Universal Healthcare Service Financial Planning Sample Answer
Introduction
Financial planning is an affirmative financial action that is spelled for a long period of time.
Universal Healthcare Service Financial Planning
It is established upon a set of goals in order to promote the mission and vision of a company. Financial planning is the most appropriate way of managing health sector budgets through allocation and well-targeted long-range solutions. It is a step by step financial process that enables the health institution achieves its strategic vision and dwell on its mission (Thompson, 2008)
Universal Health Service financial plan for the year 2012-2014
Step one: Mission and vision of Universal Health Services
Mission: Provide superior healthcare services that patients recommend to families and friends, physicians prefer for their patients, purchasers select for their clients, employees are proud of, and investors seek long term results.
Core Value: Service excellence, continuous improvement in measurable ways, employee development, teamwork, compassion, ethical and fair treatment.
Step two: Performance of Universal Health Service as compared to the past
According to the 2016 UHS annual report, its main focus is on provision of quality care to its patients as it improves its financial performance and efficiency. This is through more efficient use of professional and paraprofessional staff, monitoring and adjusting staffing levels and equipment usage, improving patient management and implementing more efficient billing and collection procedures. According to the recorded UHS’S financial information, the company’s income has been increasing. Net income attributable to UHS increased from $35 million to $545 million during 2014 as compared to $511 million during 2013 whereas it also increased from $67 million to $511 million during 2013 as compared to $443 million during 2012 (UHS, 2016).
UHS also dwells on corporate social responsibility by providing charitable care to patients who have a gross income of less than 400% of the federal poverty guidelines. This is in an attempt to improve the image of the institution and cooperate with the community. It does not pursue collection of amounts that qualify as charity care and are therefore not reported in its net revenues. The estimated cost of providing charity care in the years 2014, 2013 and 2012 was $78,475, $ 95,675 and $131,890 respectively (UHS, 2016).
Step three: A plan which incongruent with both the vision and mission of UHs based on its capital budgets
Capital budgets are majorly for the purposes of procuring projects, assets, and programs. They are long term budgets in themselves. According to (Mclean, 2003) a capital budget is one that assumes that the asset procured, will be pay to pay for itself through generating revenue or acquiring support through funding externally. This, therefore, means if the proposed asset is not in a position to pay for itself, then it should not be purchased.
Although UHS is a non-profit making hospital, the issue of capital budgeting is a matter of essence. It should be noted that over the years UHS has been on the front line to conduct acts of philanthropy to its organization. According to (UHS, 2016) the hospital has been ranked as a top performer through its registration of billions in earnings. In the year 2012, UHS collected a total of $(789,590) from all of its investing activities. The amount moved to even a higher notch in 2013 where cumulatively they acquired $ 884,241. And in 2014 a total amount of $1,035,876 was also gathered. All this endowment should be put in good use so as to assist in providing good patient care by constructing buildings, diversify the specialties available and also purchasing more land.
Step four: Harmonize the UHS’ financial goals together with its strategic goals
A good and long term image of an organization helps it maintain good credit. This in return helps it promote the strength of their credit (Thompson, 2008). A positive rating will only occur if the organization’s profit margin over the years is positive. In UHS, it has recorded a rise in profit margins over the three consecutive years. In 2012 it recorded $450,467 in 2013 $530,077and a higher amount in the year 2014 $544,921. The results are positive despite the fact many people have recently lost their medical covers.
Step five: Identify and evaluate both the micro and macro environments of UHS in order to create new opportunities.
This financial plan cannot be successful if UHS does not invest in evaluating the mentioned environments. This is done through constant reviewing of their financial positions and also the macro environment. Ensuring that all the strategic plans are based on its strength. UHS has a very strong management team that ensures that all departments result to yield revenues which amount to 73% of its total income (UHS, 2016). In the consecutive years that is 2012 -2014 UHS has developed from providing acute care hospitals to surgical and behavioral healthcare centers and in 2014 has introduced ambulatory surgery and radiation services.
Future decisions of UHS should be based on its big strength which is its managerial team and the fact that it has been recognized as the largest hospital. This new opportunities identified should provide a guideline on how financial projections can be developed by UHS. New opportunities are usually accompanied by risks. They include changes in cost of operation of activities, patient revenues and changes in productivity. All risks should be assessed. With new opportunities come expected net present values this ought to be assessed in order to evaluate the new opportunities then an optimal decision should be chosen (Mclean, 2003)
Step six: Evaluate and monitor all steps
According to the financial statements provided by UHS, their total operating revenue has continually increased. From 2012-2014 the sum amount of operating revenue rose from $ 799,231 to $1,035,876. This means that debts and funds are being well managed (McLean, 2003).
Universal Healthcare Service Financial Planning References
McLean, R. (2003). Financial management in healthcare organizations. new York: Clifton Park,.
Thompson, A. S. (2008). Crafting and executing strategy. New York: McGraw Hill:1-17.
UHS. (2016). 2014 Annual Report- Universal Health Services. UHS. New York: Retrieved from http://www.uhsinc.com/media/288196/2014-annual-report.pdf.
In this assignment we are going to look at Mrs Gwendolyn Harris. Mrs Gwendolyn Harris is an 82 year old war widow who has presented to the nurse practitioner wound management clinic after being referred by her GP Dr Greenwood. Six weeks ago she was scratched on the lower right leg by her cat Whiskers. The wound has not healed well. She has had increasing pain over the past six weeks which has been relieved to some degree after her daughter advised her to elevate her leg in the evenings. She has also been applying a small crepe bandage, which she has been washing every other day, to her lower leg daily to reduce the exudate soiling her clothes. Julia (the daughter) drives her mother to the vascular nurse practitioner (VNP) clinic. He reviews her bilateral Doppler ultrasound and bilateral ankle brachial pressure index (ABPI) results which confirm R) lower leg venous insufficiency and deep venous disease.
Mrs Gwendolyn has a Past medical history of ;Congestive cardiac failure (CCF), bilateral leg varicose veins, R) leg deep vein thrombosis (DVT) five years ago, gastrointestinal bleed (GI) bleed 10 years ago
She has a Past surgical history of; Cholecystectomy 40 years ago
Her Past family history include ;Sister, Jessie (deceased), cardiovascular disease (CVD), macular degeneration.
She is Allergic to Penicillin, Voltaren
In this assignment we are to discuss in-depth the pathophysiology of Gwendolyn’s condition firstly, therefore pathophysiology of pain and wound healing. We are then to identify objective and subjective data & formulate relevant actual or potential four (4) nursing issues based on the data presented in the scenario. The four (4) nursing issues identified for Gwendolyn are;
1) Chronic wound healing
2) Chronic pain
3) Poor eyesight
4) Hearing loss.
For each of the nursing issues identified above, we are to provide a brief pathophysiology for each one, provide excellent understanding of current evidence based practice and patient centred care. We are also to discuss the inter-professional roles likely involved, discuss/link pharmacology (Macuvision for her poor eyesight, antibiotics for her wounds and chronic pain management medication like Metronidazole, Ciprofloxacin), discuss lifespan issues (how her age can affect wound healing, Poor eyesight and hearing loss because of her age), discuss also briefly her psychosocial issues (she is a 82 yr. old widow living independently) This should be included for each of the nursing issues. We should demonstrate clear links between these concepts and the case scenario and nursing practice.
SAMPLE ANSWER
Pain has a warning damage as well as a protective function in nature, which calls for adequate medication and treatment of the affected areas as in the case of Mrs. Gwendolyn. Wounds resulting to pain is identified to have failed to heal in an orderly reparative process. The wounds lead to poor functional, and anatomy integrity due to pain that follows. Pain influences poor perfusion and low oxygen tension reduces the rate of collagen deposition in the tissues. Consequently, vasoconstriction follows due to severe pain which also impairs the healing of wounds. Infection, ischemia, nerve damage or the severe injury on the skin are the major causes of wound pain similar to the case of Mrs. Gwendolyn. The decrease of oxygen in the tissues results to production of low leucocytes which causes infection as the bacteria is given a chance to colonize the wound (Robb, 2016, pg. 56). In this case, the patient suffers severe pain and makes the healing process of the wound cumbersome. However, pain is identified to be a personal thing that is dependent on what the patient would express.
Etiology and pathology of pain dictate the sort of pain experienced by the patients. In this case, Mrs. Gwendolyn suffers from severe pain since the deep venous disease is a peripheral vascular problem which affects the healing process (Roberts et al, 2016, pg. 88). The deep venous disease in the patient also causes the venous ulcers which need to be addressed carefully through the right treatment and management strategies. Provision of a moist wound environment, compression therapy necrotic tissues’ debriment is essential during the pain and wound healing process of a patient (Bester & Van, 2015, pg. 79).
Patients with chronic wounds require quick management to prevent its progression to fatal stages causing severe pain. The accurate assessment of the patient’s pain progression is vital before the adoption of treatment strategies for chronic wounds. Venous insufficiency as identified in Mrs. Gwendolyn is one of the major causes that leads to the progression of wounds to be chronic. Other factors include arterial perfusion, unrelieved pressure, and immunosuppression. The chronic wound healing issue as identified is affected by many systematic and local factors (Robb, 2016, pg. 105). Age factor affects wound healing. The altered inflammatory process is related to impaired healing of chronic wounds among the elderly. Delayed infiltration of T-cell and chemokine production influence the delayed healing of chronic wounds among the elderly. Exercise is proved to enhance faster wound healing among the elderly. Elimination of the noxious stimuli and identifying the underlying cause is crucial while managing the chronic wound issues. Chronic wounds healing is closely associated with the high intensity of the acute postoperative pain.
It is essential to follow the patient centered care and evidence-based practices while treating patients with chronic wounds. While addressing chronic wound healing complications, there are various elements identified using TIME mnemonic device (Mehmood et al, 2015, pg. 112). The device is set to identify elements of chronic wound healing impairment. These elements include tissue surrounding the wound, infection or inflammation, moisture balance and edges blood supply. Preserving vital tissue is essential as there are many impediments that hinder optimal healing. Sharp debridement as an effective evidence-based practice used in the treatment of chronic wounds arising from venous related ulceration such as the patient in our case study. Topical antibiotics such as Vitamin A& D ointments, antacids, regranex, and collagen are used to enhance the faster and more efficient healing of chronic wounds (Mehmood et al, 2015, pg. 60). Silver-containing dressings are used in improving the healing rates for wounds. Nurses and other medical practitioners are supposed to treat the patient through proper dressing of wounds, enhancing adequate nutrition, ensuring proper tissue oxygenation as well as treating underlying infections. It is the role of the nurse to follow-up even after debriment and treatment of infections to ensure wound care is efficient to control chronic contamination of the wound (Rhee et al, 2015, pg. 109).
It is the professional role of nurses to provide wound management education and training to patients and their family members. Such measures and practices have been seen to improve the efficacy and quality of the treatment strategies used thus preventing the complication of situations. Optimal care should be provided to the patients, especially the elderly who have numerous cases of malnutrition which affects their wound healing process (Hosseini et al, 2016, pg. 93). The collaboration between the physician and patient enhances the better management of the chronic wounds.
The chronic pain is another nursing issue identified and requiring the quick address to prevents further complications experienced by the patient. The initiating causes and the patient’s threshold for pain is used in differentiating whether the pain is chronic or not. Multiple neurobiological mechanisms are said to contribute to pain making its categorization cumbersome (Lee et al, 2014, pg. 156). Nevertheless, some of the most common types of pain include nociceptive pain, central pain augmentation, and inflammatory pain. Aberrant somatosensory processing which occurs in the central nervous system is used to explain the chronic pain. Inflammation or damage to the tissue sensitizes nociceptors which are the nerve ending transmitting signals of pain in the nervous system (Scherer et al, 2016, pg. 112). Chronic pain is identified to be a persistent maladaptive response where psychological comorbidities are common.
Better pain management is made possible through adherence to the right evidence-based practices as well as the provision of patient-centered care to the patient. Such strategies would include understanding the pathophysiology of chronic pain appropriately before the administration of management strategies. Interventional and behavioral therapy should be combined as practices by the nurses while offering professional assistance to patients experiencing chronic pain (Fox et al, 2016, pg. 145). Full involvement of the family members and the patient would ensure they also contribute to making of clinical decisions towards their treatment making management of situations such as chronic pain more efficient in nature. Rehabilitation practices such as occupational, physical and cognitive therapy are used in the management of chronic pain reducing medication needs (Lukewich et al, 2015, pg. 92). Various drugs such as simple analgesics, opioid, and tricyclic antidepressants are used as the medication for treating patients with chronic pain (Scherer et al, 2016, pg. 156). It is the role of the nurse to offer proper clinical guidance to the patient as well as the prescriptions of drugs. Anti-inflammatory drugs are used in the management of pain among patients. Other medication drugs include ciprofloxacin and metronidazole (Patel et al, 2016, pg. 135).
The inter-professional role of the nurse ensures that approach of pain management is organized in nature. The approach entails, routine chronic pain evaluation, encouraging patients to share their chronic pain experiences, adopting evidence-based practices during treatment as well as selective modification of opioid regulatory policies and practices. Adherence to Consistent pain management strategies and minimizing pain is the major role performed by those caring for the patient. The psychosocial issues should be handled effectively; it is most likely that the woman feels lonely which might also affect her recovery process (Rommem et al, 2015, pg. 137). It is essential to administer therapies and advice that a person is attached to the patient to offer her necessary support. Nurse Follow-up of her medication and treatment, while she is at home, would help alleviate the psychosocial issues that could affect her recovery.
Poor eyesight is another nursing issue identified and requires proper management. Poor eyesight causes people to have a blurry vision which makes various objects appear hazy or seems to be out of focus. Some of the poor eyesight problems include astigmatism, refractory errors and also presbyopia (Waldron, 2012, pg. 43). A comprehensive eye assessments such as Snellen eye chart and the spatial contrast sensitivity test would be helpful in identifying the particular eyesight problem. Age has been consistently identified as a factor influencing poor eyesight among patients (Wadlron, 2012, pg. 64). There is macular degeneration which is age-related and leads to blurry vision and gradual loss of vision. The elderly also experience distortions which can lead to blindness at the end. The patient in our cases study has a family history of macular degeneration which can be a cause of her poor eyesight problems due to genetic factors. Through macular degeneration, the central vision would become blurred due to damage of macula. Age is a major contributing factor since most people suffering from poor eyesight problems are above the age of 65years while the risk rises with the increase in age (Dutta et al, 2015, pg. 117). Other than macular degeneration vision impairment in the elderly patient would result due to cataract and glaucoma.
Treatment and management of poor eyesight problems to prevent the progression to severe stages is essential when caring for the patients. The diagnosis of poor eyesight problem should be done correctly before undertaking any treatment strategies. Treatment is dependent on specific causes. Psychosocial reasons such as stress and loneliness might hinder the patient from taking care of herself well even to follow the diet that helps improve eyesight (Willis et al, 2016, pg. 138). In this case, it is vital to have a caregiver who is there almost all times. Alterations in vision, especially among the old, is detected using Amsler grid (Simsek et al, 2015, pg. 143). To reduce the risks of suffering from the age-related macular degeneration (AMD), intake of foods with high levels of carotenoids is useful. Foods rich in zeaxanthin and lutein are also required to solve the problem. Mineral supplements and antioxidant vitamin are offered to the patient to manage the situation (Sismek et al, 2015, pg. 73). Complete blindness is not related to AMD, thus the management of poor eyesight is easier. Radiation therapy and provision antiangiogenic drugs are recommended among the evidence-based practices to manage poor eyesight.
Hearing loss results from poor or lack of sound transmission to the cochlea. Hearing loss is usually categorized into various levels such as slight, mild, moderate, severe and profound hearing losses. Presbycusis is one of an age-related hearing loss problem which is experienced among the elderly people like Mrs. Gwendolyn (Werfel et al, 2016, pg. 75). The hearing loss gradually progresses as one gets old with time. Equal effects are experienced in both ears when one is affected by the problem. Past medications toxic to ensory cells, past medical conditions such as hypertension or chemotherapy drugs influence hearing loss among elderly people. Hearing loss affect the functioning of the tympanic membrane (Schlauch et al, 2015, pg. 83).
It is the professional role to involve the patient and the family actively in training and educating about hearing loss. Referral of patients to special programs or audiologist to assist in improving auditory reception is important. Social workers can also be assigned to those who already suffer from hearing loss to assist them in their daily activities since elderly people have psychosocial problems which call for the caregiver to be present (Rudner et al, 2016, p.g 70). The management and provision of patient-centered care are essential for the elderly patient during prevention or treatment of the problem (Van et al, 2016, p.g 112).
References List
Bester, P, & Van Deventer, Y 2015, ‘Holistic care for patients living with chronic wounds’, Wound Healing Southern Africa, 8, 2, pp. 78-81, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Dutta, S, Caplan, D, & Marcinko, D 2014, ‘Blurred Vision, Perilous Future: Management Fraud at Olympus’, Issues In Accounting Education, 29, 3, pp. 459-480, Business Source Complete, EBSCOhost, viewed 3 August 2016.
Fox, L, Walsh, J, Morrison, T, O’ Gorman, D, Ruane, N, Mitchell, C, Carey, J, Coughlan, R, & McGuire, B 2016, ‘Cognitive Coping Style and the Effectiveness of Distraction or Sensation-Focused Instructions in Chronic Pain Patients’, Plos ONE, 11, 4, pp. 1-12, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Hosseini, S, Idani, I, Rashidi, S, & Yadollahpour, A 2016, ‘Ultrasound based techniques for treatment of chronic Wounds: A comprehensive review of therapeutic efficacies and clinical considerations’, International Journal Of Pharmaceutical Research & Allied Sciences, 5, 2, pp. 387-397, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Lee, C, Crawford, C, Teo, L, & Spevak, C 2014, ‘An Analysis of the Various Chronic Pain Conditions Captured in a Systematic Review of Active Self-Care Complementary and Integrative Medicine Therapies for the Management of Chronic Pain Symptoms’, Pain Medicine, 15, pp. S96-S103, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Lukewich, J, Mann, E, VanDenKerkhof, E, & Tranmer, J 2015, ‘Self-management support for chronic pain in primary care: a cross-sectional study of patient experiences and nursing roles’, Journal Of Advanced Nursing, 71, 11, pp. 2551-2562, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Mehmood, N, Hariz, A, Templeton, S, & Voelcker, N 2015, ‘A flexible and low power telemetric sensing and monitoring system for chronic wound diagnostics’, Biomedical Engineering Online, 14, 1, pp. 1-17, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Patel, T, Chang, F, Mohammed, H, Raman-Wilms, L, Jurcic, J, Khan, A, & Sproule, B 2016, ‘Knowledge, Perceptions and Attitudes toward Chronic Pain and Its Management: A Cross-Sectional Survey of Frontline Pharmacists in Ontario, Canada’, Plos ONE, 11, 6, pp. 1-14, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Rhee, S, Valle, M, Wilson, L, Lazarus, G, Zenilman, J, & Robinson, K 2015, ‘Negative pressure wound therapy technologies for chronic wound care in the home setting: A systematic review’, Wound Repair & Regeneration, 23, 4, pp. 506-517, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Robb, C 2016, ‘Chronic wound management’, Chemist & Druggist, 284, 6965, pp. 12-14, Business Source Complete, EBSCOhost, viewed 3 August 2016.
Roberts-Turner, R 2016, ‘Quality Improvement. Pain Management: An Evidence-Based Approach’, Pediatric Nursing, 42, 1, pp. 39-49, Professional Development Collection, EBSCOhost, viewed 3 August 2016.
Romem, A, Tom, S, Beauchene, M, Babington, L, Scharf, S, & Romem, A 2015, ‘Pain management at the end of life: A comparative study of cancer, dementia, and chronic obstructive pulmonary disease patients’, Palliative Medicine, 29, 5, pp. 464-469, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Rudner, M, Mishra, S, Stenfelt, S, Lunner, T, & Rönnberg, J 2016, ‘Seeing the Talker’s Face Improves Free Recall of Speech for Young Adults With Normal Hearing but Not Older Adults With Hearing Loss’, Journal Of Speech, Language & Hearing Research, 59, 3, pp. 590-599, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Scherer, M, Hansen, H, Gensichen, J, Mergenthal, K, Riedel-Heller, S, Weyerer, S, Maier, W, Fuchs, A, Bickel, H, Schön, G, Wiese, B, König, H, van den Bussche, H, & Schäfer, I 2016, ‘Association between multimorbidity patterns and chronic pain in elderly primary care patients: a cross-sectional observational study’, BMC Family Practice, 17, pp. 1-8, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Schlauch, R, Koerner, T, & Marshall, L 2015, ‘Effective Identification of Functional Hearing Loss Using Behavioral Threshold Measures’, Journal Of Speech, Language & Hearing Research, 58, 2, pp. 453-465, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Şimşek, Y, Şenol, S, Canöz, Ö, Selçuklu, A, Diri, H, & Keleştimur, F 2015, ‘A Case of Pituicytoma Presenting with Blurred Vision and Hormone Deficiency’, Turkish Journal Of Endocrinology & Metabolism, 19, 3, pp. 115-118, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Van Eynde, C, Swillen, A, Lambeens, E, Verhaert, N, Desloovere, C, Luts, H, Vander Poorten, V, Devriendt, K, & Hens, G 2016, ‘Prevalence and Nature of Hearing Loss in 22q11.2 Deletion Syndrome’, Journal Of Speech, Language & Hearing Research, 59, 3, pp. 583-589, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Waldron, J 2012, ‘Talking labels boost compliance in patients with poor eyesight’, Chemist & Druggist, 278, 6834, p. 11, Business Source Complete, EBSCOhost, viewed 3 August 2016.
Werfel, K, & Hendricks, A 2016, ‘Identifying Minimal Hearing Loss and Managing Its Effects on Literacy Learning’, Teaching Exceptional Children, 48, 4, pp. 213-217, Professional Development Collection, EBSCOhost, viewed 3 August 2016.
Willis, J, & Ramulu, P 2016, ‘Poor Vision and Self-Reported Functional Difficulties among Recently Hospitalized Individuals in the United States’, Ophthalmic Epidemiology, 23, 3, pp. 154-161, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
We can write this or a similar paper for you! Simply fill the order form!
APA REF. NOT OLDER THEN 5 YEARS.
ALL RESEARCH SHOULD BE VALID IN AUSTRALIA.
CASE STUDY IS HERE. PLEASE REFER TO FILES ATTACHED FOR MORE INFO
John Gray
28 years old
Severe depression following suicide attempt
?
Mr John Gray is a 28 year old single male admitted to the unit a week ago after an episode of intentional self-harm. John is the son of a grazier from a farming community north of Brisbane who is expected to take over the family farm. The farm has been severely affected by the longstanding drought conditions in the district. You are the nurse assigned to John’s care for the afternoon shift. On handover you were informed John did not get up for breakfast again, went to lunch reluctantly only because he was compelled to but ate almost nothing, and returned to his bed immediately afterwards. His routine morning observations were: Blood pressure 125/75, Temperature 36.3, Pulse 66, Respirations 18. John has a rope burn mark on his neck caused by the breaking of the rope with which he attempted to hang himself and some bruising and broken skin on his arms and legs from the subsequent fall but no serious physical injuries. The areas of broken skin were covered with a non-adherent dressing and tape. The occupational therapist reported John was still choosing not to take part in any activities, including small group games or one-on-one activity.
When you go to introduce yourself to John, you find him lying on his bed with the covers pulled up high. He appears reluctant to engage in conversation with you. When you address him to introduce yourself, he grunts and turns over to face the wall away from you.
Medications:
Venlafaxine 75 mg bd
Multivit i daily
Vit B co i daily
SAMPLE ANSWER
Introduction
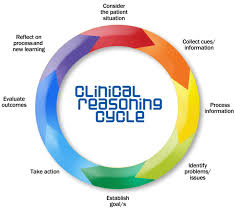
Clinical reasoning can also be termed as critical reasoning or clinical judgment (Kelton, 2014). It is the sourcing of clues about the patient’s symptoms in order to establish the cause of epidemiology rather than simply how to treat it. By looking at patient history, determining factors to the ailment and assessing response to previous medication, nursing staff can learn the patient’s immune system and propose better ways to treat the patient (Rugen et al, 2014). Clinical reasoning is a tactic in evident based practice. It comprises of; consideration for patient situation, collection of cues and data about the patient, processing these cues/information, identifying the problem or issue at hand, establishing treatment goals, taking action to administer treatment, evaluating the outcome of the treatment and reflecting on the outcome (Tsingos, Bosnic-Anticevich & Smith, 2014). This can be represented in the diagram below;
Considering the patient situation
Consideration for the situation of the patient involves aspects such as; listening to what the patient says, what their relatives say about the patient and assessing the condition. In some cases such as emergency nursing treatment where the cause for treatment is injury, little information is required to start the treatment (Jefford, 2012). There are indeed cases where the entire clinical reasoning process will not apply. However, clinical reasoning is very effective for chronic patient cases that include patients with cancer, arthritis, asthma, Leukemia and challenges such as kidney failure, diabetes and ulcers (Staveski, Leong, Graham & Roth, 2012).
Gathering Health Information
Health information can be gathered in many ways. The most popular of these ways is to check insurance records. The patient is to be made aware that such information is important for their treatment thus should be retrieved with their consent (Forbes & Watt, 2015). All records and files stored on chronic patients present a plethora of useful information that can really help nurses in offering care to the patients (Cockerham et al, 2011). For instance, a patient who has been catheterized needs to make it known before medical procedures are undertaken on them. Such knowledge may however not be present beforehand if the patient is brought in by non-relatives in a comatose /unconscious state of mind. Knowledge on past treatments helps avoid allergic reactions in current treatments as well (Andrew & Robb, 2011). It is thus important for nursing staff to be aware that they will require such information early hence begin looking for ways to source it.
Processing Information
With the entire information ready, there is need to process the information as it is. For instance, in the case of John, the patient in this case study, his history of causing self-harm cannot be easily diagnosed without having prior information on what the motivation for the harmful activities is. John’s friends and relatives can give the impression that he may have bipolar disorder, hyperactivity disorder, depression or an anxiety disorder. However, it is important to know if John has been using any drugs that may have either led to his disorders or aggravated the situation in the past. Currently, he is on Venlafaxine (anti-depressant medication), multivit (a dietary supplement) and vit B (Thiamine, Riboflavin and pantothenic acid). These medications indicate treatment for an eating disorder as well as depression.
Identifying the problem
The next step is to find out why Mr. John is depressed. It could be as a result of family, work or social issues. This information cannot be acquired from any other persons but the closest family members. Interviewing these family members would indicate reasons Mr. John may have been stressed to the point that he chose not to eat. In clinical reasoning, there is no assumption made. Every little detail about the person has to go into the preparation of the diagnosis (Bratt, 2013). Finding out the main reason for Mr. John’s stress can lead to the proper therapeutically-induced intervention for the patient. He may for instance need counseling more than he needs the medication he is on. Additionally, testing the patient’s vitals is very important in any diagnosis (Dariel, Raby, Ravaut & Rothan-Tondeur, 2013). From the vitals given; 125/75 mmHg, 36.30C, Pulse 66 and Respirations 18, he seems to be out of danger at the moment. Therapy thus seems to be the imminent treatment option.
Nursing Problems Based on Health Assessment
One of the key issues that I have identified from the provided case study is lack of patient cooperation. It is reported that Gray avoids engaging in conversations with health providers. This can result in ineffective delivery of patient care as they clinicians cannot properly tract the progress of Gray and provide quality care to him.
I am also concerned about Gray’s neck injuries and whether they could be linked to the depression that he is currently suffering from. Research by Cockerham et al., (2011) reports that severe neck or back pain can trigger can result in increased stress and depression. As a nurse, it is crucial to conduct a diagnosis aimed at determining whether the depression is lined to the pain.
The other nursing issue that perturbed me is Gray’s behavior of not eating or participating in recreational activities. Forbes & Watt (2015) enlighten that diet and activity are among the leading contributors of effective recovery from depression. Increasing the number of activities aids depressed patients such as Gray to cope with depression. Therefore, as a nurse I will encourage Gray to participate in events that he used to enjoy.
Goals for priority of Nursing care
Goals for priority of nursing care are based on various principles assigned within the clinical reasoning cycle. The most important goal is to ensure that all information acquired from interviewing John’s contacts is captured and recorded for future use. The next goal is to ensure that error omission is guaranteed by progressively seeking additional information to help in the diagnosis and treatment of the patient. Whether the information provided seems significant or not, it is vital to consider each new piece of information gained (Alfaro-LeFevre, 2012). It is also vital to ensure that the incorporation of pathophysiological knowledge into the treatment is balanced with the use of previous data and current information from significant sources.
Nursing Care for John
John is on the right track to recovery based on the medication given to him. However, the treatment of mental disorder and eating disorder is not sufficient. He needs to be under constant surveillance without making it seem like he is being monitored. He also needs to seek counseling. However, many patients often face denial and may not be willing to take this step. As a result, the primary nursing solution would be to talk to John about his actions and over time, get him to admit that he needs psychological help. By doing so, John can be fully assisted and on the road to recovery. The medication he is taking needs to continue, as long as he is not cleared of his psychological problem by a psychologist. In priority nursing care, it is important to incorporate professional advice from colleagues and supervisors (LeMone et al., 2015). This diagnosis thus needs to be discussed with other senior nursing officials to establish the degree of accuracy in the diagnosis.
Evaluating outcomes
The outcomes anticipated by the proposed nursing care for John include; admission of depression or mental problem, agreement to consult psychologist or the use of the hospital-appointed psychologist, being more open about his issues and restoration of his former life. John has to eventually continue being a father, husband and colleague to friends and family. He thus ought to begin treatment that will make him open up about the problems he faces. The importance of these strategies is that at the end of the day, John needs to be treated. The medication he is using works on him but it is apparent that he does not take it willingly. He needs to have an attitude change to accept medication before any medical intervention can work (Staveski, Leong, Graham & Roth, 2012).
Reflection
John’s case is not an isolated one. He seems to be struggling with depression-related problems. These problems are social in nature (Alfaro-LeFevre, 2012). There is need however to incorporate evidence-based practice in the treatment of John’s depression that has led to eating disorders, attempted suicide and self-inflicted injuries. Therapy seems to be the best option. However, before he begins the therapy, John needs to take his medication and lower stress levels. Once this has been done, he can then be treated and offered the necessary counseling to deal with his depression.
References
Alfaro-LeFevre, R. (2012). Applying nursing process: the foundation for clinical reasoning. Lippincott Williams & Wilkins.
Andrew, N., & Robb, Y. (2011). The duality of professional practice in nursing: Academics for the 21st century. Nurse Education Today, 31(5), 429-433.
Barker, J. (2013). Evidence-Based Practice for Nurses: SAGE Publications. Sage.
Bratt, M. M. (2013). Nurse residency program: Best practices for optimizing organizational success. Journal for nurses in professional development,29(3), 102-110.
Cockerham, J., Figueroa‐Altmann, A., Eyster, B., Ross, C., & Salamy, J. (2011, October). Supporting newly hired nurses: A program to increase knowledge and confidence while fostering relationships among the team. InNursing Forum (Vol. 46, No. 4, pp. 231-239). Blackwell Publishing Inc.
dit Dariel, O. J. P., Raby, T., Ravaut, F., & Rothan-Tondeur, M. (2013). Developing the Serious Games potential in nursing education. Nurse education today, 33(12), 1569-1575.
Forbes, H., & Watt, E. (2015). Jarvis’s Physical Examination and Health Assessment. Elsevier Health Sciences.
Jefford, E. (2012). Optimal midwifery decision-making during 2nd stage labour: the integration of clinical reasoning into midwifery practice.
Kelton, M. F. (2014). Clinical Coaching–An innovative role to improve marginal nursing students’ clinical practice. Nurse education in practice,14(6), 709-713.
LeMone, P., Burke, K., Dwyer, T., Levett-Jones, T., Moxham, L., & Reid-Searl, K. (2015). Medical-surgical nursing. Pearson Higher Education AU.
Levett-Jones, T., Hoffman, K., Dempsey, J., Jeong, S. Y.-S., Noble, D., Norton, C. A., . . . Hickey, N. (2010). The ‘five rights’ of clinical reasoning: An educational model to enhance nursing students’ ability to identify and manage clinically ‘at risk’ patients. Nurse Education Today, 30(6), 517-519.
Rugen, K. W., Watts, S. A., Janson, S. L., Angelo, L. A., Nash, M., Zapatka, S. A., … & Saxe, J. M. (2014). Veteran affairs centers of excellence in primary care education: transforming nurse practitioner education. Nursing outlook, 62(2), 78-88.
Schmidt, N. A., & Brown, J. M. (2014). Evidence-based practice for nurses. Jones & Bartlett Publishers.
Staveski, S., Leong, K., Graham, K., Pu, L., & Roth, S. (2012). Nursing mortality and morbidity and journal club cycles: paving the way for nursing autonomy, patient safety, and evidence-based practice. AACN advanced critical care, 23(2), 133-141.
Tsingos, C., Bosnic-Anticevich, S., & Smith, L. (2014). Reflective practice and its implications for pharmacy education. American journal of pharmaceutical education, 78(1).
We can write this or a similar paper for you! Simply fill the order form!
Handling a Patient who Complains about Pain Order Instructions: APA reference not older than 5 years old
ALL RESEARCH SHOULD BE FROM AUSTRALIA CREDIBLE SOURCES I.E. JOURNALS AND ARTICLES ONLY.
All students are required to attend an interview when applying for a New Graduate Program or a Registered Nurse Position.
Handling a Patient who Complains about Pain
As part of the interview process, you will be required to reflect on your past clinical experiences when answering interview questions. For this assessment task students are required to answer the following interview questions:
1. How would you handle a patient who constantly complains about pain? (reflective writing)
Using the E.A.R (event, action, result) interview method and your reflective skills provide a written (800 word) summary to this question. You are also required to refer to the criterion-referenced rubric on page 13 of the unit outline. This rubric will also form the basis of your feedback for this assessment item
The length and/or format: 800 words
Handling a Patient who Complains about Pain Sample Answer
Handling a Patient who complains about Pain
Event
I recently encountered a patient who complained of severe headaches. He said that his headaches began just after a nasty bout of vomiting, which he attributed to spoilt milk. The pain was pulsing and throbbing, and every time he moved it became even more painful. It was specific to one side of the head. He also experienced a sharp sensitivity to light, and a visual disturbance just before the headaches began.
His chief complaint, however, was the throbbing pain, which would occur at least once a fortnight. The headaches would last to a maximum of twelve hours, after which he would feel quite well. The recent attack, however, lasted for twenty-four hours and in this case, the pain was throbbing. The regularity and severity of his pain indicated that he was suffering from a migraine. As a result, he did not go to work, as it involved a lot of movement, resorted to dark places and ate less to reduce the regularity of vomiting.
Handling a Patient who Complains about Pain and Action: Diagnosis and Treatment of the Migraine
As I was asking him about his symptoms, I took note of everything he told me to the detail. I noted that the headaches started when he was quite young, and was worsened every time he moved. My diagnosis of the patient was a migraine. I arrived to this conclusion after observing that the headaches were a recurring symptom and had started while he was quite young. To confirm my diagnosis, I consulted the doctor, who asserted the diagnosis.
To reduce the severity of his pain, I advised the patient to reduce the frequency of movement every time he had an attack. As his migraine was accompanied by a sensitivity to light, I advised him to stay in relatively darker places when he had an attack. I advised him against eating less during his attacks, as he did this to prevent more vomiting. Instead, I suggested that he should eat regularly and healthily, to boost his immune system. Enough sleep would also go a long way in reducing the severity of him a migraine. Sleep, I informed him, relaxes the mind, hence reducing stress, which could lead to a migraine.
He would also require medication. There are two types of treatment plans for a migraine: abortive prescriptions and preventive antibiotics (Lau & Nissen, 2015). Both prescriptions were administered to the patient. The abortive prescriptions would aid to reduce the head pain he was experiencing, and get rid of the accompanying symptoms. The preventive medications would be to reduce the severity and frequency of future migraines. I also warned that the preventive antibiotics might be accompanied by a few side effects. These side effects included nausea, sleepiness, fatigue and a bit of physical weakness (Martin et al., 2014). However, I assured him that the cases of people experiencing these side effects were few.
Biofeedback is another important technique that has been used in the management of patients with a migraine. The patient was taught about how to use special equipment so that he can assess and regulate different physical responses that are associated with stress such as muscle tension. The patient was also advised to take meals that are rich in riboflavin such as beef, yoghurt, and spinach as and magnesium such as whole grains and wheat bread which have been shown to be effective in the management of migraines.
I further advised the patient to follow the instructions on the medications to the letter as this was the only way the desired therapy of medications would be achieved. Moreover, the patient was given a phone number where he could call the support team at the health center whenever he had felt something is wrong or had a question regarding his health.
Rolan, (2014) reports that some of the common factors that have been cited to trigger the onset of migraines include fatigue, lack of sleep, certain foods, as well as the use of medications especially the vasodilators which increase blood flow to the brain. I therefore made it clear to the patient that it is of great importance for him to stay away from these triggers. Moreover, I encouraged the patient to have a daily diary where he can document the sequence of his headaches. This is an inexpensive as well as an effective tool the will be useful in following up the course of the patient’s condition.
Result: The Patient after Treatment
The patient before treatment was experiencing difficulty with movement and had stayed home from work as his job included a lot of movement. After treatment, he was able to move comfortably without experiencing debilitating pain. His sensitivity to light reduced and he became once more comfortable enough to stay in a well-lit room. He was more relieved by the fact that he no longer felt the excruciating throbbing pain to one side of the head. The preventive drugs that were given to him reduced the occurrence of the headaches he felt were normal, and the severity of pain during one of the attacks was also reduced.
Handling a Patient who Complains about Pain References
Hale, N., & Paauw, D. S. (2014). Diagnosis and treatment of a headache in the ambulatory care setting: a review of classic presentations and new considerations in diagnosis and management. Medical Clinics of North America, 98(3), 505-527.
Lau, E., &Nissen, L. (2015). Nausea associated with migraines. Australian Journal of Pharmacy.
Martin, P. R., Reece, J., Callan, M., MacLeod, C., Kaur, A., Gregg, K., &Goadsby, P. J. (2014). Behavioral management of the triggers of a recurrent headache: a randomized controlled trial. Behaviour research and therapy, 61, 1-11.
Silberstein, S. D. (2016). Considerations for the management of migraine symptoms in the primary care setting. Postgraduate medicine, 128(5), 523-537.
Rolan, P. E. (2014). Understanding the pharmacology of a headache. Current opinion in pharmacology, 14, 30-33.
Stark, R. J., Ravishankar, K., Siow, H. C., Lee, K. S., Pepperle, R., & Wang, S. J. (2013). Chronic migraine and chronic dailheadache in the Asia-Pacific region: a systematic review. Cephalalgia, 33(4), 266-283.
Pietrobon, D., & Moskowitz, M. A. (2013). Pathophysiology
of migraine.Annual review of physiology, 75, 365-391
This week 4 assignment is actually due on sunday. So please do it as fast as possible. Please use the same health care finance book.
SAMPLE ANSWER
Assignment Week 4
Assignment Exercise 8-3: Depreciation Concept
As expected, an asset will decline in value over a given period of time depending on several factors (Baker & Baker, 2013). However, the amount of depreciation will differ based on the type of method used. In this case, the two purchased equipment in MHS will have different depreciating values when the straight line and the double-declining balance depreciation methods are used as demonstrated below.
The Straight Line Depreciation
MHS’s Lab Equipment
Year
Annual Depreciation
Remaining Balance
Beginning Balance =
$300,000
1
57,000
228000
2
57,000
171000
3
57,000
114000
4
57,000
57000
5
57,000
0
Depreciation will not be deducted from the beginning balance but the remaining balance after removing the 5% salvage cost.
300,000 * 95% = $ 285,000
$ 285,000 will then be divided by 5 years to get an equal amount of the depreciating value.
MHS’S Radiology Equipment
Year
Annual Depreciation
Remaining Balance
Beginning Balance =
$800,000
1
102857.14
617142.86
2
102857.14
514285.72
3
102857.14
411428.58
4
102857.14
308571.44
5
102857.14
205714.3
6
102857.14
102857.16
7
102857.14
0
If the salvage value is salvage value (10%) the depreciating amount will be 90% * 8000 = 720000
The Double-decline Balance Depreciation
MHS’s Lab Equipment
In this case, 95% will be divided by 5 years to give 19% which will then be doubled to 38%. The 38% will be multiplied by the remaining depreciating balance of $285,000. However, this method will have the last two years will use the straight line method (Droms & Wright, 2015). Therefore;
Year
Annual Depreciation
Remaining Balance
Beginning Balance =
$300,000
1
108300
176700
2
67146
109554
3
41,630.52
67923.48
4
33961.74
33961.74
5
33961.74
0
MHS’S Radiology Equipment
90% of the remaining balance divided by 7 years will give 12.86% which is then doubled to 25.71% and used as the multiplying factor. Therefore;
Year
Annual Depreciation
Remaining Balance
Beginning Balance =
$800,000
1
187200
532800
2
138528
394272
3
102510.72
291761.28
4
75857.93
215903.35
5
56134.87
159768.48
6
79884.24
79884.24
7
79884.24
0
References
Baker, J. J., & Baker, R. W. (2013). Health care finance. Jones & Bartlett Publishers.
Droms, W. G., & Wright, J. O. (2015). Finance and accounting for nonfinancial managers: All the basics you need to know. Basic Books.
We can write this or a similar paper for you! Simply fill the order form!
Rubric Criteria for Mini Research Paper
4 pages total including title page, and reference page.
Concise and to the point (less is more, quality instead of quantity)
Must be in APA format Word document or PDF
Title page in APA format,
4 key points that best exemplifies my National Patient Safety Goal. ( my 4 point are: 1.risk assessment and preventive interventions in the hospital for risk of suicide of Veterans. 2. risk assessment in the hospital for risk of suicide for cancer patient, 3.assessing the risk for suicide in adolescents , 4. risks associated with home oxygen therapy, such as home fires for smocking patients.
Introduction:
State the National Patient Safety goal you have researched, the background on this problem and why it is important for patients and nurses to follow this goal
Body of Paper:
Review of four (4) nursing journal articles on your assigned National Patient Safety goal!!!! (Goal 15: Risk assessment for patient population: 1)Identify patients at risk for suicide, applies to:Behavioral Health Care, Hospital, 2)Identify risks associated with home oxygen therapy, such as home fires, applies to: Home Care
4 articles must be no more than 5 years old, 2011-2016.
Give a brief synopsis of each article and state the main points.
Conclusion
Wrap up what you read and why this is so important to healthcare/nursing
Reference page
Separate page for references, total of four (4) in APA format. SAMPLE ANSWER
National Patient safety
Introduction
Patient safety is critical in ensuring the best possible outcomes for healthcare institutions. However, some conditions and treatments pose higher risks for patients due to their nature such as high and lethal dosage of cancer drugs, home oxygen, and suicidal thoughts for veterans and adolescents who might be suffering from psychological conditions. It is important for nurses and other healthcare personnel to assess the risks that are posed in each patient cases, and come up with ways of reducing the risk levels, or having them eliminated at once. It is critical to be aware of the risks that different patients are exposed to, and the means through which the safety of patients can be improved.
Improving patient safety through reduction of risks
This part of the health safety paper will cover four journals on different risks that different patients might suffer from. The sections will also cover the actions that can be implemented by health professionals to ensure reduction of risks to patients and their loved ones.
Identify risks associated with home oxygen therapy, such as home fires, applies to: Home Care
According to Cooper (2015), 14-51% of cigarette smokers continue with their habit; which endangers those that use oxygen in their homes. The presence of oxygen in the homes contributes to an improvement of the health of those that are ailing. However, it also contributes to an increase in the risk of flammability in the home. Unfortunately, most cigarette smokers in places with home oxygen fail to report the exact danger that their habits might cause the individuals probably feel some guilt because of the increased risks and dangers that they pose to their loved ones and homes. In 2010, about 4.3% of the United States population as estimated to have experienced home fires based on data from an extrapolation in Maine. Tobacco smoking, cooking, flammable materials, and outdoor fire related activities were blamed as some of the greatest contributors to home fires in the country and globe. Countries such as Finland and Romania had the highest rates of fires while Switzerland and Italy had the lowest level of oxygen related home fires that resulted in deaths in Europe, between 2008 and 2010. The level of home oxygen fires is greater among elderly patients which could be attributed to the poor physical agility in comparison to that of younger individuals. Healthcare professionals have an ethical duty to ensure that they contribute to the reduction of fires especially for elderly patients and their relatives and neighbors. Most tobacco smokers allege that they have an addiction, and might therefore experience difficulty in trying to quit their habit. The home oxygen containers are fitted with safety fittings or tubing to minimize the flow of oxygen in case of fires especially in elderly home cares where patient mobility is likely to be low.
Predictive modeling and concentration of the risk of suicide: implications for preventive interventions in veterans
According to McCarthy et al (2015), there has been a high rate of suicides among veterans in the country (US). The health system concerned with the well-being of veterans (Veterans Health Administration) initiated a program to ensure a steady reduction or maintenance of a low number of suicides among veterans. The VHA program did not contribute to a dramatic reduction in the number of suicides among the intended population, but resulted in a stable rate of suicide control in comparison to the rate of suicide among other populations. According to McCarthy et al. (2015), a predictive modeling can be utilized in finding out the at risk individuals among the population, and therefore reduce the number of individuals that commit suicide. Based on the results of the modeling, action steps would be implemented to ensure the reduction of the number of those at risk, and offering of treatment services. Those that portray risks of suicide should be involved in community or clinical based support groups based on the level of indications that they exhibit. The health department has also proposed the ease of access and counseling for pain management related patients; as a means of reducing the rates of suicides among veterans and general population. According to McCarthy et al (2015), homeless unmarried males were more likely to contemplate and execute suicidal thoughts in comparison to those individuals that had support from their family members.
Assessing the risk for suicide in patients with cancer
All chronically ill patients might suffer psychological stress in addition to their physical symptoms. Some cancer patients might feel that suicide would be a means of dying with dignity since their health keeps on deteriorating. Some healthcare professionals such as nurses might share these views, and therefore increase the risk of successful suicides for the patients. Therefore, there is a need for a high level of assessment and knowledge regarding patient safety for cancer related patients; in reducing suicide levels. According to Aiello-Laws (2010), the cancer patient might be contemplating suicide due to untreated depression or anxiety. The nurses and other healthcare patients that are around the cancer patients should ensure that there are no lethal substances or objects that are left around the patients. The cancer patients might inject themselves with lethal doses of drugs or cut themselves with sharp objects. For patients that are residing outside hospital confines, the nurses should involve the family or loved ones of the patient in ensuring the reduction of risks to increase safety. Social workers or religious leaders could be involved in the offering of visits to cancer patients that live alone so that they get encouragement and guidance that would encourage them.
A process model for assessing adolescent risk for suicide
The level of suicides among adolescents has increased over the last two decades; at an alarming rate. Most of the adolescents suffer from depressive or bi-polar conditions which contribute to an increase in their suicidal tendencies and thoughts. Adolescents who had attempted to commit suicide in the past were 18 more times likely to attempt suicide a second time. The social conditions around the adolescents such as bullying or subjection to abuse are also likely to contribute to an increased likelihood of abuse among adolescents. If adolescents are bullied, they are likely to contemplate committing suicide especially if they come from unstable homes. The adolescents would feel unappreciated and likely succumb to peer pressure or the negativity around them. The young individuals are also likely to have higher levels of suicidal thoughts if they are engaged in substance abuse. According to Stoelb & Chiriboga (1998), counseling and involvement in physical activities such as sports offers some of the best ways of ensuing patient safety among adolescents that contemplate suicide.
Conclusion
Patient safety is one of the most critical goals for the healthcare industry Nurses and other healthcare professionals have the duty of ensuring that patients do not suffer any danger or avoidable death as a result of their environment or untreated psychological state. Depressed individuals that contemplate suicide should be kept away from harmful agents and objects that would increase their likelihood of committing suicide.
Patients that smoke or have increased risks that could contribute to fires for home oxygen users should be briefed on possible accidents that could occur. Where necessary, the fire department should be involved in the assessment and briefing of the possible risks of fires for home oxygen users.
References
Aiello-Laws, L.B. (2010). Assessing the risk for Suicide in patients with cancer. Clinical Journal of Oncology. 14 (6): 685- 691.
Cooper, B. G. (2015). Home Oxygen and Domestic Fires. Lung Function and Sleep. 11 (1): 1-11.
McCarthy, J., Bossarte, R., Katz, R.I., Thompson, C., Kemp, J., Hannemann, C., Nelson, C. & Schoenbaum, M. (2015). Predictive Modeling and Concentration of the Risk of Suicide: Implications for Prevention Interventions in the US Department of Veteran Affairs. American Journal of Public Health. 105 (9):
Stoelb, M. & Chiriboga, J. (1998). A Process for Assessing Adolescent risk for suicide. Journal of Adolescence. 21 359-370.
We can write this or a similar paper for you! Simply fill the order form!
Bipolar Disorder and Young Adults Order Instructions: Topic: Bipolar Disorder and Young Adults
Scenario: A 19-year-old college student has been admitted to the Mental Health Unit with a new diagnosis of Bipolar Disorder.
Bipolar Disorder and Young Adults
During a meeting, the family asks what caused this problem, since nobody else in the family has the disorder. The family says that they do not want their relative “drugged up” by being given psychiatric medications since they have heard negative reports about side effects of these medications.
After reading the following textbook pages listed below, address the following & Answer the following questions:
1-Based on your readings and knowledge, discuss what the RN would teach the client and family about Bipolar Disorder.
2-Would the RN need to make any adjustments in the teaching based on this client’s patient’s age? If so, explain.
3-Discuss how the RN would respond to the family’s desire not to have the client take any medication.
Requirements & Attention to the writer, Make sure the following is accomplished with this paper:
1-Please focus on answering the questions and supporting your answers with the evidence.
2-Once you have thoroughly completed this objective expand on the subject a little
3-Please support the intervention directly.
4- APA style
5-1 pages long 275 words Minimum or more.
6- Provide 2 citations, one from either textbook listed below.
Thanks for your attention to the requirements and details. Questions let me know.
Bipolar Disorder and Young Adults Required Materials
Textbooks (Chapter numbers and titles may differ in subsequent editions of a given textbook. If your edition is different, use the Table of Contents in the textbook to locate the appropriate chapters to read):
Kee, J., Hayes, E., & McCuistion, L. (2015). Pharmacology: A nursing process approach (8th ed.). Philadelphia, PA: Elsevier.
Nursing Diagnosis Guidebook – A pocket-size nursing diagnosis guidebook of your choice that is no more than one edition old, that includes NANDA International-approved nursing diagnoses, definitions, defining characteristics, and possible nursing Interventions.
Pillitteri, A. (2014). Maternal and Child Health Nursing (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Townsend, M.C. (2015). Psychiatric Mental Health Nursing: Concepts of Care in Evidence-Based Practice (8th ed.). Philadelphia, PA: F.A. Davis Company.
Required: Textbooks and chapters to focus on:
Pharmacology**
• Chapter 20: Central Nervous System Stimulants
• Chapter 27: Antipsychotics and Anxiolytics
• Chapter 28: Antidepressants and Mood Stabilizers
Nursing Diagnosis
• Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Maternal and Child Health Nursing**
• Chapter 54: Nursing Care of a Family When a Child Has a Cognitive or Mental Health Disorder
Psychiatric Mental Health Nursing**
• Chapter 13: Crisis Intervention
• Chapter 17: The Suicidal Client
• Chapter 20: Electroconvulsive Therapy
• Chapter 25: Depressive Disorders
• Chapter 26: Bipolar and Related Disorders
Web-Based and Other Professional Resources:
• Suicide assessment and nurses: What does the evidence show? (2015)**
• Care of the suicidal pediatric patient in the ED: a case study (2011)**
Bipolar Disorder and Young Adults Sample Answer
BIPOLAR DISORDER AND YOUNG ADULTS
Bipolar disorder is a brain disorder also known as the manic-depressive illness that causes the shifts in ability, moods and activity levels. The RN makes the positive contributions to the patients and their families through teaching about physical care, psycho-education and relapse prevention. The RN develops knowledge of the bipolar disorder (Kee et al, 2015). The RN teaches the patient common signs and symptoms of the disorder as well as the treatment options available for managing the conditions effectively. The patient and the family are educated on the risk factors that lead to the disorder. The education makes them aware of other risk factors such as brain structure and functioning apart from family history and genetics which are the main factors they understand to cause the bipolar disorder (Townsend, 2015). The psychotherapy is also taught by RN, which is a combination of talk therapy and medication. The education essentially guides the patients and families living with the disorder (Kee et al, 2015). Adjustment during the teaching process of the patients and families about the bipolar disorder is essential where the factor is considered. The patients should be educated that the disorders occur with a growing frequency among the young ages thus it is vital for young people e.g. the 19 years old college student to ensure they keep a life chart as they are vulnerable to suffer from bipolar disorder. The young people e.g. the student in the case study have a tendency to develop the disease which also involves the environmental factors.
It is important for the RN to respond appropriately to the family of the patient on the matter of medication. Awareness of the importance of the medication shall be enhanced among the family and the patient by highlighting the treatment options and therapies available for the disorder (Kee et al, 2015). The RN also notifies the family about the type of bipolar disorder management that works best for the particular patient. If the family are totally against the medications and drugs used by bipolar disorder patients, Electroconvulsive Therapy (ECT) can be suggested to them as they consider taking other medications risky (Townsend, 2015). The primary responsibility of the RN is to ensure the patient and his family see the positive side and impact of the treatment rather than the few side effects that result after medication (Kee et al, 2015).
Bipolar Disorder and Young Adults Reference
Kee, J., Hayes, E., & McCuistion, L. (2015). Pharmacology: A nursing process approach (8th ed.). Philadelphia, PA: Elsevier.
Townsend, M.C. (2015). Psychiatric Mental Health Nursing: Concepts of Care in Evidence-Based Practice (8th ed.). Philadelphia, PA: F.A. Davis Company
Healthcare and Evidence Based Practice Capstone Paper Order Instructions:
Healthcare and Evidence Based Practice Capstone Paper
Combine all elements completed in previous weeks (Topics 1-4) into one cohesive evidence-based proposal and share the proposal with a leader in your organization. (Appropriate individuals include unit managers, department directors, clinical supervisors, charge nurses, and clinical educators.)
Obtain feedback from the leader you have selected and request verification using the Capstone Review Form. Submit the signed Capstone Review Form to
RNBSNclientcare@gcu.edu.
For information on how to complete the assignment, refer to “Writing Guidelines” and the “Exemplar of Evidence-Based Practice Capstone Paper.”
Include a title page, abstract, problem statement, conclusion, reference section, and appendices (if tables, graphs, surveys, diagrams, etc. are created from tools required in Topic 4).
Prepare this assignment according to the APA guidelines found in the APA Style Guide, located in the Student Success Center.
This assignment uses a rubric. Please review the rubric prior to beginning the assignment to become familiar with the expectations for successful completion.
You are required to submit this assignment to Turnitin. Please refer to the directions in the Student Success Center.
Note: All Capstone Projects are to be submitted to the College. Please submit the Capstone Project Copyright and Distribution Form as well as an electronic copy of the Capstone Project itself to this e-mail address: CapstoneRNBSN@gcu.edu
Constructing the Written Evidence-Based Proposal: Final
1
Unsatisfactory 0-72%
0.00%
2
Less Than Satisfactory 72-75%
75.00%
3
Satisfactory 76-79%
79.00%
4
Good 80-89%
89.00%
5
Excellent 90-100%
100.00%
80.0 %Content
5.0 %Abstract
No abstract was provided.
The abstract was provided but was missing criteria as indicated in the writing guidelines.
Abstract meets all criteria of writing guidelines.
Abstract meets all criteria of writing guidelines in a detailed and comprehensive manner.
Abstract meets all criteria of writing guidelines in a detailed and comprehensive manner while demonstrating a deeper understanding by incorporating prior learning or thoughtful reflection.
10.0 %
Healthcare and Evidence Based Practice Capstone Paper Problem Description
No problem description was provided.
Problem description was provided but was missing criteria as indicated in the writing guidelines.
Problem description meets all criteria of writing guidelines.
Problem description meets all criteria of writing guidelines in a detailed and comprehensive manner.
Problem description meets all criteria of writing guidelines in a detailed and comprehensive manner while demonstrating a deeper understanding by incorporating prior learning or thoughtful reflection.
15.0 %Solution Description
No solution description was provided.
Solution description was provided but was missing criteria as indicated in the writing guidelines.
Solution description meets all criteria of writing guidelines.
Solution description meets all criteria of writing guidelines in a detailed and comprehensive manner.
Solution description meets all criteria of writing guidelines in a detailed and comprehensive manner while demonstrating a deeper understanding by incorporating prior learning or thoughtful reflection.
15.0 %Implementation Plan
Implementation plan abstract was provided.
The implementation plan was provided but was missing criteria as indicated in the writing guidelines.
Implementation plan meets all criteria of writing guidelines.
Implementation plan meets all criteria of writing guidelines in a detailed and comprehensive manner.
Implementation plan meets all criteria of writing guidelines in a detailed and comprehensive manner while demonstrating a deeper understanding by incorporating prior learning or thoughtful reflection.
15.0 %Evaluation Plan
No evaluation plan was provided.
The evaluation plan was provided but was missing criteria as indicated in the writing guidelines.
Evaluation plant meets all criteria of writing guidelines.
Evaluation plan meets all criteria of writing guidelines in a detailed and comprehensive manner.
Evaluation plan meets all criteria of writing guidelines in a detailed and comprehensive manner while demonstrating a deeper understanding by incorporating prior learning or thoughtful reflection.
10.0 %Dissemination Plan
No dissemination plan was provided.
Dissemination plan was provided but was missing criteria as indicated in the writing guidelines.
Dissemination plan meets all criteria of writing guidelines.
Dissemination plan meets all criteria of writing guidelines in a detailed and comprehensive manner.
Dissemination plan meets all criteria of writing guidelines in a detailed and comprehensive manner while demonstrating a deeper understanding by incorporating prior learning or thoughtful reflection.
15.0 %Organization and Effectiveness
7.0 %Thesis Development and Purpose
Paper lacks any discernible overall purpose or organizing claim.
Thesis/ main claim is insufficiently developed and/or vague; the purpose is not clear.
Thesis/main claim is apparent and appropriate to the purpose.
Thesis/ main claim is clear and forecasts the development of the paper. It is descriptive and reflective of the arguments, and appropriate to the purpose.
Thesis/ main claim is comprehensive. The essence of the paper is contained within the thesis. Thesis statement makes the purpose of the paper clear.
8.0 %Argument Logic and Construction
Statement of purpose is not justified by the conclusion. The conclusion does not support the claim made. An argument is incoherent and uses noncredible sources.
Sufficient justification of claims is lacking. The argument lacks consistent unity. There are obvious flaws in the logic. Some sources have questionable credibility.
The argument is orderly but may have a few inconsistencies. The argument presents a minimal justification of claims. Argument logically, but not thoroughly, supports the purpose. Sources used are credible. Introduction and conclusion bracket the thesis.
The argument shows logical progression. Techniques of argumentation are evident. There is a smooth progression of claims from the introduction to conclusion. Most sources are authoritative.
Clear and convincing argument presents a persuasive claim in a distinctive and compelling manner. All sources are authoritative.
5.0 %Mechanics of Writing (includes spelling, punctuation, grammar, language use)
Surface errors are pervasive enough that they impede communication of meaning. Inappropriate word choice and/or sentence construction are used.
Frequent and repetitive mechanical errors distract the reader. Inconsistencies in language choice (register), sentence structure, and/or word choice are present.
Some mechanical errors or typos are present but are not overly distracting to the reader. Correct sentence structure and audience-appropriate language are used.
The prose is largely free of mechanical errors, although a few may be present. A variety of sentence structures and effective figures of speech are used.
The writer is clearly in command of standard, written, academic English.
5.0 %Format
5.0 %Paper Format (Use of appropriate style for the major and assignment)
The template is not used appropriately, or documentation format is rarely followed correctly.
Appropriate template is used, but some elements are missing or mistaken. A lack of control with formatting is apparent.
Appropriate template is used. Formatting is correct, although some minor errors may be present.
Appropriate template is fully used. There are virtually no errors in formatting style.
All format elements are correct.
5.0 %Research Citations (In-text citations for paraphrasing and direct quotes, and reference page listing and formatting, as appropriate to assignment and style)
No reference page is included. No citations are used.
The reference page is present. Citations are inconsistently used.
The reference page is included and lists sources used in the paper. Sources are appropriately documented, although some errors may be present
The reference page is present and fully inclusive of all cited sources. Documentation is appropriate and citation style is usually correct.
In-text citations and a reference page are complete and correct. The documentation of cited sources is free of error.
100 %Total Weightage
Cancel
Healthcare and Evidence Based Practice Capstone Paper Sample Answer
Student’s Name
Institutional Affiliation
Abstract
The quality of health care offered in a medical institution dictates the speed of recovery of the patient, and consequently, the level of patient satisfaction. Since patient care involves a series of medical interventions by different personnel, communication is vital in ensuring efficient service delivery. Nurses especially have close contact with the patients than a majority of other medical staff. Therefore a good interpersonal relationship should be nurtured between them, to enable pthe assing of information from the patient top the medical staff, and vice versa. Nurses hence form a vital link for relaying of information. Communication systems should be available to allow for the passing of this information. Nurses too should have excellent communication skills to facilitate receiving, processing, and pass of information. Over the years these channels and abilities of nurses to communicate effectively have been noted to exist, resulting in communication breakdown, and poor quality of health care.
This paper discusses the problem of poor communication and how this has contributed to the poor delivery of services, offering a possible means of intervention to the issue.
Healthcare and Evidence Based Practice Capstone Paper Problem Description
The lack of proper communication and active channels of disseminating information has been a major concern to the nursing community (Kourkouta & Papathaniasiou, 2014). Inefficient communication channels have led to poor quality of service to the patients and consequently patient dissatisfaction. Lack of a clear defined communication system between nurses and other medical professionals, and to patients has led to a reduction in the quality of health care offered in medical institutions in the United States. Identification of the gap has led to intervention by various stakeholders in the industry in a bid to rectify the problem and improve the quality of health care.
Physicians rely on information provided by the nurses. In a strained communication relations between these parties can be fatal, as incorrect information can be passed.
Healthcare and Evidence Based Practice Capstone Paper Solution Description
Strategies have to be initiated by the nursing fraternity to facilitate for the disjointed communication between nurses, other medical practitioners, and the patients. Efficient interpersonal communication amongst them will facilitate for this extensive communication network. The strategies set by a combined body of nurses, and incorporating other medical professionals will alleviate existing pressure between the involved parties. Better communication between the various medical personnel will result in better services coordination, and consequently, better services will be offered to the patient (Lombardo, 2013).
Enactment of relevant policies and close monitoring to ensure they are adequately followed will eliminate the barriers of communication. Policies facilitating for a patient-centred service delivery go a long way in improving the nurse- patient relationship and accordingly, better communication.
Healthcare and Evidence Based Practice Capstone Paper Literature Review
Communication in the healthcare industry is critical. Information obtained from a patient is passed over from one personnel to another. Therefore proper flow of this information should be maintained for the provision of quality health care to patients. Lack of good communication systems between the various groups of health care personnel has hindered this, resulting in an inadequate health care service. A medical institution offering substandard care leads to patient dissatisfaction and increased mortality rates may be reported.
Enacting of proper policies dictating the design of communication and interaction will reduce instances of communication breakdown in the sector. The nursing fraternity lacks the appropriate mechanisms for promoting better health care services. Nurse training programs, both pre-service and in-service, do not emphasize on installing strong communication skills to the trainees. The ignorance is subsequently passed on into the work field.
Despite the nation devising measures for improving provider-patient interaction and communication, no significant change has been noted. This, therefore, calls for the need to design further steps to achieve success. The nursing body, in collaboration with trainers, should develop ways to instil the desired patient interaction and communication skills early, most preferably during training.
Bizarre instances have been reported to occur due to lack of enactment of proper communication. Various inefficiencies have been attributed to a breakdown in communication. These include; medical errors, lack of or inadequate treatment and rising of additional, unnecessary costs have been caused by the breakdown in communication. These errors underline the necessity of devising proper communication systems to avoid similar misgivings. The nurse on duty, for example, may end up administering wrong medication to the patient due to misinformation.
Improper coordination by different bodies of the nursing bodies is attributed to inefficiencies in meeting the bio-psychological needs of the patients. Oral communication is considered a fundamental aspect of the achievement of the well-being of the patient. This is not available in the nurse-patient interaction, making the achievement of quality health care unattainable. As nurses are unable to express their sincerity and commitment towards the betterment of the patient’s health, doubt is set in the mind-set of the patient on the willingness of the healthcare provider intention to help. Nurses’ failure to communicate with each other properly also led to inadequate patient care. Lack of understanding amongst the team may result in the passing of contradicting information by the nurses to the patient, and possibly undermine the overall safety of the patient.
The nursing profession is a delicate sector and a pillar of the health care system. Mismatch in relaying of information may lead to adverse effects to the patient, including the possibility of death. Families and friends of the patients are also affected when information does not flow properly (Unluturk, M. S., Ozcanhan, & Dalkilic, 2015). Misrepresentation of the patients’ progress results may occur due to errors in relaying of information by the health care providers.
Patients over time become irritated by the unacceptable mistakes caused by the breakdown in communication. However, the inefficient communication systems and other barriers of nurse-patient communication bar the patient from notifying the health care personnel, worsening the condition. In collaboration with other factors, this may lead to reduced recovery speed of the patient, bringing prolonged stay and additional expenses.
The setting of appropriate strategies for the involved parties to provide for efficient relaying of information significantly improves the quality of health care. If the plan is keenly followed, cases of errors of assumption will be reduced, resulting in better service delivery. Patient satisfaction in the short and long run will be achieved as a consequence of a free flow of information, ideas and suggestions to, and from the patients.
Coordination between all stakeholders is vital for the achievement of a complete, efficient running of the health care industry. The nurses should also ensure a proper system of communication with physicians and other medical professionals is established. A favourable working relationship which is essential for the optimum performance of personnel will thrive in this environment, consequently resulting in better care.
Healthcare and Evidence Based Practice Capstone Paper and Implementation Plan
Evaluation method helps in identifying the objectives and manner in which a particular data had been evaluated .collected and analysed. When having a defined project evaluation plan will guide the activities and will ensure there are best service and success in the project. The assessment plan is paramount for the quality delivery of Medicare to patients by nurses and doctors. There have been problems in the health sector on the provision of the healthcare which affects the patients who are the recipient of Medicare. Because of that problem I have been forced to give a proposal for a project which will cater for the patient’s welfare since they are the ones targeted. The only solution is to have a patient-centred Medicare which will reduce all the problems which have been there for mortality rate and the readmission because of the relapse of the problems.
The patient –centred Medicare will take the services close to the patients, and there will be an observation by the head of centres to ensure it is efficient and satisfying to family members. Readmission rate is the challenging issue which would be solved by the proposal. Before the implementation of the plan, there has been lengthy hospitalization of patients which led to high cost of Medicare. Readmission has caused the patient’s speed a lot of money and in return get inadequate healthcare. To do away with all those challenges the patient –centred Medicare will extend the medication even after discharge. This proposal has reduced the rate of readmission from 30% to 20% which shows the effectiveness. Patient –centred care is aiming to lower the cost of healthcare and the pattern of admission among patients.
Evaluation plan for Healthcare and Evidence Based Practice Capstone Paper
There have been many cases of poor medication which lead to the death of the patients, and the issue has raised an alarm. The biggest problem has been the communication where the doctors fail to involve the patients in the progress of their Medicare (Grol, Wensing, Eccles, & Davis, 2013). The patients have little or no information about how they are doing and that make it difficult for them to recover from illnesses. By employing the patient-centred heal care, the mortality rates will reduce because the patients will be involved in the decision-making. The research shows that the satisfaction level has risen to over 50% after initiating the change.
The variables of assessing the project are the mortality rates among patients and reduction off the injuries which give the proposal credit. The patients will have a short stay in the hospital and the rate of readmission still can useful in evaluating the project. The families of the patient still can be used to assess the project because there will be lower medication cost and insurance.
The questionnaires will be tools used to evaluate the project outcome which will be filled by the nurses and practitioners. The survey will also be conducted in different hospitals which will be followed by seminars and training sessions (Grol, Wensing, Eccles, & Davis, 2013).
Healthcare and Evidence Based Practice Capstone Paper and Disseminating Evidence
The main aim of every project is arguably the presentation and implementation of the resultant strategy (Mitton, Adair, & McKenzie, E., 2007). Information obtained from this study will be presented to health care stakeholders over a 3-month timeframe. Hospital CEO, NICU Nurse Manager, Director of Paediatrics, and other relevant officials will receive the publication to consider incorporating the strategy into the system. Conferences and workshops will be arranged in due course to ensure a high-profile implementation of the project. A two-way interactive process will be established allowing for feedback from the NICU to the project implementers on the implementation progress and any changes required. Publication of the plan in pamphlets and online sources will also help cover a wider audience, allowing for utilization of other health care facilities (Lomas, 2013).
Healthcare and Evidence Based Practice Capstone Paper References
Grol, R., Wensing, M., Eccles, M., & Davis, D. (2013). Improving patient care. John Wiley & Sons.
Kourkouta, L., & Papathaniasiou, I. (2014). Communication in nursing practice. Journal of the Academy of Medical Science, 26(1), 65-67.
Lomas, J. (2013). Diffusion, dissemination, and implementation: who should do what? Acad Science, 226-235.
Lombardo, C. (2013). Nursing’s role in achieving excellence in care delivery across the continuum of health for new mothers with hypertension. Journal of Obstetric, Gynecologic and Neonatal Nursing, 42.
Mitton, C., Adair, C., & McKenzie, E. (2007). Knowledge transfer and exchange: review and synthesis of the literature (Vol. 85). Milbank.
Unluturk, M. S., Ozcanhan, M., & Dalkilic, G. (2015). Improving communication among nurses and patients. Computer Methods and Programs in Biomedicine, 120(2), 102-112.
Care on Patient Diagnosed with Heart Failure Order Instructions: Review of the Literature
Care on Patient Diagnosed with Heart Failure Details:
Write a paper (1,500-2,000 words) in which you analyze and appraise each of the (15) articles identified in Topic 1. Pay particular attention to evidence that supports the problem, issue, or deficit, and your proposed solution.
Care on Patient Diagnosed with Heart Failure
Hint: The Topic 2 readings provide appraisal questions that will assist you to efficiently and effectively analyze each article.
Refer to “Sample Format for Review of Literature,” “RefWorks,” and “Topic 2: Checklist.”
Prepare this assignment according to the APA guidelines found in the APA Style Guide, located in the Student Success Center. An abstract is not required.
You are required to submit this assignment to Turnitin. Please refer to the directions in the Student Success Center.
3 NRS 441v.11R.Module 2_Checklist.doc
Care on Patient Diagnosed with Heart Failure Sample Answers
REVIEW OF LITERATURE
Name
Institution
Adib-Hajbaghery, M., Maghaminejad, F., & Ali, A. (2013). The Role of Continuous Care in Reducing Readmission for Patients with Heart Failure. J Caring Sci., 2(4), 255-267. http://dx.doi.org/10.5681/jcs.2013.031
This article explores the importance of continuous care among patient diagnosed with Heart Failure. According to this article, approximately 20-50% of geriatric patients diagnosed with CHF undergo readmission in 2 weeks -90 days after they have been discharged. This paper explores the impact of post-discharge care in reducing the re-hospitalization rates and in improving patient’s quality of life. The research study is a systematic review, which was conducted to evaluate on studies that have been conducted on CHF follow up care post discharge or patients who had been readmitted. The studies from Gthe google search Engine, SID and Iranmedex databases were evaluated.
The studies evaluated were those conducted from 1995-2013. A total of 21 trials were generated, 16 of which evaluated the impact on home visits, telephone monitoring and patient education before the discharge of patients. A quarter of the studies did not report any reduction on post discharge re-admissions of patients diagnosed with CHF. This paper concluded that the post discharge interventions developed by nurses can considerably reduce the rates of readmissions. Considering the inadequacy of health care resources, using patient education combination method is an effective strategy that can be used to reduce the readmissions incidences among the geriatric population. This article will helps in building up my literature review by providing useful information on the effect of patient education using teach back method among the geriatric population diagnosed with CHF.
Black, J., Romano, P., Sadeghi, B., Auerbach, A., Ganiats, T., & Greenfield, S. et al. (2014). A remote monitoring and telephone nurse coaching intervention to reduce readmissions among patients with heart failure: study protocol for the Better Effectiveness After Transition – Heart Failure (BEAT-HF) randomized controlled trial. Trials, 15(1), 124. http://dx.doi.org/10.1186/1745-6215-15-124
CHF is a public health issue which is associated with costly hospitalization. According to evidence based research, transitional care programs do reduce readmission rates. However, the implementations of these transition care programs are faced by various barriers such as financial limitation and inadequate training. The aim of these randomized controlled studies is to evaluate on the impact of these transition care programs of the population which includes establishing interventions such as pre-education of a patient before and after their discharge, and telephone monitoring care as well as telephone nurse coaching. The study methodology is a randomized control study. A total of 1500 participants were used. The participants were above 50 years old and with a history of CHF. The study population was also from a diverse population background. The study reported a significant reduction on hospital readmission and increase in self management among the geriatric population diagnosed with CHF. This paper provides a rich source of information on the best strategies that can be used to improve patient transition care using remote technology as possible.
Chen J, Ross JS, Carlson MD, Lin Z, Normand SL, Bernheim SM. et al. (2012). Skilled nursing facility referral and hospital readmission rate after heart failure or myocardial infarction. Am J Med. 125(1):100. e1–9.
There has been a substantial increase on the number of hospital readmissions of patients diagnosed with CHF. There have been a considerable number of state-level variations in the discharge of skilled nursing facilities. However, there is limited information on hospital level variation of SNF rates and its association with increased re-admission rates. This quantitative research studies was conducted by evaluating the data obtained from fee charges of Medicare patients who had a principal diagnosis of CHF. The study indicated that a shortage of skilled nurses resulted to an increase in readmission rates. However, the article did not explain on the causes of readmission rates.
Dominque, FBI., Aliti, G., Dominguez, D., Rabelo, E., & Clausell, N. (2011). Education and telephone monitoring by nurses of patients with heart failure: a randomized clinical trial. Arq Bras Cardiol., 9(3), 233-239. http://dx.doi.org/Epub 2011 Feb 4.
Studies on nursing interventions in patients diagnosed with CHF reports reduced morbidity and mortality rates. However, there is limited information on intra-hospital education and telephone coaching. This comparative study compared two groups of patients hospitalized with CHF. The intervention group received patient education during hospitalization, which was followed by telephone monitoring and coaching after discharge. The control group only received training during hospitalizations. The patient evaluated the following outcomes including self care knowledge, the levels of CHF, re-admissions rates and the number of emergency visits. The study findings reported a 29% decrease in a number of readmission among the intervention group. This indicated that in-hospital educational nursing intervention benefited the CHF patients by making them understand their disease and effective self management care.
Feltner, C., Jones, C., Cené, C., Zheng, Z., Sueta, C., & Coker-Schwimmer, E. et al. (2014). Transitional Care Interventions to Prevent Readmissions for Persons With Heart Failure. Annals Of Internal Medicine, 160(11), 774. http://dx.doi.org/10.7326/m14-0083
Approximately 25% of the geriatric populations hospitalized with CHF are hospitalized within the first days after discharge. The aim of this study is to assess the comparative effectiveness and challenges of transitional care in the reduction of readmission rates as well as the mortality rates. The paper conducted a systematic review from the CINAHL, MEDLINE, Cochrane library and WHO registry. A total of 47 studies were identified. Most of the studies focused on the geriatric population. Some of the studies reported a 30 day readmission rates. About 65% of all the studies indicated that integration of multidisciplinary programs such as home visiting programs reduced the re-admission rated considerably. The paper recommended that the use of structured telephone support (SOE) and home visiting programs should be integrated in all clinics and by all providers who are seeking to implement the transitional care. This article is important for this capstone project as it will facilitate in the identification of programs that aid in the reduction of the readmission rates.
Gruneir A, Dhalla IA, van Walraven C, Fischer HD, Camacho X, Rochon PA. et al. (2011). Unplanned readmissions after hospital discharge among patients identified as being at high risk for readmission using a validated predictive algorithm. Open Med.;5(2):e104–11
The unplanned hospital readmissions are common among the geriatric population and are very expensive. These readmission rates are preventable if the appropriate strategies of patient education and improvement of self management programs are integrated in the clinics. The aim of this study is to identify geriatric patients at risk of readmission using an alogarithm (LACE index). This aims at evaluating of the index is effective in identifying patients who are at high risk of getting readmissions and to identify the factors that puts the patient at risk, and ways to address these challenges. The study concluded that the use of the LACE index score of 10 is effective in identifying patients who are at high risk, and those who can benefit to maximum after post discharge. Therefore, this is a useful tool that can be used by the healthcare providers to identify patients who would need the integration of the post-discharge interventions.
Hasan O, Meltzer DO, Shaykevich SA, Bell CM, Kaboli PJ, Auerbach AD. et al. (2010). Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. ;25(3):211–9.
The study conducted to evaluate the effectiveness of training the CHF patient’s family members so that they can support and provide patient home care in order to improve patient’s quality of life and to reduce the readmission rates of patients diagnosed with CHF. This single blinded randomized control study enrolled participants through random sampling. The participants were divided into two groups, the control group and the intervention group. The intervention group had training during and after hospitalization. The study findings indicate that the mean score of the patient’s quality of life reduced in the control group as compared with the intervention at a period of six months. The study concluded that nursing follow up care of CHF geriatric patients improved their quality of life.
Hasanpour-Dehkordi, A., Khaledi-Far, A., Khaledi-Far, B., & Salehi-Tali, S. (2016). The effect of family training and support on the quality of life and cost of hospital readmissions in congestive heart failure patients in Iran. Applied Nursing Research, 31, 165-169. http://dx.doi.org/10.1016/j.apnr.2016.03.005
This paper explores the early indicators patient readmission by using a complex prediction model. The study design is a prospective observation of the population, which involved 10, 496 participants. The study evaluated the number of readmission after 30 days, and grouped the factors into four categories including the health condition, social support, health utilization and socio-demographic factors. After performing a regression study, seven main factors were identified including the patient insurance status, regular physicians and the patient’s marital status. The study indicated that the nurses can utilize the prediction model effectively to identify risk factors for readmission, and use the findings to develop an education plan that targets the patient’s individual needs and challenges. This will help establish the efficient interventions that will help reduce the readmission rates.
Inglis, S., Clark, R., Dierckx, R., Prieto-Merino, D., & Cleland, J. (2015). Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Of Systematic Reviews. http://dx.doi.org/10.1002/14651858.cd007228.pub3
Specialized management of CHF involves the improvement of care and clinical outcomes as well as healthcare utilization. This paper reviews the effect of structured telephone support in a combination of non invasive home telemonitoring on CHF patients care and in comparison of the usual standard of care. The study reported a 55. 1% of the patients under the specialized management improved their medication adherence. This reduced the patient’s risk of all because of mortality as well as the heart related disorders. The interventions indicated significant improvements on the patient’s quality of life as well as the heart failure knowledge as well as self care behavior.
Inglis, S., Clark, R., McAlister, F., Stewart, S., & Cleland, J. (2011). Which components of heart failure programmes are effective? A systematic review and meta-analysis of the outcomes of structured telephone support or telemonitoring as the primary component of chronic heart failure management in 8323 patients: Abridged Coc. European Journal Of Heart Failure, 13(9), 1028-1040. http://dx.doi.org/10.1093/eurjhf/hfr039
Several clinical studies indicates that use of structured telephone support (STS) and telemonitoring have a high potential of helping the nursed to deliver specialized management to patients diagnosed with CHF. However, the efficacy of telemonitoring and STS has not been established. This meta-analysis paper evaluated the existing the randomized control trails (RCTs) by comparing the TM and STS interventions to usual care interventions. The study findings found that the interventions improved the patient’s quality of life, and reduced their costs significantly. The study concluded that key strategies in the reduction of patient readmission rates are by making improvements on patient self care, patient knowledge and improve the patient, functional class.
Kitsiou, S., Paré, G., & Jaana, M. (2015). Effects of Home Telemonitoring Interventions on Patients With Chronic Heart Failure: An Overview of Systematic Reviews. J Med Internet Res, 17(3), e63. http://dx.doi.org/10.2196/jmir.4174
The article explores the impact of post discharge patient education care using telemonitoring and coaching of patients diagnosed with CHF. This systematic review conducted a comprehensive literature search where a total of 15 reviews were published. The studies indicated a 1.4-6.5% risk reduction of all causing mortality and readmission rates. The study concluded that future studies should explore the home monitoring to identify more optimal strategies that it confers effective self management strategies.
Navidian, A., Yaghoubinia, F., Ganjali, A., & Khoshsimaee, S. (2015). The Effect of Self-Care Education on the Awareness, Attitude, and Adherence to Self-Care Behaviors in Hospitalized Patients Due to Heart Failure with and without Depression. PLOS ONE, 10(6), e0130973. http://dx.doi.org/10.1371/journal.pone.0130973
The exacerbation of CHF is influenced by factors such as the psychological factors and other health disorders associated with old age. This paper evaluates the impact of self care education on patient’s adherence, attitude and awareness of CHF patients who are hospitalized. The study findings found those intervention groups have improved scores on patient attitude, awareness and adherence as compared to control groups.
Pandor, A., Thokala, P., Gomersall, T., Baalbaki, H., Stevens, J., & Wang, J. et al. (2013). Home telemonitoring or structured telephone support programmes after recent discharge in patients with heart failure: a systematic review and economic evaluation. Health Technol Assess, 17(32). http://dx.doi.org/10.3310/hta17320
The readmission rates for CHF patients are common among the geriatric population. Research indicates that the integration of remote monitoring and patient education have a potential to deliver effective and specialized care, one that will meet the growing demands for the CHF needs for the geriatric population. Some of the challenges identifies by this study is that there is no a care package such as protocols on communication, staff visits or other resources. This indicated that there are still uncertainties about the effectives of Home monitoring in terms of management of CHF patients. However, the study generalized that where standard care is less good, then, home monitoring strategy should be used.
White, M., Garbez, R., Carroll, M., Brinker, E., & Howie-Esquivel, J. (2013). Is “Teach-Back” Associated With Knowledge Retention and Hospital Readmission in Hospitalized Heart Failure Patients?. The Journal Of Cardiovascular Nursing, 28(2), 137-146. http://dx.doi.org/10.1097/jcn.0b013e31824987bd
CHF is a chronic disease that affects approximately 5.8 million people in the USA. In addition, a further 670,000 are diagnosed with CHF annually, The large fraction of the people diagnosed with CHF are geriatric population. The average readmission days are within 30 days after hospital discharge. Despite the guidelines established on the importance of patient education to avoid readmissions, the most effective strategy of education is still unknown. The aim of the paper is to explore if the teach back method of patient education aids in the reduction of readmission rates. This prospective cohort study found that teach back method of education reduced readmission rates by 8.4 %. The study concluded that the teach back method is an effective teaching method as it helps the patients retain the information for a significantly longer time than patients who had been taught using briefer teaching.
Vedel, I. & Khanassov, V. (2015). Transitional Care for Patients With Congestive Heart Failure: A Systematic Review and Meta-Analysis. The Annals Of Family Medicine, 13(6), 562-571. http://dx.doi.org/10.1370/afm.1844
The paper is a meta-analysis paper conducted to determine the effect of transitional care interventions on the patients diagnosed with CHF. A systematic review was conducted on the following databases including the Medline, EMBASE, Psychinfo and Cochrane. A total of 41 randomized control studies were identified, The study indicated that the integration of Transitional care reduced the readmission rayed by 8-29%. The paper concludes that high intensive training which involves the combination of telephone coaching, telephone follow up and clinical visits reduced readmission risk effectively. Therefore, it is highly recommended that that the healthcare providers should integrate these interventions in their healthcare facility.
Care on Patient Diagnosed with Heart Failure References
Adib-Hajbaghery, M., Maghaminejad, F., & Ali, A. (2013). The Role of Continuous Care in Reducing Readmission for Patients with Heart Failure. J Caring Sci., 2(4), 255-267. Retrieved from http://dx.doi.org/10.5681/jcs.2013.031
Black, J., Romano, P., Sadeghi, B., Auerbach, A., Ganiats, T., & Greenfield, S. et al. (2014). A remote monitoring and telephone nurse coaching intervention to reduce readmissions among patients with heart failure: study protocol for the Better Effectiveness After Transition – Heart Failure (BEAT-HF) randomized controlled trial. Trials, 15(1), 124. Retrieved from http://dx.doi.org/10.1186/1745-6215-15-124
Chen J, Ross JS, Carlson MD, Lin Z, Normand SL, Bernheim SM. et al. (2012). Skilled nursing facility referral and hospital readmission rate after heart failure or myocardial infarction. Am J Med. 125(1):100. e1–9.
Dominque, FBI., Aliti, G., Dominguez, D., Rabelo, E., & Clausell, N. (2011). Education and telephone monitoring by nurses of patients with heart failure: a randomized clinical trial. Arq Bras Cardiol., 9(3), 233-239. Retrieved from http://dx.doi.org/Epub 2011 Feb 4.
Feltner, C., Jones, C., Cené, C., Zheng, Z., Sueta, C., & Coker-Schwimmer, E. et al. (2014). Transitional Care Interventions to Prevent Readmissions for Persons With Heart Failure. Annals Of Internal Medicine, 160(11), 774. Retrieved from http://dx.doi.org/10.7326/m14-0083
Gruneir A, Dhalla IA, van Walraven C, Fischer HD, Camacho X, Rochon PA. et al. (2011). Unplanned readmissions after hospital discharge among patients identified as being at high risk for readmission using a validated predictive algorithm. Open Med. 5(2):e104–11
Hasan O, Meltzer DO, Shaykevich SA, Bell CM, Kaboli PJ, Auerbach AD. et al. (2010). Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 25(3):211–9.
Hasanpour-Dehkordi, A., Khaledi-Far, A., Khaledi-Far, B., & Salehi-Tali, S. (2016). The effect of family training and support on the quality of life and cost of hospital readmissions in congestive heart failure patients in Iran. Applied Nursing Research, 31, 165-169. Retrieved from http://dx.doi.org/10.1016/j.apnr.2016.03.005
Inglis, S., Clark, R., Dierckx, R., Prieto-Merino, D., & Cleland, J. (2015). Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Of Systematic Reviews. Retrieved from http://dx.doi.org/10.1002/14651858.cd007228.pub3
Inglis, S., Clark, R., McAlister, F., Stewart, S., & Cleland, J. (2011). Which components of heart failure programmes are effective? A systematic review and meta-analysis of the outcomes of structured telephone support or telemonitoring as the primary component of chronic heart failure management in 8323 patients: Abridged Coc. European Journal Of Heart Failure, 13(9), 1028-1040. Retrieved from http://dx.doi.org/10.1093/eurjhf/hfr039
Kitsiou, S., Paré, G., & Jaana, M. (2015). Effects of Home Telemonitoring Interventions on Patients With Chronic Heart Failure: An Overview of Systematic Reviews. J Med Internet Res, 17(3), e63. Retrieved from http://dx.doi.org/10.2196/jmir.4174
Navidian, A., Yaghoubinia, F., Ganjali, A., & Khoshsimaee, S. (2015). The Effect of Self-Care Education on the Awareness, Attitude, and Adherence to Self-Care Behaviors in Hospitalized Patients Due to Heart Failure with and without Depression. PLOS ONE, 10(6), e0130973. Retrieved from http://dx.doi.org/10.1371/journal.pone.0130973
Pandor, A., Thokala, P., Gomersall, T., Baalbaki, H., Stevens, J., & Wang, J. et al. (2013). Home telemonitoring or structured telephone support programmes after recent discharge in patients with heart failure: a systematic review and economic evaluation. Health Technol Assess, 17(32). Retrieved from http://dx.doi.org/10.3310/hta17320
White, M., Garbez, R., Carroll, M., Brinker, E., & Howie-Esquivel, J. (2013). Is “Teach-Back” Associated With Knowledge Retention and Hospital Readmission in Hospitalized Heart Failure Patients?. The Journal Of Cardiovascular Nursing, 28(2), 137-146. Retrieved from http://dx.doi.org/10.1097/jcn.0b013e31824987bd
Vedel, I. & Khanassov, V. (2015). Transitional Care for Patients With Congestive Heart Failure: A Systematic Review and Meta-Analysis. The Annals Of Family Medicine, 13(6), 562-571. Retrieved from http://dx.doi.org/10.1370/afm.1844
Healthcare Policy Presentation by Governments and Order Instructions: How has it been presented by governments and by NGOs?
Healthcare Policy Presentation by Governments
What policy responses and services have been provided to deal with this problem? Are there other ways of responding to the problem?
Healthcare Policy Presentation by Governments and Sample Answer
How Healthcare Policy has been presented by Governments and NGOs
Health care policy is a term that is used to describe the plans, decisions and the actions that are undertaken in achieving specific healthcare objectives within a community. The World Health Organization (WHO) confirms that the development of an explicit health care policy facilitates the achievement of several things like defining a vision, outlining the priorities and the anticipate functions being played by diverse teams of individuals and informing people and building of consensus (Paolucci, 2010, pg. 33-46). Various categories of the policies in the healthcare sector exist including the individual health system, the pharmaceutical health system, and the other public health policies like breastfeeding promotion, control of tobacco, and the vaccination policy (Gani, 2008, pg. 72-81). These plans may cover the topics of delivery of healthcare, health equity, financing and access to care. There are many disciplines in politics and evidence influencing the decision making by the government or the NGOs in adopting a particular healthcare policy.
According to Klančar and Švab (2014, pg. 166-172), the modern concept of the healthcare system comprises of the access to the health professionals from different categories and the health technology in use as the equipment of surgery. Also, it includes access to the current evidence and information obtained from research such as healthcare services and medical research. In most of the government and NGOs, it is left to a person to get an access of the healthcare products through paying them from their own source of income and to the NGOs operators in the pharmaceutical and medical companies in developing the research. The production and making plans of the human resources concerning health get dispersed among the players of the market.
Many governments and the non-governmental organizations are integrating the philosophy of human rights in directing healthcare policies. The WHO has the report that for every nation in the world conform to at least one of the agreements of the human rights that play the role of addressing the rights which are related to health such as the right to health, and those reasons that relate to situations requiring better health. The NGO of the UNUDHR reports that all people have a right to health care (Siciliani, Moran & Borowitz, 2014, pg. 292-303).
Some of the faith-based NGOs, the perceived obligation which is shaped by the beliefs of a religion in catering for those unfavorable circumstances like the sick influences the health care policies. Other governments and the NGOs depend on the humanist principles in clarifying the policies of health, stating the enshrined right to health and the perceived obligation. The Amnesty International in the recent years has channeled its focus on health as a human right, finding solutions to the inadequate access to the HIV and AIDS drugs the rights of the women’s sexual and reproduction comprising of the differences in the maternal mortality within and across nations (Smullen & Hong, 2015, pg. 347-355).
There is a considerable controversy that remains regarding the policies on who would take the role of paying the health care costs for all individuals. For instance, the expenditure of the governments on healthcare is in particular cases applied as a global indicator of the commitment of the government towards the health of its citizens. Contrary, the United States rejects the notion financing the healthcare using the taxpayer’s money as being incompatible with the right of the professional judgment of the physician and other concerns that are related to the government involvement to oversee its citizen’s health (Groenewegen, P. et al., 2015, pg. 1576-1582). As a result, it could further lead to erosion of the privacy right between the patients and doctors. The statement urges that the healthcare insurance denies the patients’ right in disposing of their earnings according to their wish.
The other problem that arises in the healthcare policy debate on the problem the human right is the use of the legislation by the different governments in controlling competition among the national insurance systems and the private providers of the medical insurance such as the health insurance program for Canada. The Laissez-faire proponents have the argument this would erode the effectiveness of the cost of the health system since those having the capacity in paying for the private healthcare services draw the resources from the public. The problem here is whether the companies that are investor-owned or the other institutions of health maintenance have the capability in acting in the best interest of the consumers as compared to the oversight and regulation of the government. The other assertion by the US government is that the over-regulation insurance and healthcare industries by the government are perceived as the most appropriate end to the home visits by the doctors among those who are old and the have-nots.
Policy responses and services that have been provided in dealing with the Healthcare Policy
Changing of the administration can consequently lead to a change in the issues of policy. The presence of proper research in the healthcare does not bring about the policymaking that is evidence-based. For instance, in South Africa, whose population sets the record of the HIV cases, the policy of the former regime which was limiting the provision of funds for treatment of AIDS was met with arguments due to its denial in accepting the scientifically approved evidence on the method of the transmission of the disease. The change in the policy, therefore, brought out new policies being implemented for the widespread in accessing the services of HIV.
Most of the governments and NGOs are present including a health dimension in their foreign policies with the aim of achieving global health objectives. The promotion of health in the low income earning nations has been observed as being instrumental in achieving the other objectives on the comprehensive agenda. One of the agendas is the promotion of global security. The global security involves linking to the fears of the global pandemics, the potential increase in the conflicts of humanity, emergencies, the intentional spread of the pathogens and natural calamities. Secondly, promotion of the economic development which involves addressing of the economic effect of the poor health in the areas of development, gain from the ever-growing world market in the field of the health goods and services and the extreme outbreaks in the world market place. Finally, promotion of the social justice, the governments, and the non-governmental institutions are reinforcing health as a human right and a social value including the provision of support to the goals of the United Nation’s Millennium Development (Siciliani, Moran & Borowitz, 2014, pg. 289-296).
The government offers support to the legislation that has a focus speeding up the establishment of new and better treatments through encouraging the creation of drugs which treat conditions having less or no medical options (Paolucci, 2010, pg. 33-46). The term dormant therapy is used in referring to a new drug or a biological product determined to have inadequate patent protection and fulfills the unmet medical conditions, reduces risks as compared to the already existing treatment and improves the medical outcomes. Weak or no patent protection hinders the ability of the manufacturer in recouping the investment towards establishing the product and therefore, it is a disincentive for drug development. The current policies and regulations by the various governments and NGOs give encouragement to companies in pursuing the products having strongest patents, not necessarily products addressing the unmet medical requirements (Paolucci, 2010, pg. 33-46).
In dealing with the challenge of patient engagement, the governments of different countries are seeking the identification and implementation of the best actions for integrating the voice of the patient into the conduct of research and decision making of the healthcare. Most of the governments have undertaken initiatives of addressing the barriers to patient engagement by the multi-stakeholder framework through coming up with a consensus-based conceptual approach for patient engagement and agreement on the best actions in the development and research in the establishment of the drug. The governments and the NGOs have also established an information collection tool which performs the role of helping patient advocacy and organizations and organizing the concerns of the patient and gives a comment on the benefits and limitations of the treatment options. The tool is also designed in ensuring that the FDA captures reliable information that it needs from the patients, the patient advocates, and the family caregivers.
Working with the member organizations, most of the governments have been getting active on the major areas of policy during the implementation of the Affordable Care Act (ACA). The major areas that both the government and NGOs give priority are in ensuring that the health insurance policy plans meet the required standards that are the needs of individuals having chronic conditions and making reforms to the health care delivery system towards improving access to quality in the healthcare system. The governments and the NGOs are focused on the five top issues of making sure that the plans of insurance meet the required needs of patients including non-discrimination, continuity of care, transparency, enforcement of the patient protections and uniformity of the program materials (Siciliani, Moran & Borowitz, 2014, pg. 290-295). The implementation of the ACA would depend on as the regulators of the market of the insurance health. The support by the states is critical towards the guaranteeing of the ACA’s objectives of the affordable and quality care for the individuals. By the end of 2015, NHC in most of the states had established specific progress reports in assessing the patient-centeredness of the health insurance worldwide markets. The body also conducted national studies of the patient experience to enroll in the exchanges and relaunching a website designed to assist individuals to pick the right insurance plan that meets the budget and health needs including an out of pocket cost calculator.
In the provision of the real value in the healthcare system, there should be a confluence of the healthcare research and personal circumstances including the genetics of the patient, socio-economic status at the point of care, religion, and ethnicity. The combination of the healthcare research with the real-world application has facilitated improved health outcomes and would assist in curbing the costs in a responsible manner (Siciliani, Moran & Borowitz, 2014, pg. 298-303).
Anon (2011) asserts that the process of shopping for a given item like healthcare insurance, making choices can either be right or bad. But in case, one does not have all the necessary information concerning the issue, to perform an accurate side by side comparison of them, or the available information is not presented in a transparent manner to aid in an easy comparison, then the process of making the decision may become quite frustrating. If a consumer, therefore, picks a health insurance coverage that does not meet his or her budget and unique needs, the costs of the healthcare can go up (Anon, 2011, pg. 236-245).
The National Health Council of various countries has launched a system in form website composed of an interactive set of tools so as to assist the consumers in learning about the options for the health insurance. The site might be comprised of the resources on healthcare insurance, the marketplaces, and the place for numerous visitors for sharing their experiences on the health care and a health care cost estimator (Anon, 2011, pg. 231-235).
Other ways of responding to the problem include the development of the explicit policy in supporting and ensuring access to all the members of the state, funding the medical research and planning adequate distribution and the quality of the health workers in meeting the objectives of the healthcare (Lorenz, 2012, pg. 1-13). Many governments and NGOs around the world have developed a health system that is universal which is taking the burden of the expenses off of the individuals and businesses by pooling the financial risk. There are arguments arising for and against the health care and the related policies concerning the situation. Healthcare is, therefore, a vital section of the healthcare systems and as a result, it always has a contribution towards the greatest areas of expenditure both by the NGOs and government worldwide.
Healthcare Policy Presentation by Governments List of References
Anon, 2011. Public Long-term Care Financing Arrangements in OECD Countries. Help Wanted? OECD Health Policy Studies, pp.231–245.
Groenewegen, P. et al., 2015. Primary care practice composition in 34 countries. Health Policy, 119(12), pp.1576–1583.
Gani, A., 2008. Health care financing and health outcomes in Pacific Island countries. Health Policy and Planning, 24(1), pp.72–81.
Klančar, D. & Švab, I., 2014. Primary care principles and community health centers in the countries of former Yugoslavia. Health Policy, 118(2), pp.166–172.
Lorenz, C., 2012. Triangulating Health Expenditure Estimates from Different Data Sources in Developing Countries. Applied Health Economics and Health Policy, 10(1), pp.1–13.
Nolte, E. et al., 2008. Learning from other countries: an on-call facility for health care policy. Journal of Health Services Research & Policy, 13(suppl 2), pp.58–64.
Olsen, J.A., 2009. What makes the market for health care different? Principles in Health Economics and Policy, pp.47–60.
Paolucci, F., 2010. The Design of Health Care Financing Schemes in Different Countries. Developments in Health Economics and Public Policy Health Care Financing and Insurance, pp.33–46.
Siciliani, L., Moran, V. & Borowitz, M., 2014. Measuring and comparing health care waiting
times in OECD countries. Health Policy, 118(3), pp.292–303.
Smullen, A. & Hong, P.K., 2015. Comparing the Health Care Systems of High-Performing Asian Countries. Asia & the Pacific Policy Studies Asia and the Pacific Policy Studies, 2(2), pp.347–355.