research designs either qualitative and quantitative or mixed depending on the nature of the study. Some of the topics of study can be well understood through any of these study designs (Rofail, Maguire, Kissner, Colligs & Abetz-Webb, 2014). The topics of these studies as well can provide some insights to the research study adopted. Studies in relation to effects of cardiac rehabilitation exercise program on the morale and motivation of persons recovering from recent heart attacks uses qualitative research designs. The reason for adoption of this design is that it generates information through interviews that can be explained and described to enhance understanding (Mayberry & Kent, 1983). Researcher can observe the patients as well as interrogate them to determine whether they are motivated or their morale has increased after exposure to rehabilitative exercise. Other studies that adopt qualitative design include, A study of the effects of different types of music on sleeping patterns of elderly insomnia patients and A study of the impact of political and social trends on the direction of nursing research. These studies do not require reliance of statistics or to present the findings using statistics.
On the other hand, some studies require adoption of quantitative study designs for the findings to be of great value and assistance. Examples of these studies may includes an exploratory ethno-botanical study of medicinal plants used by the Turks in the treatment of eye disorders, a study of the impact of different dietary patterns on breast cancer patients and The effectiveness of the acquired immunodeficiency syndrome (AIDS) Drug Assistance Program (ADAP). These studies require presentation of data using numerical statistics to enhance their understanding.
Drawing on the theories and strategies of change you learned about this week, consider how you, as a leader, would foster change that you think is needed within this organization as well as within your community.
Answer the following Questions:
1. Describe steps to take to foster the change process in your selected organization. Provide a rationale for these steps from this week’s Learning Resources. What challenges would you expect, and how would you deal with them?
2. Compare and contrast this with the steps you would take to foster the change process in your own community to positively impact public health. Again, provide support for your assertions. Explain any challenges you think might arise from this process and the ways in which you would use change theory to bring about positive results.
USE THESE ARTICLES ONLY
1. Kotter, J. P. (2007). Leading change. Harvard Business Review, 85(1), 96-103.
This articles shares the author’s research findings surrounding a ten-year study concerning how businesses cope with changing business trends while attempting to maintain market leverage.
2. Senge, P. M. (1990). The leader’s new work: Building learning organizations. Sloan Management Review, 32(1), 7-23.
This article describes the skills and tools needed by public health leaders who want to develop learning organizations that encompass creative tension while managing corporate change.
Leading Change
Section: BEST OF HBR | 1995 THE TESTS OF A LEADER
Why Transformation Efforts Fail
Editor’s Note: Guiding change may be the ultimate test of a leader — no business survives over the long term if it can’t reinvent itself. But, human nature being what it is, fundamental change is often resisted mightily by the people it most affects: those in the trenches of the business. Thus, leading change is both absolutely essential and incredibly difficult.
Perhaps nobody understands the anatomy of organizational change better than retired Harvard Business School professor John P. Kotter. This article, originally published in the spring of 1995, previewed Kotter’s 1996 book Leading Change. It outlines eight critical success factors — from establishing a sense of extraordinary urgency, to creating short-term wins, to changing the culture (“the way we do things around here” ). It will feel familiar when you read it, in part because Kotter’s vocabulary has entered the lexicon and in part because it contains the kind of home truths that we recognize, immediately, as if we’d always known them. A decade later, his work on leading change remains definitive.
Leaders who successfully transform businesses do eight things right (and they do them in the right order).
OVER THE PAST DECADE, I have watched more than 100 companies try to remake themselves into significantly better competitors. They have included large organizations (Ford) and small ones (Landmark Communications), companies based in the United States (General Motors) and elsewhere (British Airways), corporations that were on their knees (Eastern Airlines), and companies that were earning good money (Bristol-Myers Squibb). These efforts have gone under many banners: total quality management, re-engineering, rightsizing, restructuring, cultural change, and turnaround. But, in almost every case, the basic goal has been the same: to make fundamental changes in how business is conducted in order to help cope with a new, more challenging market environment.
A few of these corporate change efforts have been very successful. A few have been utter failures. Most fall somewhere in between, with a distinct tilt toward the lower end of the scale. The lessons that can be drawn are interesting and will probably be relevant to even more organizations in the increasingly competitive business environment of the coming decade.
The most general lesson to be learned from the more successful cases is that the change process goes through a series of phases that, in total, usually require a considerable length of time. Skipping steps creates only the illusion of speed and never produces a satisfying result. A second very general lesson is that critical mistakes in any of the phases can have a devastating impact, slowing momentum and negating hard-won gains. Perhaps because we have relatively little experience in renewing organizations, even very capable people often make at least one big error.
Error 1: Not Establishing a Great Enough Sense of Urgency
Most successful change efforts begin when some individuals or some groups start to look hard at a company’s competitive situation, market position, technological trends, and financial performance. They focus on the potential revenue drop when an important patent expires, the five-year trend in declining margins in a core business, or an emerging market that everyone seems to be ignoring. They then find ways to communicate this information broadly and dramatically, especially with respect to crises, potential crises, or great opportunities that are very timely. This first step is essential because just getting a transformation program started requires the aggressive cooperation of many individuals. Without motivation, people won’t help, and the effort goes nowhere.
Compared with other steps in the change process, phase one can sound easy. It is not. Well over 50% of the companies I have watched fail in this first phase. What are the reasons for that failure? Sometimes executives underestimate how hard it can be to drive people out of their comfort zones. Sometimes they grossly overestimate how successful they have already been in increasing urgency. Sometimes they lack patience: “Enough with the preliminaries; let’s get on with it.” In many cases, executives become paralyzed by the downside possibilities. They worry that employees with seniority will become defensive, that morale will drop, that events will spin out of control, that short-term business results will be jeopardized, that the stock will sink, and that they will be blamed for creating a crisis.
A paralyzed senior management often comes from having too many managers and not enough leaders. Management’s mandate is to minimize risk and to keep the current system operating. Change, by definition, requires creating a new system, which in turn always demands leadership. Phase one in a renewal process typically goes nowhere until enough real leaders are promoted or hired into senior-level jobs.
Transformations often begin, and begin well, when an organization has a new head who is a good leader and who sees the need for a major change. If the renewal target is the entire company, the CEO is key. If change is needed in a division, the division general manager is key. When these individuals are not new leaders, great leaders, or change champions, phase one can be a huge challenge.
Bad business results are both a blessing and a curse in the first phase. On the positive side, losing money does catch people’s attention. But it also gives less maneuvering room. With good business results, the opposite is true: Convincing people of the need for change is much harder, but you have more resources to help make changes.
But whether the starting point is good performance or bad, in the more successful cases I have witnessed, an individual or a group always facilitates a frank discussion of potentially unpleasant facts about new competition, shrinking margins, decreasing market share, flat earnings, a lack of revenue growth, or other relevant indices of a declining competitive position. Because there seems to be an almost universal human tendency to shoot the bearer of bad news, especially if the head of the organization is not a change champion, executives in these companies often rely on outsiders to bring unwanted information. Wall Street analysts, customers, and consultants can all be helpful in this regard. The purpose of all this activity, in the words of one former CEO of a large European company, is “to make the status quo seem more dangerous than launching into the unknown.”
In a few of the most successful cases, a group has manufactured a crisis. One CEO deliberately engineered the largest accounting loss in the company’s history, creating huge pressures from Wall Street in the process. One division president commissioned first-ever customer satisfaction surveys, knowing full well that the results would be terrible. He then made these findings public. On the surface, such moves can look unduly risky. But there is also risk in playing it too safe: When the urgency rate is not pumped up enough, the transformation process cannot succeed, and the long-term future of the organization is put in jeopardy.
When is the urgency rate high enough? From what I have seen, the answer is when about 75% of a company’s management is honestly convinced that business as usual is totally unacceptable. Anything less can produce very serious problems later on in the process.
Error 2: Not Creating a Powerful Enough Guiding Coalition
Major renewal programs often start with just one or two people. In cases of successful transformation efforts, the leadership coalition grows and grows over time. But whenever some minimum mass is not achieved early in the effort, nothing much worthwhile happens.
It is often said that major change is impossible unless the head of the organization is an active supporter. What I am talking about goes far beyond that. In successful transformations, the chairman or president or division general manager, plus another five or 15 or 50 people, come together and develop a shared commitment to excellent performance through renewal. In my experience, this group never includes all of the company’s most senior executives because some people just won’t buy in, at least not at first. But in the most successful cases, the coalition is always pretty powerful — in terms of titles, information and expertise, reputations, and relationships.
In both small and large organizations, a successful guiding team may consist of only three to five people during the first year of a renewal effort. But in big companies, the coalition needs to grow to the 20 to 50 range before much progress can be made in phase three and beyond. Senior managers always form the core of the group. But sometimes you find board members, a representative from a key customer, or even a powerful union leader.
Because the guiding coalition includes members who are not part of senior management, it tends to operate outside of the normal hierarchy by definition. This can be awkward, but it is clearly necessary. If the existing hierarchy were working well, there would be no need for a major transformation. But since the current system is not working, reform generally demands activity outside of formal boundaries, expectations, and protocol.
A high sense of urgency within the managerial ranks helps enormously in putting a guiding coalition together. But more is usually required. Someone needs to get these people together, help them develop a shared assessment of their company’s problems and opportunities, and create a minimum level of trust and communication. Off-site retreats, for two or three days, are one popular vehicle for accomplishing this task. I have seen many groups of five to 35 executives attend a series of these retreats over a period of months.
Companies that fail in phase two usually underestimate the difficulties of producing change and thus the importance of a powerful guiding coalition. Sometimes they have no history of teamwork at the top and therefore undervalue the importance of this type of coalition. Sometimes they expect the team to be led by a staff executive from human resources, quality, or strategic planning instead of a key line manager. No matter how capable or dedicated the staff head, groups without strong line leadership never achieve the power that is required.
Efforts that don’t have a powerful enough guiding coalition can make apparent progress for a while. But, sooner or later, the opposition gathers itself together and stops the change.
Error 3: Lacking a Vision
In every successful transformation effort that I have seen, the guiding coalition develops a picture of the future that is relatively easy to communicate and appeals to customers, stockholders, and employees. A vision always goes beyond the numbers that are typically found in five-year plans. A vision says something that helps clarify the direction in which an organization needs to move. Sometimes the first draft comes mostly from a single individual. It is usually a bit blurry, at least initially. But after the coalition works at it for three or five or even 12 months, something much better emerges through their tough analytical thinking and a little dreaming. Eventually, a strategy for achieving that vision is also developed.
In one midsize European company, the first pass at a vision contained two-thirds of the basic ideas that were in the final product. The concept of global reach was in the initial version from the beginning. So was the idea of becoming preeminent in certain businesses. But one central idea in the final version — getting out of low value-added activities — came only after a series of discussions over a period of several months.
Without a sensible vision, a transformation effort can easily dissolve into a list of confusing and incompatible projects that can take the organization in the wrong direction or nowhere at all. Without a sound vision, the reengineering project in the accounting department, the new 360-degree performance appraisal from the human resources department, the plant’s quality program, the cultural change project in the sales force will not add up in a meaningful way.
In failed transformations, you often find plenty of plans, directives, and programs but no vision. In one case, a company gave out four-inch-thick notebooks describing its change effort. In mind-numbing detail, the books spelled out procedures, goals, methods, and deadlines. But nowhere was there a clear and compelling statement of where all this was leading. Not surprisingly, most of the employees with whom I talked were either confused or alienated. The big, thick books did not rally them together or inspire change. In fact, they probably had just the opposite effect.
In a few of the less successful cases that I have seen, management had a sense of direction, but it was too complicated or blurry to be useful. Recently, I asked an executive in a midsize company to describe his vision and received in return a barely comprehensible 30-minute lecture. Buried in his answer were the basic elements of a sound vision. But they were buried — deeply.
A useful rule of thumb: If you can’t communicate the vision to someone in five minutes or less and get a reaction that signifies both understanding and interest, you are not yet done with this phase of the transformation process.
Error 4: Undercommunicating the Vision by a Factor of Ten
I’ve seen three patterns with respect to communication, all very common. In the first, a group actually does develop a pretty good transformation vision and then proceeds to communicate it by holding a single meeting or sending out a single communication. Having used about 0. 0001% of the yearly intracompany communication, the group is startled when few people seem to understand the new approach. In the second pattern, the head of the organization spends a considerable amount of time making speeches to employee groups, but most people still don’t get it (not surprising, since vision captures only 0. 0005% of the total yearly communication). In the third pattern, much more effort goes into newsletters and speeches, but some very visible senior executives still behave in ways that are antithetical to the vision. The net result is that cynicism among the troops goes up, while belief in the communication goes down.
Transformation is impossible unless hundreds or thousands of people are willing to help, often to the point of making short-term sacrifices. Employees will not make sacrifices, even if they are unhappy with the status quo, unless they believe that useful change is possible. Without credible communication, and a lot of it, the hearts and minds of the troops are never captured.
This fourth phase is particularly challenging if the short-term sacrifices include job losses. Gaining understanding and support is tough when downsizing is a part of the vision. For this reason, successful visions usually include new growth possibilities and the commitment to treat fairly anyone who is laid off.
Executives who communicate well incorporate messages into their hour-by-hour activities. In a routine discussion about a business problem, they talk about how proposed solutions fit (or don’t fit) into the bigger picture. In a regular performance appraisal, they talk about how the employee’s behavior helps or undermines the vision. In a review of a division’s quarterly performance, they talk not only about the numbers but also about how the division’s executives are contributing to the transformation. In a routine Q&A with employees at a company facility, they tie their answers back to renewal goals.
In more successful transformation efforts, executives use all existing communication channels to broadcast the vision. They turn boring, unread company newsletters into lively articles about the vision. They take ritualistic, tedious quarterly management meetings and turn them into exciting discussions of the transformation. They throw out much of the company’s generic management education and replace it with courses that focus on business problems and the new vision. The guiding principle is simple: Use every possible channel, especially those that are being wasted on nonessential information.
Perhaps even more important, most of the executives I have known in successful cases of major change learn to “walk the talk.” They consciously attempt to become a living symbol of the new corporate culture. This is often not easy. A 60-year-old plant manager who has spent precious little time over 40 years thinking about customers will not suddenly behave in a customer-oriented way. But I have witnessed just such a person change, and change a great deal. In that case, a high level of urgency helped. The fact that the man was a part of the guiding coalition and the vision-creation team also helped. So did all the communication, which kept reminding him of the desired behavior, and all the feedback from his peers and subordinates, which helped him see when he was not engaging in that behavior.
Communication comes in both words and deeds, and the latter are often the most powerful form. Nothing undermines change more than behavior by important individuals that is inconsistent with their words.
Error 5: Not Removing Obstacles to the New Vision
Successful transformations begin to involve large numbers of people as the process progresses. Employees are emboldened to try new approaches, to develop new ideas, and to provide leadership. The only constraint is that the actions fit within the broad parameters of the overall vision. The more people involved, the better the outcome.
To some degree, a guiding coalition empowers others to take action simply by successfully communicating the new direction. But communication is never sufficient by itself. Renewal also requires the removal of obstacles. Too often, an employee understands the new vision and wants to help make it happen, but an elephant appears to be blocking the path. In some cases, the elephant is in the person’s head, and the challenge is to convince the individual that no external obstacle exists. But in most cases, the blockers are very real.
Sometimes the obstacle is the organizational structure: Narrow job categories can seriously undermine efforts to increase productivity or make it very difficult even to think about customers. Sometimes compensation or performance-appraisal systems make people choose between the new vision and their own self-interest. Perhaps worst of all are bosses who refuse to change and who make demands that are inconsistent with the overall effort.
One company began its transformation process with much publicity and actually made good progress through the fourth phase. Then the change effort ground to a halt because the officer in charge of the company’s largest division was allowed to undermine most of the new initiatives. He paid lip service to the process but did not change his behavior or encourage his managers to change. He did not reward the unconventional ideas called for in the vision. He allowed human resource systems to remain intact even when they were clearly inconsistent with the new ideals. I think the officer’s motives were complex. To some degree, he did not believe the company needed major change. To some degree, he felt personally threatened by all the change. To some degree, he was afraid that he could not produce both change and the expected operating profit. But despite the fact that they backed the renewal effort, the other officers did virtually nothing to stop the one blocker. Again, the reasons were complex. The company had no history of confronting problems like this. Some people were afraid of the officer. The CEO was concerned that he might lose a talented executive. The net result was disastrous. Lower-level managers concluded that senior management had lied to them about their commitment to renewal, cynicism grew, and the whole effort collapsed.
In the first half of a transformation, no organization has the momentum, power, or time to get rid of all obstacles. But the big ones must be confronted and removed. If the blocker is a person, it is important that he or she be treated fairly and in a way that is consistent with the new vision. Action is essential, both to empower others and to maintain the credibility of the change effort as a whole.
Error 6: Not Systematically Planning for, and Creating, Short-Term Wins
Real transformation takes time, and a renewal effort risks losing momentum if there are no short-term goals to meet and celebrate. Most people won’t go on the long march unless they see compelling evidence in 12 to 24 months that the journey is producing expected results. Without short-term wins, too many people give up or actively join the ranks of those people who have been resisting change.
One to two years into a successful transformation effort, you find quality beginning to go up on certain indices or the decline in net income stopping. You find some successful new product introductions or an upward shift in market share. You find an impressive productivity improvement or a statistically higher customer satisfaction rating. But whatever the case, the win is unambiguous. The result is not just a judgment call that can be discounted by those opposing change.
Creating short-term wins is different from hoping for short-term wins. The latter is passive, the former active. In a successful transformation, managers actively look for ways to obtain clear performance improvements, establish goals in the yearly planning system, achieve the objectives, and reward the people involved with recognition, promotions, and even money. For example, the guiding coalition at a U.S. manufacturing company produced a highly visible and successful new product introduction about 20 months after the start of its renewal effort. The new product was selected about six months into the effort because it met multiple criteria: It could be designed and launched in a relatively short period, it could be handled by a small team of people who were devoted to the new vision, it had upside potential, and the new product-development team could operate outside the established departmental structure without practical problems. Little was left to chance, and the win boosted the credibility of the renewal process.
Managers often complain about being forced to produce short-term wins, but I’ve found that pressure can be a useful element in a change effort. When it becomes clear to people that major change will take a long time, urgency levels can drop. Commitments to produce short-term wins help keep the urgency level up and force detailed analytical thinking that can clarify or revise visions.
Error 7: Declaring Victory Too Soon
After a few years of hard work, managers may be tempted to declare victory with the first clear performance improvement. While celebrating a win is fine, declaring the war won can be catastrophic. Until changes sink deeply into a company’s culture, a process that can take five to ten years, new approaches are fragile and subject to regression.
In the recent past, I have watched a dozen change efforts operate under the reengineering theme. In all but two cases, victory was declared and the expensive consultants were paid and thanked when the first major project was completed after two to three years. Within two more years, the useful changes that had been introduced slowly disappeared. In two of the ten cases, it’s hard to find any trace of the reengineering work today.
Over the past 20 years, I’ve seen the same sort of thing happen to huge quality projects, organizational development efforts, and more. Typically, the problems start early in the process: The urgency level is not intense enough, the guiding coalition is not powerful enough, and the vision is not clear enough. But it is the premature victory celebration that kills momentum. And then the powerful forces associated with tradition take over.
Ironically, it is often a combination of change initiators and change resistors that creates the premature victory celebration. In their enthusiasm over a clear sign of progress, the initiators go overboard. They are then joined by resistors, who are quick to spot any opportunity to stop change. After the celebration is over, the resistors point to the victory as a sign that the war has been won and the troops should be sent home. Weary troops allow themselves to be convinced that they won. Once home, the foot soldiers are reluctant to climb back on the ships. Soon thereafter, change comes to a halt, and tradition creeps back in.
Instead of declaring victory, leaders of successful efforts use the credibility afforded by short-term wins to tackle even bigger problems. They go after systems and structures that are not consistent with the transformation vision and have not been confronted before. They pay great attention to who is promoted, who is hired, and how people are developed. They include new reengineering projects that are even bigger in scope than the initial ones. They understand that renewal efforts take not months but years. In fact, in one of the most successful transformations that I have ever seen, we quantified the amount of change that occurred each year over a seven-year period. On a scale of one (low) to ten (high), year one received a two, year two a four, year three a three, year four a seven, year five an eight, year six a four, and year seven a two. The peak came in year five, fully 36 months after the first set of visible wins.
Error 8: Not Anchoring Changes in the Corporation’s Culture
In the final analysis, change sticks when it becomes “the way we do things around here,” when it seeps into the bloodstream of the corporate body. Until new behaviors are rooted in social norms and shared values, they are subject to degradation as soon as the pressure for change is removed.
Two factors are particularly important in institutionalizing change in corporate culture. The first is a conscious attempt to show people how the new approaches, behaviors, and attitudes have helped improve performance. When people are left on their own to make the connections, they sometimes create very inaccurate links. For example, because results improved while charismatic Harry was boss, the troops link his mostly idiosyncratic style with those results instead of seeing how their own improved customer service and productivity were instrumental. Helping people see the right connections requires communication. Indeed, one company was relentless, and it paid off enormously. Time was spent at every major management meeting to discuss why performance was increasing. The company newspaper ran article after article showing how changes had boosted earnings.
The second factor is taking sufficient time to make sure that the next generation of top management really does personify the new approach. If the requirements for promotion don’t change, renewal rarely lasts. One bad succession decision at the top of an organization can undermine a decade of hard work. Poor succession decisions are possible when boards of directors are not an integral part of the renewal effort. In at least three instances I have seen, the champion for change was the retiring executive, and although his successor was not a resistor, he was not a change champion. Because the boards did not understand the transformations in any detail, they could not see that their choices were not good fits. The retiring executive in one case tried unsuccessfully to talk his board into a less seasoned candidate who better personified the transformation. In the other two cases, the CEOs did not resist the boards’ choices, because they felt the transformation could not be undone by their successors. They were wrong. Within two years, signs of renewal began to disappear at both companies.
* * *
There are still more mistakes that people make, but these eight are the big ones. I realize that in a short article everything is made to sound a bit too simplistic. In reality, even successful change efforts are messy and full of surprises. But just as a relatively simple vision is needed to guide people through a major change, so a vision of the change process can reduce the error rate. And fewer errors can spell the difference between success and failure.
Reprint R0701J; HBR OnPoint 1710
EIGHT STEPS TO TRANSFORMING YOUR ORGANIZATION
1. Establishing a Sense of Urgency
• Examining market and competitive realities
• Identifying and discussing crises, potential crises, or major opportunities
2. Forming a Powerful Guiding Coalition
• Assembling a group with enough power to lead the change effort
• Encouraging the group to work together as a team
3. Creating a Vision
• Creating a vision to help direct the change effort
• Developing strategies for achieving that vision
4. Communicating the Vision
• Using every vehicle possible to communicate the new vision and strategies
• Teaching new behaviors by the example of the guiding coalition
5. Empowering Others to Act on the Vision
• Getting rid of obstacles to change
• Changing systems or structures that seriously undermine the vision
• Encouraging risk taking and nontraditional ideas, activities, and actions
6. Planning for and Creating Short-Term Wins
• Planning for visible performance improvements
• Creating those improvements
• Recognizing and rewarding employees involved in the improvements
7. Consolidating Improvements and Producing Still More Change
• Using increased credibility to change systems, structures, and policies that don’t fit the vision
• Hiring, promoting, and developing employees who can implement the vision
• Reinvigorating the process with new projects, themes, and change agents
8. Institutionalizing New Approaches
• Articulating the connections between the new behaviors and corporate success
• Developing the means to ensure leadership development and succession
————————–?
PHOTO (COLOR)
~~~~~~~~
by John P. Kotter
Now retired, John P. Kotter was the Konosuke Matsushita Professor of Leadership at Harvard Business School in Boston.
________________________________________
Harvard Business Review Notice of Use Restrictions, May 2009Harvard Business Review and Harvard Business Publishing Newsletter content on EBSCOhost is licensed for the private individual use of authorized EBSCOhost users. It is not intended for use as assigned course material in academic institutions nor as corporate learning or training materials in businesses. Academic licensees may not use this content in electronic reserves, electronic course packs, persistent linking from syllabi or by any other means of incorporating the content into course resources. Business licensees may not host this content on learning management systems or use persistent linking or other means to incorporate the content into learning management systems. Harvard Business Publishing will be pleased to grant permission to make this content available through such means. For rates and permission, contact permissions@harvardbusiness.org.
Authors: Senge, Peter.
Source: Executive Excellence.
Jan1999, Vol. 16 Issue 1, p12. 2p. 1
Color Photograph, 1 Black and White Photograph. .
Document
Type: Article.
Subject Terms:*MANAGEMENT
*LEADERSHIP.
Abstract: Explains the corporate concept of creative tension. Orientation of primary institutions; How to resolve and generate creative tension..Full Text Word Count:1650.ISSN:8756-2308.Accession Number:
Creative Tension.
Leaders build organizations where people are continually expanding their capabilities to shape their futures.
WE ARE DESIGNED FOR learning. We come fully equipped with an insatiable drive to explore and experiment.
Unfortunately, the primary institutions of our society are oriented predominantly toward controlling rather than learning, rewarding individuals for performing for others rather than for cultivating their natural curiosity and impulse to learn. The young child entering school discovers quickly that the name of the game is getting the right answer and avoiding mistakes — a mandate no less compelling to the aspiring manager.
“Our prevailing system of management destroys people,” wrote W. Edwards Deming. “People are born with intrinsic motivation, self-esteem, dignity, curiosity to learn, joy in learning. The forces of destruction begin with toddlers — a prize for the best costume, grades, degrees, and gold stars. On the job, people, teams, and divisions are ranked — reward for the one at the top, punishment at the bottom. Quotas, incentive pay, and separate business plans cause further loss.”
Ironically, by focusing on performing for someone else’s approval, corporations create the very conditions that predestine them to mediocre performance.
Over the long run, superior performance depends on superior learning. The need for understanding how organizations learn and accelerating that learning is greater today than ever before. It is simply no longer possible for anyone to “figure it all out at the top.” The old model, “the top thinks and the local acts,” must now give way to integrating thinking and acting at all levels. While the challenge is great, so is the payoff. “The person who figures out how to harness the collective genius of the people in his or her organization,” according to former Citibank CEO Walter Wriston, “is going to blow the competition away.”
The Integrating Principle
Leadership in a learning organization starts with the principle of creative tension. Creative tension comes from seeing clearly where we want to be, our “vision,” and telling the truth about where we are, our “current reality.” The gap between the two generates a natural tension.
Creative tension can be resolved in two basic ways: by raising current reality toward the vision, or by lowering the vision toward current reality. Individuals, groups, and organizations who learn how to work with creative tension learn how to use the energy it generates to move reality more reliably toward their visions.
The principle of creative tension has long been recognized by leaders. Without vision there is no creative tension. Creative tension cannot be generated from current reality alone. Analysis alone will never generate a vision. Many who are otherwise qualified to lead, fail to do so because they try to substitute analysis for vision. They believe that, if only people understood current reality, they would surely feel the motivation to change. They are then disappointed to discover that people resist the changes that must be made to alter reality. The natural energy for changing reality comes from holding a picture of what might be that is more important to people than what is.
But creative tension cannot be generated from vision alone; it demands an accurate picture of current reality as well. Vision without an understanding of current reality will more likely foster cynicism than creativity. The principle of creative tension teaches that an accurate picture of current reality is just as important as a compelling picture of a desired future.
Leading through creative tension is different than solving problems. In problem solving, the energy for change comes from attempting to get away from an aspect of current reality that is undesirable. With creative tension, the energy for change comes from the vision, from what we want to create, juxtaposed with current reality. While the distinction may seem small, the consequences are not. Many people and organizations find themselves motivated to change only when their problems are bad enough to cause them to change. This works for a while, but the change process runs out of steam as soon as the problems driving the change become less pressing. With problem solving, the motivation for change is extrinsic. With creative tension, the motivation is intrinsic.
Reflection and Inquiry Skills
Many of the best ideas in organizations never get put into practice because new insights and initiatives conflict with established mental models. The leadership task of challenging assumptions without invoking defensiveness requires four reflection and inquiry skills:
1. See leaps of abstraction. Our minds literally move at lightning speed. Ironically, this often slows our learning, because we leap to generalizations so quickly that we never think to test them. We then confuse our generalizations with the observable data upon which they are based, treating the generalizations as if they were data.
2. Balance inquiry and advocacy. Most managers are skilled at articulating their views and presenting them persuasively. While important, advocacy skills can become counterproductive as managers rise in responsibility and confront increasingly complex issues that require collaborative learning among different, equally knowledgeable people. Leaders in learning organizations need to have both inquiry and advocacy skills. When advocating a view, they need to explain the reasoning and data that led to their views and encourage others either to test their views or to provide different views. And when inquiring into another’s views, they need to seek to understand the other’s views, rather than simply restate their own views.
3. Distinguish espoused theory from theory in use. We all like to think that we hold certain views, but often our actions reveal deeper views. For example, I may proclaim that people are trustworthy, but never lend friends money and jealously guard my possessions. Obviously, my deeper mental model (my theory in use) differs from my espoused theory. Recognizing gaps between espoused views and theories in use (which often require the help of others) can be pivotal to deeper learning.
4. Recognize and defuse defensive routines. As one CEO put it, “Nobody ever talks about an issue at the 8 a.m. business meeting exactly the same way they talk about it at home that evening or over drinks at night.” The reason is what Chris Argyris calls “defensive routines,” entrenched habits used to protect ourselves from the embarrassment and threat that come with exposing our thinking. For most of us, such defenses began to build early in life in response to pressures to have the right answers. Organizations add new levels of performance anxiety and thereby amplify and exacerbate this defensiveness. Those who are best at revealing and defusing defensive routines operate with a high degree of self-disclosure regarding their own defensiveness.
Systems Thinking Skills
Leaders should help people see the big picture. But how? In my experience, successful leaders often are “systems thinkers.” They focus less on day-to-day events and more on underlying trends and forces of change. But they often feel frustrated that others cannot see the world the way they do. Future leaders will need five skills:
1. See interrelationships, not things; processes (scenes), not snapshots. Most of us have been conditioned to focus on things and to see the world in static images. This leads us to linear explanations of systematic phenomenon.
2. Move beyond blame. We tend to blame each other or outside circumstances for our problems. But it is poorly designed systems, not incompetent or unmotivated individuals, that cause most problems. Systems thinking shows us that you and the cause of your problems are part of a single system.
3. Distinguish detail complexity from dynamic complexity. Some types of complexity are more important strategically than others. Detail complexity arises when cause and effect are distant in time and space, and when the consequences over time of interventions arc subtle and not obvious to many participants in the system. The leverage in most management situations lies in understanding dynamic complexity, not detail complexity.
4. Focus on areas of high leverage. Some have called systems thinking the “new dismal science” because it teaches that most obvious solutions don’t work — at best, they improve matters in the short run, only to make things worse in the long run. But there is another side to the story. Systems thinking also shows that small, well-focused actions can produce significant, enduring improvements, if they are in the right place. Systems thinkers refer to this idea as the principle of “leverage.” Tackling a difficult problem is often a matter of seeing where the high leverage lies, where a change — with a minimum of effort — would lead to lasting, significant improvement.
5. Avoid symptomatic solutions. The pressures to intervene in management systems that are going awry can be overwhelming. Unfortunately, given the linear thinking that predominates in most organizations, interventions usually focus on symptomatic fixes, not underlying causes. This results in only temporary relief, and it tends to create still more pressures later on for further, low-leverage intervention. If leaders acquiesce to these pressures, they can be sucked into an endless spiral of increasing intervention. Sometimes the most difficult leadership acts are to refrain from intervening through popular fixes and to keep the pressure on everyone to identify more enduring solutions. While leaders who can articulate systematic explanations are rare, those who can will leave their stamp on an organization.
Many charismatic leaders manage almost exclusively at the level of events. They deal in visions and in crisis, and a little in between. Under their leadership, an organization hurtles from crisis to crisis. Eventually, people become reactive, burned out, and cynical. People have no control over their time, let alone their destiny.
In a learning organization, leaders are designers, teachers, and stewards. These roles require new skills: the ability to build shared vision, to challenge prevailing mental models, and to foster more systematic patterns of thinking.
Without vision there is no creative tension.
PHOTO (BLACK & WHITE):
PHOTO (COLOR):
~~~~~~~~
By Peter Senge, Peter Senge is chairman of Society of Organizational Learning and a senior lecturer fit MIT’s Sloan School of Management. He is the author of The Fifth Discipline, 617-253-1572.
________________________________________
Copyright of Executive Excellence is the property of HR.com, Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder’s express written permission. However, users may print, download, or email articles for individual use.
SAMPLE ANSWER
Fostering change
Steps to foster change process
Change is inevitable in any organization. However, it is as well difficulty to trigger change in organization, as it requires application of specific techniques. Not many people will embrace change that easy (Kotter, 2007). To foster change in my organization, I will do in-depth research to establish whether it is indeed necessary to embrace change. This will help to identify whether the change will be of benefit to the organization or not or whether, the other stakeholders will accept it or not. I will as well incorporate the views and opinions of other stakeholders. Stakeholders will have to deliberate on the change idea and provide their own recommendation. Communication is also very important when implementing change (Kotter, 2007). All the parties that the change is going to affect will be informed progressively about the change and its benefits. This will help to reduce the level of resistance. Some of challenges that should be expected is increased resistance from the stakeholders, poor communication techniques, insufficient resources to implement the change and inadequate personnel with adequate skills to ensure proper implementation of the change. However, these changes can be managed by recruiting additional staffs that have requisite skills to implement the changes, adopting effective communication media, convincing/persuading the stakeholders on the benefits of the changes and soliciting funds and other resources through credit facilities.
Comparison and contrast of steps to take to foster change process in my own community to impact public health.
To foster change in my own community I will first engage with the community leaders to share this idea with them. Afterwards, I will communicate the vision to the rest of the community members and receive their response. I will then act on their feedback and persuade them about the need to embrace the change. This will require that I demonstrate good leadership skills that they should not worry about the project. These steps are not consistent with the previous steps as there is no in-depth research conducted. The steps are appropriate because they will help to motivate and persuade the community to accept the changes with minimal or no resistance. One challenge likely to be encountered is resistance by some section of the community. To counter this, I will bring experts and opinion leaders that will demonstrate to them that the changes have worked elsewhere and therefore they should embrace the same for their own benefit (Senge, 1990)
References
Kotter, J. P. (2007). Leading change. Harvard Business Review, 85(1), 96-103.
Senge, P. M. (1990). The leader’s new work: Building learning organizations. Sloan Management Review, 32(1), 7-23.
We can write this or a similar paper for you! Simply fill the order form!
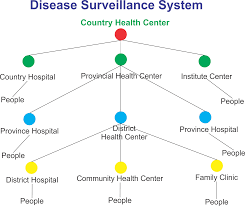
Effectiveness and efficiency of the disease surveillance system
How to evaluate the effectiveness and efficiency of the disease surveillance system
Order Instructions:
Evaluating Automated Surveillance Systems for Tuberculosis.
System Evaluation Proposal (New) for tuberculosis
Research and identify two or three additional peer-reviewed articles related to evaluating disease surveillance systems.
Write a 2- to 3-page paper in which you:
Propose how you would evaluate the effectiveness and efficiency of the disease surveillance system you have developed throughout the course.
Identify and define the criteria you will include in your evaluation.
Justify the selection of evaluation criteria.
Cite the two or three articles that informed your research for this section.
System Analysis (New)
Write a 2- to 3-page paper in which you analyze the cost, functionality, timeframe, and social, political, environmental, and economic elements of your surveillance system.
Conclusion (New)
Write a 1- to 2-page summary of your Project including a review of the purpose and goals of the Project, salient research findings, system features, analysis, implications, and limitations.
References (New)
Write a bibliography of research and Project resources compiled in APA format.
SAMPLE ANSWER
How to evaluate the effectiveness and efficiency of the disease surveillance system
The adoption of Automated Surveillance System in the tuberculosis treatment aims at helping health professionals assess the tuberculosis prevalence, initiate reliable intervention measures, and examine the epidemiology of the health complication. Therefore, the adoption of effective and reliable measures for evaluating the efficiency of the surveillance system will be relatively essential in reducing the regrettable effect of tuberculosis infection on patients and the entire society. The core aim of introducing Automated Surveillance Systems in the treatment of tuberculosis is to enhance confidentiality, timeliness, and accuracy. As a result, in order to evaluate the effectiveness of the Automated Surveillance Systems in the treatment and prevention of tuberculosis, scholars and healthcare professionals need to assess the accuracy of the system. Researchers will rely on the available medical information in assessing whether information given by patients are similar to the one presented in the system. Conducting interview among health professionals and the infected victims will be essential in examining the effectiveness of the system. Additionally, health professionals will be interested in evaluating the time taken in retrieving critical medical data. Timely retrieval of patients’ data will be an indication that the system is effective in supporting the prevention of tuberculosis in the modern society.
Furthermore, the Automated Surveillance Systems must have the ability of helping health professionals abide by the set ethical guidelines. Consequently, with the intention of evaluating the effectiveness and efficiency of the system, health professionals will focus at assessing whether the Automated Surveillance Systems hold the confidentiality principle. The system ability to comply with the existing confidential ethical guideline will be critical in examining the effectiveness of the modern technology in addressing tuberculosis challenges in the modern society (Thacker, Choi, & Brachman, 2009)
The assessment of the Automated Surveillance Systems ability to prevent and control the occurrence of tuberculosis in the future will be significant in influencing the efficiency of the system. Ideally, the main aim of introducing Automated Surveillance Systems in the treatment of tuberculosis is to help in the collection of accurate data essential in formulating reliable intervention measures. Furthermore, the adoption of Automated Surveillance Systems aim at assessing the impacts of the existing intervention programs in the treatment of tuberculosis. Therefore, the evaluation initiative will aim at examining whether the system has the ability of providing accurate data that could assist in the reduction of tuberculosis infection in the future. Successful Automated Surveillance Systems should also have the ability of providing reliable information that could assist in modifying educational and other critical risk-reduction initiatives and programs. Therefore, the evaluation of the applicability of the Automated Surveillance Systems in modern education sector will be essential in determining the effectiveness of system in the modern health sector (Hripcsak, Knirsch,Jain, Stazesky, Pablos-Mendez & Fulmer, 2009).
The evaluation of the Automated Surveillance Systems in the treatment of tuberculosis should also seek to examine the system’s ability to examine the long-term trend and the pattern of the disease. Precisely, the introduction of modern technology aims at easing the process of assessing the trend of the health problems. Effective assessment of the secular trend of any healthcare challenges helps in the adoption of reliable and effective plans for dealing with the health problem. Besides, the knowledge on the pattern of spread of tuberculosis will help health professionals set aside the necessary resources for dealing with the problem. Therefore, an effective Automated Surveillance Systems should provide data essential in predicting the pattern of the disease and the most effective intervention measures of dealing with the challenge (Yokoe, Subramanyan, Nardell, Sharnprapai, McCray & Platt, 1999).
Analysing critical elements in surveillance system
The proposed Automated Surveillance Systems will largely reduce the cost of treating and preventing tuberculosis. Although the cost of implementing the process may be relatively high, the outcomes of the project largely supersede the entire implementation cost. For instance, effective adoption of Automated Surveillance Systems will reduce the cost incurred in storing critical health record. The technology will equally be useful in minimising the cost of undertaking critical health researches. The timeframe for adopting Automated Surveillance Systems in the tuberculosis intervention measures is relatively limited compared to the other conventional intervention measures. The policy implementers will require roughly three to six months installing all the necessary machineries, software, and hardware. The project is also likely to reduce the time required in collecting and storing critical health records. Modern technology especially in healthcare sector aim at reducing the time required in retrieving critical health information.
Regarding the functionality of the project, Automated Surveillance Systems aim at integrating all stakeholders in the treatment of tuberculosis. The technology will offers an avenue where all stakeholders including family members and patients will share critical information on the most effective and applicable means of dealing with tuberculosis infections (Aryel, 2004). The technology will also be significant in enhancing the storage of critical information essential in supporting the spread of the disease. The project implementers will also have the mandate of ensuring that the technology fits with other equipment in the healthcare system. Based on the available data, effective application of Automated Surveillance Systems should address threatening social and ethical issues in the society. The technology ensures that health professionals uphold clients’ confidentiality and privacy. Besides, the initiative is critical in reducing social challenges that emerge due to the spread of tuberculosis infections in the society. Studies indicate that tuberculosis is among the leading killers diseases in developing and poor states. Therefore, the Automated Surveillance Systems will be vital in addressing social challenges that emerge due to high tuberculosis prevalence rate.
Automated Surveillance Systems will also be a critical tool in influencing making political decisions in the treatment and prevention of tuberculosis. For instance, political leaders will rely on the Automated Surveillance Systems data in making critical policies and regulations to prevent tuberculosis in the society. Equally, Automated Surveillance Systems will serve a critical role in facilitating the adoption of well-informed decisions on critical health issues. Automated Surveillance Systems will play a noticeable role in determining environmental factors that led to the spread of tuberculosis. The technology will also help in the classification of areas and regions that are prone to tuberculosis infections. The identification of environmental factors that could lead to increased spread of tuberculosis will be paramount in enhancing the adoption of reliable policies and intervention measures to deal with the problem. Studies further indicate that the modern technology has been playing a central role in addressing economic challenges (Wagner, Tsui, Espino, Dato, Sitting, Caruana & Fridsma, 2001). For instance, effective implementation of Automated Surveillance Systems in the prevention and treatment of tuberculosis will be significant in addressing financial challenges in modern healthcare system. The project will also be helpful in minimising the cost incurred in the treatment of tuberculosis. Additionally, the project will reduce research and development costs. Therefore, based on the presented data, the adoption of Automated Surveillance Systems in the treatment of tuberculosis will holistically address all issues and elements that hinder the success of the current intervention measures
Conclusion
The core aim of adopting the Automated Surveillance Systems in the treatment of tuberculosis is to understand and learn the pattern of the diseases occurrence. The system data will also be essential in facilitating the adoption of reliable and effective intervention and treatment measures. The project is also essential in enhancing the investigation, control, and prevention of tuberculosis. The available research data further indicate that an effective application of Automated Surveillance Systems will be essential in increasing effectiveness in the treatment of tuberculosis. Furthermore, Automated Surveillance Systems is vital in addressing various environmental, economic, social, and political elements that hinder the success of the conventional intervention measures.
In addition, some of the Automated Surveillance Systems features include storage and analysis software, data retrieval software, ability to detect future health changes, ability to identify host and agent factors, and the ability of identifying sudden changes and transformation in disease distribution and occurrences. The researchers will rely on modern software in analysing the effectiveness of Automated Surveillance Systems in the treatment of tuberculosis. The study on the efficiency of the Automated Surveillance Systems will have an implication on the manner in which scholars adopt modern means in the treatment of regrettable health challenges. In addition, modern scholars will have the ability and opportunity of applying modern technology in the collection of researches data. Although the project aims at improving the nature of services in modern health centres, it may witness some regrettable limitations that include limited resources and time, resistance, ethical challenges and legal issues.
References
Aryel, R. M. (2004). Public Health Surveillance: The Role of Clinical Information Systems. In Healthcare Information Management Systems (pp. 513-531). New York, NY: Springer New York
Hripcsak, G., Knirsch, C. A., Jain, N. L., Stazesky Jr, R. C., Pablos-Mendez, A., & Fulmer, T. (2009). A health information network for managing innercity tuberculosis: bridging clinical care, public health, and home care. Computers and Biomedical Research, 32(1), 67-76.
Wagner, M. M., Tsui, F. C., Espino, J. U., Dato, V. M., Sitting, D. F., Caruana, R. A., & Fridsma, D. B. (2001). The emerging science of very early detection of disease outbreaks. Journal of Public Health Management and Practice, 7(6), 51-59.
Yokoe, D. S., Subramanyan, G. S., Nardell, E., Sharnprapai, S., McCray, E., & Platt, R. (1999). Supplementing tuberculosis surveillance with automated data from health maintenance organizations. Emerging infectious diseases, 5(6), 779.
We can write this or a similar paper for you! Simply fill the order form!
Improving Disease Surveillance in Developing Countries
Improving Disease Surveillance in Developing Countries
Order Instructions:
Improving Disease Surveillance in Developing Countries
The dearth of disease surveillance in developing nations is an immediate opportunity for public health professionals to improve the health of underserved populations. As presented in Chapter 9 of your course text, implementing disease surveillance in developing nations requires that public health professionals acclimate to the variety of unique obstacles in each country. From insufficient lab diagnostics to a lack of personnel with necessary professional skills, there are many potential challenges to establishing surveillance systems in developing nations.
To prepare for this Application Assignment, review your Learning Resources. Go to the World Health Organization (WHO) website and identify conditions or diseases that occur in developing countries where the establishment of disease surveillance systems would help to prevent or mitigate the spread of disease (e.g., hospital-acquired infections, food- and water-borne diseases, tuberculosis, cervical cancer, etc.). Select a country and a corresponding disease or condition that you believe would be greatly impacted by the implementation of a disease surveillance system. Research the literature pertaining to the surveillance system in your chosen country and condition.
To complete this Application Assignment, write a 3- to 4-page paper that provides an overview of your selected country and condition or disease.
Be sure to address the following:
Describe the condition/disease and the developing country.
Describe the current monitoring procedures used in the developing country.
Provide a rationale as to why the country would greatly benefit from a disease surveillance system.
Describe two additional special features that should be a part of surveillance systems in your chosen country.
Describe challenges public health officials face in establishing disease surveillance systems in this country.
Describe how you would address these challenges.
SAMPLE ANSWER
Malaria and Condition in Kenya
Malaria is a major health concern in the Sub-Saharan region of Africa. Prevalence of this disease in the region calls for effort to ensure proper surveillance and management of the disease in the region. Kenya is one of the countries within the Sub-Sahara region where malaria is preponderant and needs improved surveillance. According to World Health Organization (WHO), about 90% of all global malaria deaths occur in the Sub-Sahara Africa where Kenya is part of. Further, about 627,000 deaths recorded each year around the globe are due to malaria. This implies that about 564,000 deaths resulting from malaria are recorded within the Sub-Sahara Africa each year. This makes malaria a leading killer in the region and disease surveillance of the disease in the region is warranted and urgent (Yukich et al., 2012).
In terms of costs one of the challenges of malaria is the cost of management. On the other hand, the number of deaths as a result of malaria fever has reduced but there is still a lot to be done since in 2013 alone there were 30,000 deaths attributed to malaria fever. According to KEMRI (Kenya Medical Research Institute) malaria fever is the leading cause of death in Kenya, accounting for between 30% and 50% outpatient attendance in health care facilities. Moreover, malaria fever accounts for 20% of the total number of admissions to hospitals and healthcare facilities.
Current Monitoring Procedures
Malaria surveillance and reporting in Kenya is achieved through utilization of a number of reporting systems. These reporting systems comprise of District Health Information Systems (DHIS), Integrated Disease Surveillance and Response (IDSR), Logistics Management Information System (LMIS), and Laboratory Information Management System (LIMS). Surveillance data derived from these systems are conveyed at diverse intervals with broad variations across the systems.
In order for the malaria surveillance and reporting system to work, it needs to provide reports about rapid diagnostic kit (RDT), timely report of malaria drug stocks, the number of outpatients coming to the health facility, the number of patients tested for malaria, the number that tests positive for malaria and the number of patients treated with anti-malaria (Bastiaens et al., 2011).
Rationale for the SMS-Based Malaria Surveillance System for Kenya
The proposed Short-Message Based (SMS-Based) malaria surveillance is philosophically sound based on its ability to solve the problems and difficulties presented by the existing surveillance systems. Firstly, the existing malaria surveillance and reporting system is delayed and inaccurate. Secondly, the delay and inaccuracy that accompany it lead to characteristically low approximations of malaria incidence from custom surveillance data. Therefore, effective surveillance procedures to gather, accumulate and handle information from communities to national levels in a timely fashion are urgently desired to monitor realization of the new case-management guidelines (Githinji et al., 2014). Kenya, just like most developing countries, has seen rapid increase in mobile phone connections and this boosts the potential of utilizing mobile phone text messages in collection of data from the field. This is because it makes it possible for immediate communication besides providing an added advantage of ease of use. Mobile telephony in field data collection also reduces data transmission delays hence solves a big problem that that faces the existing surveillance strategy.
Additional Special Features for Malaria Surveillance in Kenya
Technology integration especially short-message platforms can immensely help in disseminating information from health care facilities. Mobile phone platform will be an essential feature of the surveillance system. This feature will enable data from the rural and sub-county regions to be sent to the national malaria surveillance centers through short messages.
Health worker training will be another feature that will encompass proper understanding utilization of the system and reporting of the data. This training will involve how to access and extract the relevant surveillance data. The training will further have an objective geared toward achieving the “T3: Test-Treat-Track” of the WHO launched in 2010 (WHO 2012).
Challenges in Establishing Malaria Surveillance in Kenya
Insufficient supply of diagnostic equipment in health facilities besides poor knowledge about malaria are among the most evident challenges that public health officials who handle malaria management encounter. In addition, there has been reluctance in the way the public takes preventive measures against malaria. Such preventive measures include sleeping under nets treated with necessary insecticide. Another challenge is that while taking anti-malarial drugs is important for management of the disease, many pregnant women do not take anti-malarial drugs (Mphatswe et al 2012). Investment in malaria has also seen a steady decline and this has limited the extent to which the management and surveillance can be achieved given that resources needed to handle the endemic are limited.
Solution for the Challenges
The surveillance system will be designed to specifically address the imprecision in timing of the existing system. As such, SMS system will be made to contemporaneously report malaria incidence on a weekly basis. Accuracy will also make an integral part of the system, where medical practitioners will be trained on the proper use and reporting of the system.
References
Bastiaens G. J, Schaftenaar E, Ndaro A, Keuter M, Bousema T, Shekalaghe S. A (2011): Malaria diagnostic testing and treatment practices in three different Plasmodium falciparum transmission settings in Tanzania: before and after a government policy change. Malaria Journal, 10:76
Mphatswe W, Mate K. S., Bennett B, Ngidi H, Reddy J, Barker P. M, & Rollins N (2012): Improving public health information: a data quality intervention in KwaZulu-Natal, South Africa. Bull World Health Organ, 90:176-182.
Githinji, S., Kigen, S., Memusi, D., Nyandigisi, A., Wamari, A., Muturi, A., Jagoe, G., Ziegler, R., Snow, R., W. & Zurovac, D (2014) Using mobile phone text messaging for malaria surveillance in rural Kenya. Malaria Journal 13:107
Yukich J. O, Bennett A, Albertini A, Incardona S, Moonga H, Chisha Z, Hamainza B, Miller JM, Keating J, Eisele TP, Bell D (2012): Reductions in artemisinin-based combination therapy consumption after the nationwide scale up of routine malaria rapid diagnostic testing in Zambia. American Journal of Tropical Medical Hygiene, 87:437-446
We can write this or a similar paper for you! Simply fill the order form!
Which social determinants of health will the Hispanic community volunteers identify in their community leading to overweight and eventually obesity?
Will photo-voice data analysis help to elucidate ways to motivate the community to healthy collective action and social change to modify behavior and reduce health risks, therefore reducing health disparities in Hispanic communities?
Following Seminar 1 write your current research question.
B.
Research Methodology
The research will employ both qualitative and quantitative methodologies. This choice of methodology is based on the desire to gain trend insights and the human touch. In the findings the qualitative data will assist in understanding the patterns of quantitative analysis
What methodology would you propose to test your research question and why this is the best one?
C.
Theoretical Foundation and/or Conceptual Framework
The study will be guided by conceptual theories that will make it easier to understand, dynamics, interpret and forecast development and outcomes within the Hispanic community. To best address the questions, the study will use both the Social Learning Theory (SLT) and the Community Based Participatory Research (CBPR). The SLT will allow for focus on the following learning and modeling behavior – Reproduction, Attention, Motivation and Reproduction. On its part, the CBPR will allow the study to be sensitive and to connect attitudes and behavior. The behavior will be based on and guided by behavioral, normative and control beliefs.
D.
Gaps
The study will seek to offer communities an opportunity to record and reflect of their concerns. This should empower them in addition to offering better research data.
Identify at least 1 potential gap
E.
Assumptions, Limitations, and Delimitations
The study assumes that the Hispanic community has a problem with weight and obesity. The study will be limited to the Hispanic community only and delimited by taking into account the outside factors that affect the target population.
Identify at least 1 assumption, limitation, and delimitation.
F.
Controlling and Managing Bias
To control and manage bias, the research will employ a strategy that minimizes or eliminates the external influences on the subjects, researchers and methodologies.
Identify one strategy for controlling and managing bias in your research.
G.
Summary of the Literature/Logical Fallacies
The study will seek to understand the individual and by extension community motivators in seeking out healthy collective action and social change. It will additionally seek literature that explains the motivators that reduce health risks and by extension health disparities in the Hispanic communities.
The one logical fallacy that this study will work steadfastly to avoid is that of hasty generalizations. This entails making assumptions about a whole group based on sample that is inadequate. This is especially alive in this study that seeks the social determinants of health leading to overweight and eventually obesity.
Attach a brief outline that describes the flow of your intended literature review. Describe one logical fallacy and how you will guard against this in your own writing.
H.
Synthesis of the Literature
The centers of Disease Control and Prevention (CDC) points out that of the people who identify themselves as Hispanics, a significant majority were overweight and on their way to obesity. The Whatcom county Community health Assessment report does state that efforts to improve the social determinants of health have potential to positively impact many health outcomes for individual and families.
Write 1 paragraph that provides a synthesis of at least 3 articles that approach your topic from different perspectives.
I.
Implications for Future Research
This study seeks to offer a window in to the Hispanic community and their motivation in keeping a healthy societal outlook. In the future, the study should make it possible to better understand the individual factors and who they individually and collectively affect the health of Hispanics and by extension the world.
What implications will your study have on future research?
J.
Contributions to Discipline and to Social Change
The study will contribute to societal change by highlighting the factors that are social in affecting the health of a community. It is expected that the study will contribute to social change by motivating individuals and by extension the society to work their weight issues. When this is achieved, the society will have overcome the challenge of obesity within it. Finally, the study will offer insights into the Hispanic culture that must adjust to allow for the attainment of the desired health results leading to reductions and eventual elimination of obesity.
What contributions will your research make to the discipline and society?
Note: Social change implications are expressed in terms of tangible improvements to individuals, communities, organizations, institutions, cultures, or societies.
As in any field, employees in public health tend to be more productive and satisfied in their work when they are part of a strong, supportive team. How do leaders help to bring about such a team?
This week you learned about several strategies for building teams that meet the needs of the organization and of the team members. These strategies include the use of the Behavioral Event Interview (BEI) when hiring, as well as the STAR method, which can be helpful in many contexts including an interview. As a reminder, “STAR” stands for:
ANSWER THE FOLLOWING QUESTIONS:
1.Situation: give an example of a situation you were involved in that resulted in a positive outcome
2.Task: describe the tasks involved in that situation
3.Action: talk about the various actions involved in the situation’s task
4.Results: what results directly followed because of your actions
USE THE FOLLOWING ARTICLES ONLY (DO NOT DEVIATE FROM ARTICLES)
1. Fernandez, C. (2007). Employee engagement. Journal of Public Health Management & Practice, 13(5), 524-526.
2. Fernandez, C. (2006). The behavioral event interview: Avoiding interviewing pitfalls when hiring. Journal of Public Health Management & Practice, 12(6), 590-593.
Please apply the Application Assignment Rubric when writing the Paper.
I. Paper should demonstrate an excellent understanding of all of the concepts and key points presented in the texts.
II. Paper provides significant detail including multiple relevant examples, evidence from the readings and other sources, and discerning ideas.
III. Paper should be well organized, uses scholarly tone, follows APA style, uses original writing and proper paraphrasing, contains very few or no writing and/or spelling errors, and is fully consistent with doctoral level writing style.
IV. Paper should be mostly consistent with doctoral level writing style.
For this Discussion, consider the steps you could take as a leader to build a strong team. What would you do to hire your replacement in your current job (if you work in the public health area) or to fill a public health position you hope to hold in the near future? How might you use the BEI and STAR method to help you in this hiring/interviewing process?
SAMPLE ANSWER
Employees tend to be more productive and satisfied with their work when they are part of a strong, supportive team with the help of a strong team leader. Leaders significantly influence building a strong team through application of strategies that build teams that meet organizational and team member’s needs. Fernandez (2006) argues that building a strong team is a challenging task for managers. Team selection and team building are the predictors of future derailment, while hiring the wrong employees is a common experience limiting building a strong team. As a leader, one can build a strong team through hiring the right people for the job roles. The right people should not only have technical skills to qualify as strong team members but should also possess knowledge on the job tasks to be given as well as have soft skills. Soft skills are vital for work dynamics and ultimately govern innovation, productivity and the team’s agility. Leaders can build strong teams through choosing members who have diverse backgrounds to bring a range of skills to the organization. Leaders should look for committed members who are willing to see the vision of the organization come to yield. They will guide the organization towards attaining its vision and mission. A leader should guide the team and be enthusiastic for his role to impact the team positively.
The public health sector is highly dynamic requiring strong teams to perform tasks effectively. To get the right team for public health, it is crucial to hire the right employees for the right job roles. The process of hiring and replacing employees in the public health sector, can be done through strategies like interviewing the candidates before hiring them. According to Fernandez (2006), the interview is an imperative part of letting the team manager about a candidates qualifications, attributes, competencies and traits and how consequently deciding on which candidate best suits the job vacancy. The old style of interview is typically plagued by spending time telling employees about the organization rather than the organization learning about the prospective candidates.
The BEI and STAR method can be useful for the hiring and interviewing processes. BEI is a strategy of interviewing that demonstrates efficacy based on a prospective candidates actual experience. It starts by examining the job description closely to pull out critical areas that determine the success of the candidate. This technique also has open-ended questions to examine the candidates accomplished tasks. BEI is a suitable method that can be applied to public health to list critical areas of job performance like conducting preventive medicine or disaster response programs followed by application of the epidemiological method to identify factors increasing mortality. The next step can include questions relevant to the candidate’s actual behavior like specific experience in emergency response initiatives like responding to the Ebola outbreak.
The third step can include a STAR method that represents situation, task, action and result. It guides an interviewer to a successful interview through which they answer questions regarding a situation they were involved in resulting to a positive outcome, describing tasks involved in the situation, talking about various actions involves in the situation and the task and finally the results directly followed because of actions. Using BEI and SMART techniques for interviewing employees helps build a team that has highly predictable performance in terms of Interpersonal interactions. BEI specifically predicts the future behavior through examining the past performances that are critical for future performances of the organization. Both techniques are suitable for developing appropriate methods that build strong teams
SWOT analysis is a powerful tool that you can use in order to assess your strengths and weakness and to anticipate threats and opportunities. By cultivating such awareness, individuals can gain valuable information that they can act upon in order to take advantage of the multiple opportunities available to them and seek assistance to meet the challenges they face. This Personal Development Portfolio assignment asks you to analyze your own strengths and weaknesses and identify opportunities and threats in your environment.
•Based upon the Learning Resources and your experience, reflect on your strengths, weaknesses, opportunities and threats as they relate to your goals and career development.
• Create a document with four areas labelled as strengths, weaknesses, opportunities and threats. Using bullet points, fill in the document with your strengths, weaknesses, opportunities and threats as they relate to your goals and career development.
•Strengths and weaknesses are aspects of your knowledge, abilities, background and so forth. They are something you possess as a person and could potentially develop or improve upon.
•Opportunities and threats are external to you—in other words, aspects of your organisation, your industry or even the economic, social or political context in general.
•Include a brief (approximately 600 words) summary and reflection on your personal SWOT analysis.
Appreciate each single moment you spend in writing my paper
Best regards
SAMPLE ANSWER
Week 5 information: Tuberculosis disease surveillance system
TB disease surveillance system is essential in ensuring closer monitoring and management of the disease. The system must function appropriately to have tangible benefits to the users. Quality assurance is very critical part of any surveillance system that operates successful. Quality assurance ensures that the system is continuously monitored evaluated and data is improved.
In US, national tuberculosis Surveillance System (NTSS) is located at the division of tuberculosis Elimination (DTBE) and functions as the national repository of TB disease surveillance data. Center for Diseases control and prevention receive information/data from the various jurisdictions reports through a standardized data collection from known as RVCT) Report of Verified of Case OF Tuberculosis (Center for Disease Control and Prevention (CDC), 2014).
The RVCT is usually revised on period basis to take into consideration the new changes in the disease epidemiology. The latest implementation was done in the year 2009 and it incorporated more recent development such as web-based systems. There is still a lot that have been done to ensure that data is collected and reported well to ensure that adequate information is available. Various teams form partnerships with public health officials and other local professionals to develop and in launching of national training programs on the new RVCT (WHO, 2014). These initiatives are undertake to foster or enhance quality of data collected. In management of TB, it is critical to have enough data or information about the prevalence of the diseases. This information on the areas the disease is prevalence as well helps to come up with appropriate strategies to manage the disease.
Five factors require consideration to ensure quality assurance of the tuberculosis surveillance systems. These components includes, case detection, data accuracy, data completeness, data timeliness and data security and confidentiality (Center for Disease Control and Prevention (CDC), 2014). Case detection is the first aspect. Once an instance of specific diseases or even exposure such as TB is done, a health care worker reports it. This information as well is collected from laboratory work or from a medical or a vetenary care. The observation or such incidence should be diagnosed and verified.
Data accuracy is another important component of quality assurance. The submitted data need to match with the patient record at the location or point of care (Arkansas Department of Health, 2014). The data recorded in the surveillance system need to remain consistent with the activities that happened in the clinical encounter if they were not clinically appropriate or if they were clinically appropriate.
The third component is data completeness. This measure helps to ascertain whether information submitted has complete set of data items or not (Center for Disease Control and Prevention (CDC), 2014). This is very important as it ensures that any information stored in the system is complete and therefore can be relied in the future. This requires verification of such information to ensure that it is complete and meets the threshold set for data completeness.
Data is also required to factor in the aspect of timeliness. It is important that prompt reporting of surveillance data is done to the health authorities. Once the information is accessed, it is very important that this information is reported immediately to provide an appropriate mechanisms responding to the same and instituting to preventive mechanism.
The last component is data security and confidentiality. Security of data entails measures in place geared at protecting data of public health and information systems from accessibility by unauthorized release (Center for Disease Control and Prevention (CDC), 2014). It also involves measures concerning information identification, loss of information and damage of the systems. Data confidentiality aims to protect personal information gathered by public health organizations. Personal information should not be released to third parties without the consent of the owner of the information or the patients.
Quality Assurance components of TB surveillance system
Center for Disease Control and Prevention. (CDC). (2014). Tuberculosis Information Management System (TIMS) Replacements. Retrieved from: http://www.cdc.gov/tb/programs/tims/NEDSS.
•Comparing the HR leadership competencies outlined in the CIPD Profession Map and the SHRM Competency Model
•Critically analysing how these perspectives on HR professional competencies relate to the strategic HR leader role
The following conditions must meet in the essay:
1) I want a typical and a quality answer which should have about 1100 words.
2) The answer must raise appropriate critical questions.
3) The answer must include examples from experience or the web with references from relevant examples from real companies.
4) Do include all your references, as per the Harvard Referencing System,
5) Please don’t use Wikipedia web site.
6) I need examples from peer reviewed articles or researches.
Appreciate each single moment you spend in writing my paper
Best regards
SAMPLE ANSWER
HRM.W4.collaboration.R
CIPD Profession Map addresses different Human Resource aspects (perspectives) through structured HR leadership competencies in the map. From these different HR perspectives, CIPD Map addresses most HR obligations at all stages in management. That is, it covers all levels and stages in organization leadership like entry stage, mid stage, senior stage, and finally executive stage (CIPD website). Specifically, CIPD proffession Map covers eight behaviors and ten professional sectors in HR leadership in the four leadership stages mentioned above.
Society for Human Resource Management (SHRM) Competency Model on the other hand addresses HR leadership competencies at different leadership levels and stages, just like CIPD Map. Therefore, it addresses the HR leadership at entry stage, mid stage, senior stage, and executive stage from nine competencies perspective (SHRM website). Similar to CIPD Map, SHRM competency model focuses on eight HR behaviors in addressing the leadership competencies. Different from CIPD Map, the technical competency in SHRM Model is explained as implicating the application of the other eight behavioral competencies in the model. Therefore, a more genuine comparison can be achieved on the leadership competencies addressed in both CIPD Map and SHRM Model specifically on Human resource management.
In comparing the two approaches, both address HR leadership in three perspectives. They both address leadership at professional perspectives, behaviors perspective and different HR stages (Ulrich 2013). For instance, CIPD Profession Map addresses professional in leadership from the HR knowledge perspective. Therefore, HR knowledge dictates what a leader knows and does in line of duty, a prospect also supported in the SHRM Model on HR expertise replicating a technical competency in the model. These knowledge perspectives are applicable in diverse HR occupations irrespective of location or region. In addition, HR knowledge applies to all organizations irrespective of their size or shape in the market, a concept which creates bases for all eight behaviors in HR leadership activities.
SHRM Competency Model addresses business acumen as the leadership potential to critically think and make appropriate decisions in time with respect to the business situation at hand. This behavior approach is addressed in the CIPD Profession Map as decisive thinker behavior (CIPD website). It portrays similar characters of HR leadership where specifically, entrepreneurial characters of making potential and critical decision apply in the leadership role.
Critical evaluation is another leadership behavior addressed in both HR approaches. SHRM Competency Model specifies the critical evaluation behavior as the bases for logical and creative decision making in an organization. This follows step by step initiatives observed in critical evaluation of a situation (Lussier & Hendon 2013). Therefore, the effectiveness and worthiness of a decision is determined in critical thinking in evaluation. This behavior is perceived as personality credibility in the CIPD professional map, which filters decisions through critical evaluation. Even though the behaviors are indicated differently, their application in HR leadership behavior asserts to criticality and creativity application in evaluations for decision making.
Both approaches also observe global effectiveness of HR leadership, in addition to cultural effectiveness (Ulrich 2013). These are addressed as outcomes of positive influence of the environment and the society with respect to public relations. From SHRM Model, the leadership effectiveness is first observed inside the organization before being externally effective. Therefore, HR leaders have to model their organization internally, if good public relation is to be realized. Even though CIPD Map places this concept behavior from the HR role, applying skills in leadership replicates enhanced effectiveness. Therefore, utilizing the influence skills in HR leadership leads to global effectiveness, as well as cultural effectiveness.
The next comparison from the two approaches relate to the leading, directing and planning of the activities and progress of an organization. This is the primary definition of leadership in HR, to lead and direct, thus HR leaders avoid centralism and internalization behaviors (Lussier & Hendon 2013). CIPD Map presents such leadership behaviors as being determined to deliver, in avoiding centralism. SHRM Model on the other hand presents navigation in leadership behavior as being goal focused, thus supporting determination to deliver.
Quality communication is an essential behavior in leadership characters (Garey 2011). SHRM Model views communication as the key to organizational competency, while CIPD Map characterized this leadership behavior as curious way of acquiring and sending information. This behavior presents the essence of searching to acquire the information needed even when it is unavailable. HR leaders are therefore determined to look for essential communication and implement it where possible within the organization. Consultation would therefore be effected through quality communication, thus presenting another HR leadership behavior (Armstrong & Taylor 2014). CIPD Map positions consultation as the courage expressed while challenging a concept or idea. Prior to SHRM Model, consultation enables a leader to build relationships, hence getting the best from the challenges.
Relationship management is another behavior expressed in SHRM Model as leadership ability to instill togetherness in organization performance. This brings about team work in performance, which is a character every HR leader strives to attain and maintain. In CIPD Map, the relationship character is observed as a collaborative behavior implying team work development as supported in SHRM Model. Therefore, Leadership competency in teamwork building is developed through collaborative measures for excellent performance.
In relation to maintaining all the behavioral characters discussed above, being a role model as a leadership characterizes strategies in development of organizational behavior. HR leader should practice being a role model to employees and staff, a character which grows in them for development of ethical practices in an organization (McCarter & Schreyer 2000). SHRM Model refers such unity in behaviors as development of ethical practices. In CIPD Map, such leadership behavior is addressed similarly as a role model behavior, which leads to development and maintenance of ethical practices.
In general, all the above HR competencies happen to be related to the actual HR roles in an organization (Garey 2011). For instance, the characters of leadership, motivation and even personal credibility are involved in upholding HR leadership. Therefore, leadership characters would avoid internalization and centralism as noted in the two approaches, SHRM competency model and CIPD professional Map. Also, HR leader should present role model characters for creation and maintenance of relationships, which would translate to team work and ethical practices in an organization (Becker & Huselid 2001). Additionally, quality communication would enhance flow of activities, while ensuring efficient and effective problem solving within an organization.
Notably, all the eight behaviors in HR leadership are addressed in SHRM competency model at similar interpretations noted in CIPD professional Map. Since the HR competencies addressed are related to HR roles, their application would lead to professional HR performance. Moreover, the two models address HR leadership behavior at the four basic stages of HR leadership which are, entry stage, mid stage, senior stage, and the final stage. Therefore, HR leadership can be guided by the two models with respect to leadership roles applicable, irrespective of leadership level or stage (Armstrong & Taylor 2014).
References
Armstrong, M & Taylor, S 2014, Armstrong’s Handbook of Human Resource Management Practice (13th ed.), London: Kogan Page
Becker, B & Huselid, M 2001, The HR scorecard: Linking people, strategy, and performance, Boston, MA: Harvard Business School Press.
Describe the aggregate record of data that you will use.
Explain how you will ensure the quality of the data collected
SAMPLE ANSWER
Question
In many studies, data collected is used to provide insights about the areas of study. Assumptions are made through analysis of the data collected on various aspects. Aggregate data is therefore collection or related items that help the researcher or an individual to make some inferences (Greek interview, 2014). The aggregate record of data that I will use is about the products that tops in terms of sales for a particular employee in an organization. I will have to query several tables so that I can have information that will help me to make informed decision pertaining to the future operations and the strategies to adopt.
Quality of collected data should be safeguarded, as this will help to make correct assumptions. Enhancing quality of this data will be achieved throughout the process of data retrieving, application and after use. The information must be verified when it is input in the computer system to ensure that it is the correct information. Any mistake that may be made during this stage will affect the quality of data. The right software must be used to make this analysis to guarantee quality of data. The data should as well be free from any interference from third parties. The information must be well kept in safer locations and any data in the software must have a password that will deter people with malice from gaining access to the same. Furthermore, I will ensure quality of this data by using query function to examine information in various tables to help me to reflect properties of many groups of rows to ascertain whether indeed the date reflects the situation at hand (Greekinterview, 2014).
The data collocated must be well preserved and stored in safer locations to avoid any form of interference
Conflicting statistics exist related to women offenders. The number of women in the prison system, on parole, and on probation has increased steadily since the 1990s (Glaze, 2010). According to the Federal Bureau of Investigation (2010), however, women comprised only about 25% of all arrests in the United States in 2010 and are only 18% of the total correctional population. The latter might be due to the fact that women are less likely to commit violent offences that result in correctional sentences. But why do women comprise only 18% of the correctional population when 25% of all arrests are women? This leads to questions related to differential treatment between women and men offenders in the criminal justice system at the law enforcement, court, and/or correctional levels.
For this Assignment, you think about types of crimes that women offenders are more likely to commit. Also, you consider the treatment of women compared to men in the criminal justice system.
The Assignment (3 pages):
• Briefly describe two types of crimes that are more likely to be committed by women than men. Reference the FBI web resource listed in this week’s Learning Resources.
• Explain possible reasons each type of crime is more likely to be committed by women than men.
• Explain how women offenders may be treated differently than men offenders in the criminal justice system at the law enforcement, court, and/or correctional level(s).
• For your two examples, explain possible reasons for the differential treatment.
• Article: Flemke, K. (2009). Triggering rage: Unresolved trauma in women’s lives. Contemporary Family Therapy: An International Journal, 31(2), 123–139.
• Article: National Criminal Justice Reference Service. (2011). Women & girls in the criminal justice system—Facts and figures. Retrieved from http://www.ncjrs.gov/spotlight/wgcjs/facts.html
• Article: Spjeldenes, S., & Goodkind, S. (2009). Gender differences and offender reentry: A review of the literature. Journal of Offender Rehabilitation, 48(4), 314–335.
SAMPLE ANSWER
NCJRS (2012) reported that of the estimated 12,196,959 arrests made that year, 26.2% were female arrests. The office of the juvenile also reported female arrests as having accounted for 28% of the total arrests in 2010. The bureau of justice statistics revealed results of midyear jail inmates in 2013 as 10.9% being female inmates while male inmates were 4.2%. Justice statistics provided accounts of annual probation survey and parole from the total persons supervised in 2012 Jan –Dec stated that 24% of all adults on probation that year were females and 11% of all adults on parole were women with 19% of women on supervision in 2010 (NCJRS, 2012). These percentages clearly reveal that women offenders are increasing leading to more arrests, probation, and supervision in correctional centers.
Two types of crimes likely to be committed by women
Two of the most common crimes that women commit are prostitution and child/infant homicide. While prostitution is recognized as an old crime globally, it is reported to be the only crime that overtakes crimes committed by males in the criminal justice system. Women have fewer rates of arrest for virtually all crimes. Unlike men and women are quick to learn and correct their wrongs avoiding breaking the law at all costs. Child or infant homicide is another crime that women are likely to commit than men with infant homicide happening a few days after the birth of a child. Female arrests for prostitution crime category have been on high accounting for 30-40% of all arrests made on women (FBI, 2010). Infant homicide rates increased from 4.3 per 100000 in the 70’s to 9.2 per 100000 in 2000 (Child trends, 2014). Half of all infant homicides occur before the first trimester after birth.
Possible reasons for likelihood to be committed by women
Prostitution and infant homicide are most likely to be carried out by women for various reasons. Women indulge in prostitution as a source of income to fend for themselves and their children. With tough economic times, no employment opportunities and chances to get wealthy men who are willing to give them money for a little fun, women go for prostitution. While not all jobless women resort to prostitution as a means of getting their income, many countries shun prostitution as a vice and a moral wrong. Prostitution lowers the dignity of human worth limiting people to selling their dignity for money. States attempt to deal with morality and uphold virtues by arresting prostitutes. Infant homicide is a crime that has been reported amongst new mothers and women (Child trends data bank, 2014). Newborn children suffer the greatest risks of infant homicide as they are under the care of their mothers all the time. Infants depend on their mothers for nursing, feeding and totally everything. After child delivery, most women go through postnatal depression, which has been reported to be a factor for infant homicide. Women living with stepfathers of their children have also been noted to commit infant and child homicide.
Different treatment for women offenders than men
Despite the crimes and offences, the treatment of female offenders is lenient as compared to male offenders. It has been noted that women receive fewer sentences and punishment for similar crimes committed by male offenders. A study on male and female offenders in England in 2009 revealed that there were differences in sanctions given to men and women in the court. Female defendants for instance received fines as compared to male offenders at 77% female and male 63%. Lower female defendants received community sentences as compared to men who received suspended sentences. Immediate custody is more likely for men than women with 10% of males and 3% of females (NCJSR, 2011). Women seemed to be serving proportionately shorter custodial sentences as compared to men. Most women are remanded or serve shorter sentences for non-violent crimes than men. Results from gender differences and offender reentry revealed that all offender genders have the same categories of needs including mental health problems, vocational training, education, treatment for substance abuse and social support (Glaze, 2010). To benefit from the incarceration, their needs should be weighed and addressed appropriately for their benefits argues NCJSR (2009).
Possible reasons for differential treatment
Women are likely to receive better treatment than men in prison are. Self-harm incidents amongst women were higher accounting for 25.8% in 2013. 1549 cases of self-harm were reported amongst women as compared to 201 cases reported for men. The community orders for women are likely to have higher successful percentages than men thus leading to the gender differences. In 2013/14 for example 95% females and 75.8%males received successful community orders (FB1, 2010). Proven adjudications for women are at higher rates than men. The number of women released on a temporary license is also higher than the number of men. According to Flemke (2010), many women offenders have family responsibilities like children and being primary caregivers to the elderly or disabled relatives. It is thus easier for them to receive community projects as they continue taking care of their families.