W1 Clinical Assignment:
Define the Community at Risk
During your practicum you will use the follow guidelines to complete your final project and a community teaching project and paper.
Identify the target population Definition of the risk or problem and the significance ( e.g. teenage pregnancy, HIV, obesity).
The target population for this community teaching project will be all sexually active members of the community. This means that the married, divorced, separated and single adults as well as adolescents and commercial sex workers will be involved in this project. HIV knows not age, class, race, ethnicity, religion or even profession. It has the capability of infecting any sexually active individual who engages in irresponsible sexual behaviour with multiple partners. Information and awareness creation on HIV is therefore very essential for the young, the middle-aged and old members of the community (Crawford, Caldwell, Bush, Browning & Thornton, 2012).This population has been chosen because it is at the highest risk of being infected with HIV. The population will therefore be empowered with important information regarding HIV with the aim of reducing and eventually stopping new infections, caring for and treatment of those already living with the disease.
Definition of the problem
HIV has been a problem that has given medical researchers sleepless nights for so many years. It is indeed a great challenge for members of different communities given that up to date, there is no known cure for it. Everybody is at risk of HIV infection given that it is very difficult to tell whether one is infected or not unless a medical test is conducted. As for young people particular those going through there adolescence, the risk of infection is even greater because they lack adequate information on reproductive health and they are also likely to involve themselves in risky sexual behaviour due their strong peer influence. Adults who are married are not safe from HIV either. This is because a good number of married couples have been found to engage in extra marital affairs which have actually predisposed them to the risk of HIV infection. This means that HIV is silently spreading in marriages which were initially thought to be relatively safe. Infants have also not been left out due to the risk of mother to child transmission. Infection with HIV is not a barrier for women to get pregnant and therefore it would be important to educate expectant mother whether living with HIV or not on how they can protect their new born babies from acquiring this deadly virus (Sepúlveda, 2012). Another very common problem that relates to HIV in the community is stigmatisation of those who are living with the virus. Many HIV positive individuals have reportedly been living in fear or even hiding from other members of the society. This is a very serious problem that has also prevented them from accessing their medication which has led to further deterioration of their health.
Significance
This project will play a very crucial role not only to members of the community but also to the public health and nursing profession. Members of the community will be able to learn a lot pertaining to HIV and with such kind of information, new infections will have a significant decline if not a complete halt. This is because some new infections usually occur as a result of ignorance and the moment awareness is created among community members, such cases will definitely decrease. The project will also enable community members to learn about home-based care of people living with HIV since it is a chronic disease. It would also be important for people to be informed about the signs and symptoms of HIV so that they can seek early medical attention before the virus advances in their bodies. Most importantly, the project will be encouraging people to go for frequent voluntary counselling and testing for HIV so that can get to know their status and take appropriate action. Those who test positive for the virus will of course be counselled and prepared to start antiretroviral therapy where as those who test negative will be enlightened on how they can continue protecting themselves against the virus (Kuznetsov, Matterne, Crispin & Ruzicka, 2013).
References
Crawford, T., Caldwell, G., Bush, H. M., Browning, S., & Thornton, A. (2012), Foreign born status and HIV/AIDS: A comparative analysis of HIV/AIDS characteristics among foreign and U.S. born individuals. Journal of Immigrant and Minority Health, 14(1), 82-8. doi:http://dx.doi.org/10.1007/s10903-011-9455-8
Kuznetsov, L., Matterne, U., Crispin, A., Ruzicka, T., Zippel, S. A., & Kuznetsov, A. V. (2013), Knowledge, attitude and behavioral intention to act regarding HIV infection and prevention in immigrants from the former soviet union in Germany: A comparative study with the native population. Journal of Immigrant and Minority Health, 15(1), 68-77. doi:http://dx.doi.org/10.1007/s10903-012-9671-x
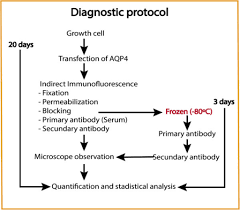
Protocol for Diagnosis, Management, and Follow-Up Care
Application: Protocol for Diagnosis, Management, and Follow-Up Care of Growth and Development and Psychosocial Issues
Order Instructions:
Application: Protocol for Diagnosis, Management, and Follow-Up Care of Growth and Development and Psychosocial Issues
As pediatric patients grow from infancy to adolescence, there are many common growth and development and psychosocial issues that may potentially present. As an advanced practice nurse caring for these patients, you must be able to recognize red flags and select age-appropriate assessment and treatment options. In this Assignment, you prepare for your role in clinical settings as you design an age-specific protocol for the diagnosis, management, and follow-up care for a common growth and development or psychosocial issue.
To prepare:
•Reflect on the age group and the growth and development or psychosocial issue of a toddler.
•Think about the epidemiology of the issue.
•Consider an age-appropriate protocol for the diagnosis, management, and follow-up care of the issue you selected.
•Think about how culture might impact the care of patients that present with this issue.
To complete:
Write a 2- to 3-page paper that addresses the following:
•Explain a growth and development or psychosocial issue that might present in the age group you selected. Include the epidemiology of the issue in your explanation.
•Explain an age-appropriate protocol for the diagnosis, management, and follow-up care of this issue.
•Explain how culture might impact the care of patients who present with the growth and development or psychosocial issue you selected.
Note: The School of Nursing requires that all papers submitted include a title page, introduction, summary, and references. The Sample Paper provided at the Walden Writing Center provides an example of those required elements available at http://writingcenter.waldenu.edu/57.htm). All papers submitted must use this formatting.
SAMPLE ANSWER
Protocol for Diagnosis, Management, and Follow-Up Care
Developmental Issues in Toddlers
Nurses identify red flags in situations where children fail to meet the expected developments. There are guidelines that allow nurses to determine whether children exhibit a normal course of growth. In the toddler stage, for example, children are expected to exhibit tendency to seek independence (MacLeod, 2013). Aspects of growth considered in identifying red flags include gross and fine movements, communication, as well as emotional and social interactions (Queensland Government, 2010, Pg. 1). The capabilities that children attain at different stages allow for the evaluation of their growth pattern. Children may also exhibit traits that could suggest abnormalities. Both failure to express certain traits and expression of abnormal characteristics raise alarms termed as red flags.
Sleep disorders are possible developmental ailments that toddlers could express. Both excessive and reduced sleeping during toddler stage could be developmental disorders (Patient, 2015). Toddlers should develop the circadian pattern if their growth is normal. Common sleep abnormalities that toddlers express include difficulties in settling in beds, and unexpected waking up at night (Stores, 2009, Pg. 83). Other disorders include sleep apnea, periodic limb motion, and restless legs complex (Stores, 2009, Pg. 83). Epidemiological investigations show that approximately 30% of children experienced sleep disorders. Research shows that toddlers could have more of night-time waking compared to other age groups (Stores, 2009, Pg. 84). On the other hand, older children could have more nightmares compared to toddlers (Stores, 2009, Pg. 84). Toddlers with other developmental complications such as psychosocial insufficiencies are most affected by sleep disorders.
In assessing and diagnosing sleep disorders in toddlers, practitioners should obtain an informative history, and then conduct physical examinations on their clients. In most cases, evaluating toddlers on cognitive and developmental abnormalities is essential (Moturi & Avis, 2010, Pg. 24). Healthcare practitioners should differentiate normal sleeping from the abnormal type. For instance, it could be appropriate for toddlers to take habitual naps while it would be pathological for older children (Moturi & Avis, 2010, Pg. 24). Tools necessary in diagnosing sleep abnormalities include polysomnography. The tool is of particular importance for the assessment of obstructive apnea (Moturi & Avis, 2010, Pg. 24). It is advisable that healthcare providers involve parents in the management of sleep disorders in toddlers. Parents, guardians and other family members are likely to offer information that would enhance the understanding the etiology of sleep abnormalities in toddlers (Moturi & Avis, 2010, Pg. 24). Parents can also facilitate follow-ups, especially by recording patterns of sleep shown by their young ones. In addition to finding use in follow-ups, sleep diaries also provide rich information that is important to history collection (Moturi & Avis, 2010, Pg. 24). It is also advisable that practitioners screen toddlers for sleep disorders other than the already established ones. It is common for other abnormalities to accompany primary sleep abnormalities. For instance, cognitive impairment and day-time drowsiness could accompany sleep apnea (Moturi & Avis, 2010, Pg. 24).
Culture influences the diagnoses of sleep complications in toddlers. For instance, some cultures could encourage co-sleeping while others may not (Moturi & Avis, 2010, Pg. 24). The occurrence of certain sleep trait could be normal in some cultural setups while the same could call for complaints in other cultures. Lifestyles adopted through culture could also impact on both assessment and management of sleep disorders. Practices such as watching the television could certainly affect sleeping patterns in toddlers (Moturi & Avis, 2010, Pg. 24).
Prophylactic antibiotic timing and SSIs incidences
Evidence based research on Prophylactic antibiotic timing and SSIs incidences
Order Instructions:
Please follow the instruction attached.
SAMPLE ANSWER
Prophylactic antibiotic timing and SSIs incidences
Part 1: Evidence based research on Prophylactic antibiotic timing and SSIs incidences
Background
According to the national statistics, there are about 5% reports of surgical site infection (SSI) in all surgical processes every year. The study indicates that SSIs accounts about 2% of the mortality; and increases healthcare cost by 10 to 20%. Additionally, it has also been found that it increases hospital stays and increases the medical care costs (Shepard et al., 2013). Evidence based research indicates that about 60% of the SSIs are preventable if there the government implements quality based standards which should be implemented in the inpatient surgery. Therefore, the federal government should explore SSIs epidemiology, clinical consequences and the risk factors involved. This will help in establishing guidelines on the effective strategies such as hand hygiene, sustaining normothermia. This article explores the evidenced based practice that proper timing of prophylactic antibiotics could reduce the incidences of surgical site infection (Rafique, 2012).
Research indicates that SSIs are the second most challenge facing the public health. According to National Nosocomial Infection System, SSIs are infections that arise after operative procedures, within one month after the procedures. The efforts to lower the incidences of SSIs are not new concept. The efforts can be traced to the 19th Century with Lister who pioneered the use of antiseptic incidence in patients in the orthopedic ward. The issue of SSIs is not new in this health care facility (Teija-Kaisa, Eija, Marja, & Outi, 2012). For instance, about of 2% of patients undergoing surgical process in this health care facility reports SSIs. This causes about 5% readmission rates and 3% increase hospitalization days. In fact, it have been found that patients who present SSIs are 5 folds likely to be readmitted, with 60%of them being more likely stay in the ICU, and are two folds likely to pass away as compared to those who have no infection. The financial burden of the disease cannot be overlooked (Regimbeau et al., 2014; Hopper et al., 2015).
Purpose of the study
This study proposes that administering of prophylaxis antibiotics one hour before surgical procedures will lower the SSIs incidences. The study aims at establishing the most effective and best timing for the administration of the prophylactic antibiotic during the surgical procedures. This is because there is limited research on the adherence to the proposed Surgical Care Improvement guidelines; this has failed to prove that timely administration of prophylactic antibiotic reduces the incidence rates of SSIs (Alberta Health Services, 2014).
Evidence based practice
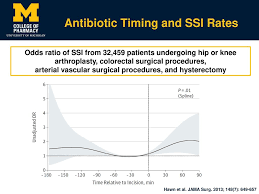
The issue of SSIs and its challenges is global. For instance, A retrospective study conducted using the Veterans affairs data on antibiotic administration timing on patient who were undergoing surgical procedures in the orthopedic, vascular, colorectal, and gynecologic procedures from 2005 to 2009 indicates that timing rate influenced the rate SSIs. Another study was conducted on 1922 patients who were primary care of hip arthroplasty in about 11 hospitals (Center for Healthcare Related Infection Surveillance and Prevention and Tuberculosis Control, 2012). The hip arthroplasty have been associated high morbidity due to their difficultness to study using the controlled trials. Additionally, the study indicated that the infection rate is generally low and would therefore not indicate significant outcomes. However, several other studies have indicates a proportional relationship indicating a U curve, with the lowest infection rate being recorded when the prophylactic antibiotic was administered about half an hour before incisions were made; and rates increased as time before the administration increased. Current US guidelines recommends that the prophylactic should be administered at least 60 to 120 min of incision (Fry, 2013).
Several other studies have demonstrated a good penetration of the tissue as well as excellent concentration of the antibiotics in the tissue when the administration of the antibiotic is done close incision time (Bowler, Welsby, Hogarth, & Towers, 2013).
The current clinical guideline on antimicrobial prophylaxis was developed by Burke. The guideline resulted from an investigation on the rate of inflammatory response on the surgical incision. The analysis found that the prophylactic antibiotic prophylactic process was most effective if the antibiotic was administered within 1 hour before the incision process. The analysis concluded that the bacteria were the most susceptible to the antibiotics, and their susceptibility was determined by the antibiotic timing as well as selection. Another retrospective study conducted by Classen and colleagues on 3000 patients who were undergoing surgical procedure indicated that patients received antibiotic one hour before the surgical process reported the lowest rates of SSIs (Anderson, 2014).
Study conducted by Merollini and colleagues using structured interviews on general practitioners, the nurses and physicians in the orthopedic department recommended the use of antibiotics within 30min to 1 hour before incision (Diamond, M. (2008). Other systematic review study, which used key words such as SSIs, orthopedic as well as prevention; indicated most studies reported that patients who received antibiotic prophylaxis would reduce the SSI rates to 1-3% in comparison to 4% without 8% with the control group. Based from this research study, one can therefore suggest that the most effective period to administer prophylaxis antibiotic is within one hour before the healthcare provider initiates the incision process because it reduces the risk of SSIs effectively (Center for Healthcare Related Infection Surveillance and Prevention and Tuberculosis Control, 2012).
Solution description
The proposed is that the healthcare providers in the surgical department will be encouraged to administer prophylactic antibiotic within one hour before the surgical process begins. This is because it will lead to reduction of the microorganism burden by three folds. Additionally, due to the increased residual effects associated with prophylactic antibiotic, the solution proposed will be consistent improved quality of life for patients, and reduced cost of care (Pearse et al., 2014).
However, just like many organization, this strategy could face numerous barriers from the healthcare providers. This is particularly so because the healthcare providers are not willing to change their routine pattern because they feel that they have been applying the same strategy for a long period of time, and would therefore hesitate to adopt the new developments/ change. To start with, the healthcare professionals in the surgical department tend to have low priority of the administration process (Fonseca, C. (2012).
This is attributable to the fact that they the anesthesiologists are more concerned in ensuring that the environment is safe, the right equipment is sterilized and safe. The healthcare professionals are more concerned about healthcare conditions that affect the patient immediately, and tend to ignore the impacts of SSIs because they do not affect the patient immediately. Some of the professionals claim that the administration process is tedious and time consuming thus limiting the administration of medication on time. Additionally, the healthcare facility workflow could limit the proper timing of the antibiotics .In most of the healthcare centers; the insertion of IV is done by the nurses and is time consuming. The healthcare facility process of communication could affect the communication of the new an effective protocols (Jarral, McCormack, Ibrahim, & Shipolini, 2010).
Majority of the health care facility communicate to their staff verbally, this indicates the importance of effective process of exchanging information such as use of automated systems to communicate new systems and to reduce confusions of adminsterring antibiotics in time by the nurses. Lastly, the concept of role perception determines the rate of drug administration, resulting to confusion as each healthcare provider denies that it is his or her responsibility. This causes further delays in the administration of the prophylactic antibiotic (Erb et al., 2014).
Implementation strategies
The first implementation strategy will be to educate the healthcare professionals in the surgical department on the important of using shorter duration for the administration of prophylactic antibiotic. The advantages will be discussed first with by the head of the surgical department with the aim of describing the feasibility of the matter. Secondly, poster concerning the best antibiotic agent and the recommended prophylactic antibiotic administration time will be hung in all vicinities surrounding surgical operation room including the physician room, the scrub sinks, and the operation room. This education is aims at enlightening the healthcare providers at individual level to transform the healthcare provider’s attitudes, behavior, as well as beliefs (Samant & Ramugade, 2014)
The second step will be to establish a multidisciplinary protocol that will be used to influence the healthcare providers on the effective management of SSIs through teamwork and effective communication, which will specify the timing as well as the sequences necessary for the achievement of the responsibility. Lastly, the institutions will implement the antibiotic timing programs, which will involve the integration of systems that will reduce, curtail, and control the process of antibiotic administration program. This will include approaches to measure parameters such as the written orders, computerized support programs among others (Feilmeier, Dayton, Sedberry, & Reimer, 2014).
Expected outcomes
Research associates increased utility of quality care improvements where the management of guidelines is followed reduces variability and miscommunication, which is often associated with increased medication and diagnostic errors. In this context, a successful intervention is one, which will involve identification of a nurse leader to serve and the motivator and change champions. This will require a number of in service refresher course training, use of systems that reminds the nurses on the timing of administration of prophylactic antibiotic and one with specific bench marking of physician. The ultimate expectations of these actions is to improve patients quality of life through reduced rates of SSIs, reduced hospital stays and overall reduction of the healthcare costs (Johnson Et al., 2013).
Part B: Picot analysis
Research Question: How effective is prophylactic antibiotic administration timing effective in the reduction of Surgical Sites Infections Incidences (SSIs)?
Type of patient/Problem
Intervention
Comparison intervention
Outcome
Patient in surgical Wards
Close administration of antibiotics (within one hour) before incision
Compared to delayed administration of antibiotics
Reduced incidences of SSIs
Reduced readmission rates
Reduced mortality and reduced length of hospital stays
Key word:
Colorectal patients, orthopedic, hip arthroplasty patients
Surgical site infection
Key Word Prophylactic antibiotics,
Administration rate within one hour
Antibiotic
Surgical site infection
Key Word:
Prophylactic antibiotics,
Administration rate within one hour
Health care quality
Key Word:
Hospital stays
Readmission rates
SSIs mortality
Practice guidelines
Search History
Literature search was done in three main databases using the University online database. The database included CINAHL, Proquest, and EBSCOhost. The key word used to run the search included ; Colorectal patients, orthopedic, hip arthroplasty patients, Surgical site infection, Prophylactic antibiotics, Administration rate within one hour, Antibiotic, Surgical site infection, Prophylactic antibiotics, Administration rate within one hour, Health care quality, Hospital stays, Readmission rates, SSIs mortality, Practice guidelines
From these key words, approximately 534 articles were generated. The articles were narrowed down using filter methods such as publication year. The articles chose were supposed to from 2010, to avoid generating outdated information. From these, the articles were narrowed down to 235, and when Key words “SSIs” and “prophylactic antibiotics” were applied, the articles were narrowed down to 45 articles. Out of these articles, 17 articles were chosen to compile the work based on the relevance of the abstract and the year of the publication.
Example
Hooper, T.D., Hibbert P.D., Hannaford, N.A, Jackson, N., Hindmarsh, D.M., Gordon, D.L., Coiera, E.C., Runciman, W.B.(2015). Surgical site infection—a population-based study in Australian adults measuring the compliance with and correct timing of appropriate antibiotic prophylaxis. Anesthesia and intensive care 43 (4); 461- 469
P- The population being studied by this article is the Australian Adults who are undergoing operative procedures. The problem being investigated is the rate of SSIs to evaluate the infection rates with and without correct timing of prophylactic antibiotic administration
The intervention suggested by this article is that proper timing of the administration of the prophylactic antibiotic reduces the incidences of SSIs considerably.
C- The study compares health outcomes of patients who experienced proper timing of the administration of the drugs with those who had delayed administration of the drug.
O- The outcome evaluated is the rate of adherence to proper timing, reduced health care costs and overall improve quality of life for patient.
Anderson, D. (2014). Prevention of Surgical Site Infection: Beyond SCIP. AORN Journal, 99(2), 315-319. doi:10.1016/j.aorn.2013.11.007
Bowler, P., Welsby, S., Hogarth, A., & Towers, V. (2013). Topical antimicrobial protection of postoperative surgical sites at risk of infection with Propionibacterium acnes: an in-vitro study. Journal Of Hospital Infection, 83(3), 232-237. doi:10.1016/j.jhin.2012.11.018
Diamond, M. (2008). Postsurgical Adhesions. Seminars In Reproductive Medicine, 26(04), 287-288. doi:10.1055/s-0028-1082386
Erb, S., Sidler, J., Elzi, L., Gurke, L., Battegay, M., Widmer, A., & Weisser, M. (2014). Surgical and Antimicrobial Treatment of Prosthetic Vascular Graft Infections at Different Surgical Sites: A Retrospective Study of Treatment Outcomes. Plos ONE, 9(11), e112947. doi:10.1371/journal.pone.0112947
Feilmeier, M., Dayton, P., Sedberry, S., & Reimer, R. (2014). Incidence of Surgical Site Infection in the Foot and Ankle with Early Exposure and Showering of Surgical Sites: A Prospective Observation. The Journal Of Foot And Ankle Surgery, 53(2), 173-175. doi:10.1053/j.jfas.2013.12.021
Fonseca, C. (2012). Nursing Care Indicators to Nursing Homes. Journal Of Nursing & Care, 01(03). doi:10.4172/2167-1168.1000107
Fry, D. (2013). Use of surgical-site infection rates to rank hospital performance across several types of surgery ( Br J Surg 2013; 100: 628-637). British Journal Of Surgery, 100(5), 637-637. doi:10.1002/bjs.9040
Jarral, O. A., McCormack, D. A., Ibrahim, S., & Shipolini, A. R. (2010). Should surgeons scrub with chlorhexidine or iodine prior to surgery? Oxford Journals, 12 (6), 1017-1021. doi: 10.1510/icvts.2010.259796
Johnson, A., Zywiel, M., Jones, L., Delanois, R., Stroh, D., & Mont, M. (2013). Reduced re-infection rates with postoperative oral antibiotics after two-stage revision hip arthroplasty. BMC Musculoskeletal Disorders, 14(1), 123. doi:10.1186/1471-2474-14-123
Pearse, R., Harrison, D., MacDonald, N., Gillies, M., Blunt, M., & Ackland, G. et al. (2014). Effect of a Perioperative, Cardiac Output–Guided Hemodynamic Therapy Algorithm on Outcomes Following Major Gastrointestinal Surgery. JAMA, 311(21), 2181. doi:10.1001/jama.2014.5305
Rafique, H. (2012). A retrospective case series study of a single centre’s experience of surgical site infection following purse-string closure versus linear closure of ileostomy sites. International Journal Of Surgery, 10(8), S26-S27. doi:10.1016/j.ijsu.2012.06.141
Regimbeau, J., Fuks, D., Pautrat, K., Mauvais, F., Haccart, V., & Msika, S. et al. (2014). Effect of Postoperative Antibiotic Administration on Postoperative Infection Following Cholecystectomy for Acute Calculous Cholecystitis. JAMA, 312(2), 145. doi:10.1001/jama.2014.7586
Samant, P., & Ramugade, S. (2014). Successful use of intravitreal and systemic colistin in treating multidrug resistant Pseudomonas aeruginosa post-operative endophthalmitis. Indian J Ophthalmol, 62(12), 1167. doi:10.4103/0301-4738.126991
Shepard, J., Ward, W., Milstone, A., Carlson, T., Frederick, J., Hadhazy, E., & Perl, T. (2013). Financial Impact of Surgical Site Infections on Hospitals. JAMA Surgery, 148(10), 907. doi:10.1001/jamasurg.2013.2246
Teija-Kaisa, A., Eija, M., Marja, S., & Outi, L. (2012). Risk factors for surgical site infection in breast surgery. J Clin Nurs, 22(7-8), 948-957. doi:10.1111/jocn.12009
We can write this or a similar paper for you! Simply fill the order form!
Content
1. Introduction to the paper includes a few general statements on the idea of nursing theory being applied to solve problems/issues in nursing practice, regardless of the specialty area of practice. For example, why would one pick a nursing theory to solve a practice problem? Would a grand, middle-range, or practice theory be best? Does the writer have any experience in using nursing theory this way? In addition, a brief one-paragraph summary of a specific nursing theory and information on the sections of the paper are provided. The selected nursing theory can be a grand theory, a middle-range theory, or a practice theory.
2. Description of the problem/issue for which strategies will be developed. The problem to be resolved must be in nursing leadership, nursing education, nursing informatics, or health policy. Scholarly evidence (in the form of a literature review) supporting the issue is included. The problem/issue could be local to one’s specific practice setting. For example, the setting might be a nursing unit, a nursing-education program, an informatics department, or a health-policy unit of a consulting firm. The problem/issue needs to be something that a nursing theory can impact, whether it solves the actual problem/issue or enables people affected by the problem/issue to deal with it. It is best if the problem/issue is from real life – something the writer of the paper has dealt with or is currently engaged in.
Some examples (these are fictitious examples)
a. A nursing unit has experienced rapid turnover of professional staff, including several nurse managers. A new nurse manager from outside of the nursing unit is appointed.
b. Informatics nurse specialists face a lot of resistance from all healthcare professionals to implementation of a computer-based order entry program. The implementation date will not be changed.
c. A nurse educator is assigned to take over a large class of undergraduate nursing students, with a mix of young adults and adults returning for a second degree. The subject is difficult, students have not been doing well, and frustration and tempers are impeding group work.
d. A health-policy nurse specialist works for a consulting firm that lobbies on behalf of many healthcare professions. Within the specialist’s work unit, there is much debate over the pros and cons of various policies being proposed for attention in the coming year.
3. Applying concepts and principles from the selected theory, one strategy for resolving the identified issue is described in depth. Details on how the theory would be applied are included (consider: who, what, when, where, and how). Rationales for the strategy as well as evidence from scholarly literature are included. One ethical and/or legal aspect of the strategy is discussed. Expected outcome(s) from implementing the strategy are proposed.
4. Concluding statements include new knowledge about applying nursing theory gained by writing the paper
Format and Special Instructions
1. Paper length: 6 pages minimum; 8 pages maximum, excluding title page and reference page. Points will be deducted for not meeting these requirements.
2. The textbook required for this course may not be used as a reference for this assignment.
3. A minimum of 3 scholarly references are used. References must be current – no older than 5 years, unless a valid rationale is provided. Consult with the course instructor about using an older source.
4. Title page, body of paper, and reference page(s) must be in APA format as presented in the 6th edition of the manual
5. Ideas and information from readings and other sources must be cited and cited correctly.
6. Grammar, spelling, punctuation, and citations are consistent with formal academic writing as presented in the 6th edition of the APA manual
SAMPLE ANSWER
Introduction
Barr and Welch (2012) suggest that leading change in health care has become more rampant among the nurse leadership. Strong leadership in partnership facilitates smooth transformational change. Nursing theory shape nurse practice in a myriad ways, and provides considerable positive impact. Nursing theory provides a framework, which support nursing practice and offers solutions to nursing ethical dilemmas, thereby ensuring delivery of quality care. Nursing theories assists the nurse discipline in the clarification of beliefs, goals, and values. This facilitates proper definition of the unique nurse contribution to the concept of care. In fact, nurse clinical practice standards are derived from the nursing theories. The nursing theory resolves challenges in educational, leadership and research as well as practice settings.
Depending on the health issue under investigation, there are three major types of nursing theory. Grand nursing theory is the broadest, but provides generalized propositions. This level of nursing theory reflects on the nurse practice, thereby offering very insightful solutions. Theories in this level include conceptual frameworks. The middle range theories scopes are narrower than Grand nursing theory. The importance of this level of nursing theory is that it acts a bridge between the grand nursing theory and nursing practice. The nursing practice theories have very limited scope. These theories are developed within a specific nursing practice. The nursing theories at this level offer intervention for nursing practice, and predict outcomes of nursing practice. The advantages of nursing theory will be demonstrated by Jean Watson’s theory (Clark, Zickar & Jex, 2013).
Identification of practice problem
The main issue in the health care facility I work at is staffing ratio. Literature indicates that nurse-staff ratio ensures quality of care. However, high turnover rates and reduced number of nurse graduates has been an ongoing challenge of nurse managers as well as administrators. Blignaut, Coetzee & Klopper (2013) argue that challenge is associated with negative patient outcome, reduced safety in work place and reduces patient satisfaction. The high turnover rates are attributable to nurse overwork, burnout, and fatigue. This affects nurse’s practice because the nurse lacks compassionate working.
Witges & Scanlan, (2014) state that the staffing ratio has been associated with reduced patient and nurse safety. The availability of health as nurses who have had ample rest is important in providing quality and empathetic acer. However, most work places are described with innumerable stressors, which often result to disease or even injuries. The stressors occur in various forms such as, characteristics of the facility’s leadership, internal and external changes the organization. Some of these changes includes lean contracts, use of advance technology without refresher courses, increased population of older workforce and high number of aging population seeking care in the healthcare facility have been associated with reduced patient safety.
The hazardous working condition can impair nurse’s health. This includes health complications such as musco-skeletal disorders, infections, mental discomfort, cardiovascular diseases, and other complications such as neoplastic diseases. Working for longer shift affects nurse sleep pattern and gastro-intestinal system. This results to psychological response such as stress and depression. Long hour shifts also increases rate of exposure to harmful chemicals and infectious agents. Long hour working can increase smoking and alcohol consumption rate, and caffeine use with the aim of fighting fatigue (Blignaut, Coetzee & Klopper, 2013).
According to Lievens and Vlerick (2013), the traditional approach of addressing the nurse staffing issues has not been very successful. The paper suggests that by applying the theory of human caring will help solve this challenge. This is because the model points out on nursing leadership solutions, which can help the administrators and the healthcare management by guiding them on how to solve this issue amicably.
Proposition of Jean Watson’s theory
Thomas-Hawkins & Flynn (2015) study indicates that the main concepts of the Jean Human caring theory assume that the foundation of nursing and its essence resides in provision of care. According to this theory, quality care provision is enhanced through interpersonal interaction. The main and basic assumptions of the theory include the fact that caring is effectively practiced through interpersonal interaction. The theory suggests there are a set of carative factors, which increase patient satisfaction. The theory also suggests that effective care promotes health of the patient, family and the community at large. Additionally, the theory suggests that caring responses accept a person as what she is currently and what she may become in the future. The nursing theory concept suggest that a caring environment is important as it provides an opportunity for a person to choose the best care plan for themselves at any given point of care.
Witges and Scanlan (2014) research indicates that a caring leadership is more healthogenic, this makes caring an integral concept to nursing practice. The theory has ten carative factors including the establishment of humanistic-altruistic leadership system. This factor is mediated through experiences and exposures to various healthcare challenges. This factor is paramount for maturation of nurse leadership and management skills. This nursing theory suggests that an effective leadership is one that cultivates sensitivity to others and to oneself. The nurse leader must ensure that the nurses are more sensitive and authentic. Moreover, the nurses should be encouraged such that self-actualization and self-growth is sustained. This in turn ensures that those people the nurse interacts with are empowered, thereby promoting health.
Empowered nurses will ensure that they build a strong relationship through effective communication. Effective communications is associated with good work place rapport and strengthen the aspects of human caring. The theory outlines that a good leadership is characterized by empathy, congruence, and warmth. These feelings foster a caring relationship between healthcare facility management and their staff as it improves the organizations awareness. The human caring theory enables the nurse leader to solve problems following systematic scientific approach of problem solving. This is the only approach to control, predict and to find the best solution. The human caring science should always be neutral and objective. The human caring theory focuses on the learning-teaching process. This will help the nurse understand the situation better, enabling them have a cognitive plan (Clark, Zickar & Jex, 2013).
Blignaut, Coetzee, and Klopper (2013) argue that for quality delivery of services, the model suggests that nurse must work in a safe environment. Tis will help the nurse to offer supportive and protective care adequately. The human caring theory recommends that both the internal and external environments should be at equilibrium as both environment are interdependent. The model as is grounded in a hierarchy of human demands similar to that of Maslow’s, and each need or demand is as important as the principles of nursing. Therefore, to provide an optimal care, the needs should be valued and attended. Lastly, the model has some allowance for existence of phenomenological forces. Phenomenology in this case refers to the way people understand and value this i.e. people’s opinion. The model allows the integration of psychology in nursing leadership. This helps the nurse and the organization management to mediate the concept of holistic nursing practice, and identify the best approach, which will empower nurses, improve staff ratio, lower nurse workloads and strengthen the quality of care.
Application of Watson’s theory
Witges and Scanlan (2014) reveals that Nurse Leaders can use this theory to address nurse safety issues associated with reduced nurse-staff ratio. Using the ten caritas, the health care facility can address the issue of nurse staffing and by enable the staff engage in holistic nursing practices, and making the uses engage in self-care. Additionally, the organization can plan on policies, which will ensure nurses do no work for long hours. The organization leadership should ensure that the nurses have enough time to rest so that they can rejuvenate. Incorporating this theory into practice, provides a great impact to the work environment as well as positively impact on the nurse’s perception. The theory enables the nurses to incorporate a caring practice in their practice; caring to patients and to their health’s. This indicates that there is connectedness between nurse leadership, nurse and the patients.
Strategy Rationale
Nurse safety is an integral component in any health care facility; however, the concept is overlooked. There are limited resources on the role of nurse leadership in enhancing staffing ratios. With the shortages of nurses in the country, it is high time that for leadership to explore other options such as the adoption of new technology such as robotics, telehealth, use of sensors in beds, motion sensors and thermos-sensors to help the nurse in delivering their services. Other options such as employing of unregistered nurses as staff assistance, more volunteers, and interns could be other options, which can be applied to reduce nurse workloads (Blignaut, Coetzee & Klopper, 2013).
According to Clark, Zickar & Jex, (2013) the strategy intends to reform the healthcare facility policies and protocols, which acts as barriers to improving, nurse safety through increasing nurse-staff ratio and reducing overworking the nurses. The exact model, which will be applied in this strategy, is Continuous Quality Model commonly referred to as FOCUS-PDSA. The Strategy rationale includes searching and seeking the underlying concept, which cause high turnover rates and increased workloads for the employees. This includes exploring options of integrating computerized health care devices such as Tele-health concept. Organization committee comprising of relevant stakeholders will be formed. These people (including nurses, managers, head of departments and community representatives) will preside over the barriers and facilitators of working; analyze the discrepancies and to establish the most effective interventions.
Expected outcome
The evaluation of the expected outcome will be done after one year. However, this should not be limited within this time because interventions outcomes may take a while before they are realized. The expected outcome includes improved and safe working environment. The nurses should not act for long hours. The turnover rate should decrease as well as the number of work injury or ailment related complication. The benefits of improving working environment for the nurses are manifested through increased quality of care. This includes reduced number of hospital acquired infections, hospital falls and postoperative infections. This is because the nurses will be in a position to deliver quality care, with minimal confusion or error. Relaxed and nurses with adequate rests manifest proper communication and interpersonal skills. This implies that there will be a reduction in medical errors, improved quality of life, and patient’s satisfaction.
The main challenges with this nursing theory is that it does not rely on the conventional mechanism of ensuring that only qualified people are employed, which are still being applied in most of the healthcare facility. Additionally, the theory lacks mechanisms to motivate nurse work force to ensure that they are retained. This implies that the theory is somewhat too abstract that the leaders may become reluctant to integrate into practice (Blignaut, Coetzee & Klopper, 2013; Witges & Scanlan, 2014).
Conclusion
Nurse staffing and nurse safety is a major issue, which need to be addressed. For a long time, these challenges have been solved using shortsighted interventions such as additional incentives and recruitment bonuses. These interventions solve the problems temporarily, and introduce fiscal difficulties to the organization. This calls for the integration of nursing theory to address this issue more amicably, through practical interventions. This implies that the nurse leaders must be involved, and must apply nursing theory to identify the underlying mechanism. The nursing theory should be applied when exploring available options. It should also be applied when making long-term changes that will shape the health care facility in to a safer environment for both the service user and service provider. Using theoretical framework, the nursing leadership as well as organizations will record higher employee retention rate, and simultaneously improve the quality of care and patients outcome.
Reference list
Barr, J., & Welch, A. (2012). Keeping nurse researchers safe: workplace health and safety issues. Journal Of Advanced Nursing, 68(7), 1538-1545. doi:10.1111/j.1365-2648.2012.05942.x
Blignaut, A., Coetzee, S., & Klopper, H. (2013). Nurse qualifications and perceptions of patient safety and quality of care in South Africa. Nurs Health Sci, 16(2), 224-231. doi:10.1111/nhs.12091
Clark, O., Zickar, M., & Jex, S. (2013). Role Definition as a Moderator of the Relationship Between Safety Climate and Organizational Citizenship Behavior Among Hospital Nurses. J Bus Psychol, 29(1), 101-110. doi:10.1007/s10869-013-9302-0
Lievens, I., & Vlerick, P. (2013). Transformational leadership and safety performance among nurses: the mediating role of knowledge-related job characteristics. J Adv Nurs, 70(3), 651-661. doi:10.1111/jan.12229
Thomas-Hawkins, C., & Flynn, L. (2015). Patient Safety Culture and Nurse-Reported Adverse Events in Outpatient Hemodialysis Units. Res Theory Nurs Prac, 29(1), 53-65. doi:10.1891/1541-6577.29.1.53
Witges, K., & Scanlan, J. (2014). Understanding the Role of the Nurse Manager: The Full-Range Leadership Theory Perspective. Nurse Leader, 12(6), 67-70. doi:10.1016/j.mnl.2014.02.007
We can write this or a similar paper for you! Simply fill the order form!
Developing a Professional Portfolio in Nursing Order Instructions: Final Project Instructions
Capstone Project
Final Project
Developing a Professional Portfolio in Nursing
Read and review the PDF article: Developing a Professional Portfolio in Nursing
Develop a Plan for Professional Development; there is a sample plan on page 75 of the article.
Develop your Portfolio; (the article discusses 2 types of Portfolios; Best Work and Growth and Development). You will develop a Growth and Development Portfolio
On page 76 and 77 of the article, it states what needs to be included in the Portfolio. DO NOT submit to me any private health information or your social security number!!! I do not need to see your transcripts or performance appraisals. I want you to know these are recommended, but I don’t want them.
All work must be in 12 pt. font, APA format, and any references properly cited.
Do not copy and paste your work it must be submitted as a word document by attachment.
Marilyn H. Oermann
A professional portfolio is a collection of carefully selected materials
that document the nurse’s competencies and illustrate the expertise of
the nurse. Since a portfolio is developed over time, it also provides a
way of monitoring professional development. By periodically reviewing
the portfolio, nurses can assess their progress in meeting personal and
professional goals and can better plan their careers in nursing. This
article describes professional portfolios, their uses in nursing, and how
to develop and maintain one.
Marilyn H. Oermann, PhD, RN, FAAN,
is il professor in the College of Nursing
at Wayne State University In Detroit,
Michigan.
11 nurses should maintain a
professional portfolio to
reflect on their own development
of knowledge and
skills over time, present
levidence of compefendes,
and market themselves when applying
for career ladder positions or new
jobs in nursing.
A professional portfolio contains
materials fhat document the nurse’s
competencies and experiences and
Illustrate the career pat±i of the nurse.
Artists, photographers, designers, and
other professionals use portfolios to
showcase their work for clients and
potential employers. Portfolios in nursing
accomplish the same purpose —
they showcase the nurse’s background
and expertise for others fo review. This
article describes professional portfolios,
their uses in nursing, and how to
develop and maintain one.
Professional Portfolios
A professional portfolio is a compilation
of carefully selected materials that
dt5cumenf the nurse’s competencies.
The materials placed in a portfolio
illustrate the background, skills, and
expertise of the nurse (Trossman,
1999). The portfolio also provides a
way of monitoring the nurse’s own
professional development- By periodically
reviewing the portfolio, nurses
can assess their progress in meeting
personal and professional goals and
can better plan their careers in nursing.
The portfolio does not replace the
resume or curriculum vitae, but provides
information not available from
fhese alone. A resume and curriculum
vitae list the educational institutions
attended, the positions held, and
other background informafion about
the nurse. The portfolio provides evidence
of the competencies and
expertise of fhe nurse developed as a
result of fhese experiences.
Types of Portfolios
There are two types of portfolios, bestwork
and growth and development
(Gaberson & Oermann, 1999; Oermann
& Gaberson, 1998). Best-work
portfolios provide evidence of the
nurse’s competencies and expertise.
These portfolios are used as doaimentafion
for career ladder promotions,
job applications, annual performance
reviews, accreditations, initial and
continuing certification, and situations
in which other people will be
reviewing the portfolio. These portfolios
contain carefully selected materials
that are organized, labeled, and
prepared for review by others.
Growth and development portfolios
are designed for nurses to monitor
In the portfolio, the nurse can list
professional goals to be achieved
and related time frames, and the
nurse can use the portfolio to
monitor progress in meeting them.
their progress in meeting personal and
professional learning goals. Nurses use
this type of portfolio to evaluate tiieir
own learning and development, not
for others to review. The growth and
development portfolio is a working
document that provides ongoing evidence
of competencies. The nurse can
then select materials from this document
to include in a best-work portfolio
that is shown to others.
Uses of Portfolios in Nursing
Portfolios in nursing may he used for
professional development, for career
ladder promotions and wifh joh applications,
for annual performance
appraisals, as documentation of employee
performance for accreditation
surveys, when applying to educational
programs, and fo document continuing
competence.
Professional Development
A portfolio enables nurses tt) monitor
the development of their competencies
over a period of time. The documents
in a porftoiio provide evidence of what
has been accomplished fo meet personal
and professional learning needs,
progress in achieving career goals, and
where further learning is needed.
Used in this way, the porffolio
serves as a plan for professional development.
Registered dietitians and dietetic
technicians recently began
using the portfolio for recertification;
the porffolio includes a learning plan,
a log of completed continuing professional
activities with supporting documentation,
and an evaluation of outcomes
of learning (l’erfel, 1999),
In nursing the porffolio could be
used as a continued competency documenfation
tool. Nurses could list
learning acfivities they have completed,
evaluafe fheir effectiveness in promofing
professional growth and continued
competency, and specify goals
to be accomplished.
In using fhe portfolio as a plan for
professionai development, fhe nurse
progresses fhrough four steps, similar
to the nursing process.
IStep 1 is the learning needs
assessment in which the nurse
evaluates his or her own knowledge
and skills to identify areas for furfher
learning. From this needs assessment,
the nurse identifies personal and professional
goais fo be met. This step is
similar to the assessmenf and diagnostic
phases of the nursing process
(Oermann, 1998).
2The next step is to develop a
plan for meefing those learning
needs. The plan may include inservice
and continuing education, completion
of .selected clinical experiences
and other types of learning acfivifies,
independent pracfice of skills, reading
of arficles and other types of publications
to fill gaps in knowledge, and
many ofhers. All of these acfivities
wilh accompanying due dafes are
included in fhe learning plan.
3The third step is implemenfation
of the plan, which involves
completing tiie activities specified in it.
The implementation dafes are included,
thereby providing a record of continued
learning and development for
review by others. It also is helpful fo
include a list of maferials fo be collected
for fhe portfolio that provide evidence
of the learning activifies completed,
such as records of confinuing
education.
4The final step is evaluation of
fhe oufcomes of learning and
revision of the plan if indicafed. In fhis
sfep, fhe nurse assesses progress made
in meefing learning needs and decides
on areas for continued professional
development. The portfolio includes
the plan for professional development
with accompanying maferials fhat validafe
completion of the learning acfivities,
competencies developed and
maintained, new knowledge gained,
and other outcomes of learning. Table
1 provides a sample professional development
plan that can be included in a
portfolio.
A porffolio used in this way also
helps nurses in planning their careers.
.All too often nurses change posifions
wifhouf considering where they wanf
to he in 1, 5, and 10 years, and they do
not evaluate how each position fits
into their career plans. In the portfolio,
the nurse can list professional
goals to be achieved and related time
frames and can use the portfolio to
monitor progress in meeting them. In
this way, the portfolio is a career-planning
joun^al fhaf guides setting career
goals and making career decisions
(Koch etal., 1998).
Career Ladder Promotions
and Job iVIobility
Another use of the portfolio is for
career ladder promotions within the
organization and for seeking new positions
in nursing. The portfolio provides
justification for a career ladder promotion
in fhe clinical setting and contains
documents that support it {Brooks et
al., 1998).
The nurse also can use a portfolio
when applying for a new position. The
portfolio demonstrates to the potential
employer the knowledge, skills, and
relevant experiences of the nurse. With
the portfolio, nurses can more easily
market fhemselves to potential employers,
illustrating their value and how
they could fulfill the demands of the
position. Portfolios allow nurses to take
control of their professional development
(Brooks & Madda, 1999). A related
advantage is that the portfolio is
readily available for career transitions.
74 Orthopaedic Nursing – March/April 2002 – Volume 21 • Number 2
TABLE 1
Sample Plan for Professional Development
Learning Needs
Patient
education
,1
Goal
Improve knowledge
and 5kills
for teaching
patients with
varied health
problems
Learning
Activities
with Due Dates
Develop teaching
plans for patients
on unit/adapt
standardized
plans; have manager
or another
expert nurse
review them
(due 10/01)
Attend CE
program on
patient teaching
(due before
1/02)
Read articles on
patient teaching
(due 9/01)
Review Internet
sites that could
be used by
patients on unit
(due 11/01)
Serve on unit
patient
education
committee
(join by 10/01)
Activity and
Date Done
3 plans
developed and
reviewed by
manager;
9/22/01
Attended
inservice
program on
11/12/01
Read two articles
(see portfolio
documents);
9/2/01
Served on committee
to rev\ew
sites; completed
literature review
and evaluated 28
Internet sites.
Project completed
1/4/02
Committee
member;
developed
pamphlet on
calcium
supplements
Contact
Hours
4 contact hours
Passed CE test
with article for
2 contact hours
Evaluation
Improved understanding
of how
to adapt teaching
materials for
patients. Written
plans met criteria
established by
manager and
used in facility
Passed posttest
Able to use
concepts in
own teaching;
improved
strategies for
teaching older
patients
Sites being
developed as
handout for
patients;
improved
knowledge of
using Internet for
health teaching
Continuing
committee
member
Supporting
Materials in
Portfolio
3 teaching plans
Copy of
program;
certificate of
attendance;
posttest results
Articles;
certificate
indicating
contact hours
received
Worksheets for
review of sites;
final document
Committee
minutes;
summary report
Annual Performance Appraisals
In addition to self growth and professional
development, the portfolio also
is a valuable tool for annual performance
appraisals. When portfolios are
Sample Plan for Professional Development
Learning Needs
Patient
education
,1
Goal
Improve knowledge
and 5kills
for teaching
patients with
varied health
problems
Learning
Activities
with Due Dates
Develop teaching
plans for patients
on unit/adapt
standardized
plans; have manager
or another
expert nurse
review them
(due 10/01)
Attend CE
program on
patient teaching
(due before
1/02)
Read articles on
patient teaching
(due 9/01)
Review Internet
sites that could
be used by
patients on unit
(due 11/01)
Serve on unit
patient
education
committee
(join by 10/01)
Activity and
Date Done
3 plans
developed and
reviewed by
manager;
9/22/01
Attended
inservice
program on
11/12/01
Read two articles
(see portfolio
documents);
9/2/01
Served on committee
to rev\ew
sites; completed
literature review
and evaluated 28
Internet sites.
Project completed
1/4/02
Committee
member;
developed
pamphlet on
calcium
supplements
Contact
Hours
4 contact hours
Passed CE test
with article for
2 contact hours
Evaluation
Improved understanding
of how
to adapt teaching
materials for
patients. Written
plans met criteria
established by
manager and
used in facility
Passed posttest
Able to use
concepts in
own teaching;
improved
strategies for
teaching older
patients
Sites being
developed as
handout for
patients;
improved
knowledge of
using Internet for
health teaching
Continuing
committee
member
Supporting
Materials in
Portfolio
3 teaching plans
Copy of
program;
certificate of
attendance;
posttest results
Articles;
certificate
indicating
contact hours
received
Worksheets for
review of sites;
final document
Committee
minutes;
summary report
Annual Performance Appraisals
In addition to self growth and professional
development, the portfolio also
is a valuable tool for annual performance
appraisals. When portfolios are
used for self-growth, fhis is defined as
formative evaluation. This type of
evaluafion gives feedback to the nurse
about progress in developing competencies
for practice. Formative evaluation
identifies where further learning
and development are needed.
Annual performance appraisals, a
form of summative evaluation, are
done at periodic intervals to indicate
the extent to which the nurse has
achieved specific competencies. Summative
evaluation certifies the competencies
of the nurse at a particular
point in time (Oermann, 199K, 1999;
Oertnann & Gaberson, 1998).
For annual reviews the nurse can
collect and organize documents that
demonstrate achievement of the performance
standards. The portfoiio
then shows how the nurse met these
standards or exceeded them. The portfolio
can be subinifted to tiie manager
before tiie annual review so the manager
has this documentation when
Orthopaedic Nursing – March/April 2002 – Volume 21 • Number 2 75
It is best to save more materials
than needed for the current portfolio
because at a later time^ the purpose
of the portfolio might change.
completing the review. In this way the
portfoiio validates and supplements
known information about the nurse
(Brooks & Madda, 1999).
Accreditation Surveys
Portfolios also can be used for accreditation
surveys as a means of doaimenting
employees’ performance and
to provide additional data to support
the accreditation standards. With Joint
Commission on Accreditation of
Heaithcare Organizations surveys, the
portfolio complements the human
resource files by containing documents
tliat vaiidate the nurse’s competencies
(Brooks & Madda, f999).
Applications for Nursing
Education Programs
In some nursing education programs,
a portfoiio can be submitted with the
application materials. The portfolio
carl be used to summarize past educational
and work experiences as a basis
for advanced placement in tiie nursing
program. Once accepted into the
program, the nurse can expand the
portfoiio to include new knowledge
and skills acquired in the program.
Continuing Competence
Documentation
Portfolios provide documentation of
continued competence of the nurse.
There are some proposals being considered
that would require RNs to
maintain a professional portfolio for
relicensure and certification.
Exampies of documents for the
portfolio are skili assessment inventories;
testing at specified intervais (e.g..
computer-simulated testing in the
practice specialty, initial specialty certification,
or recertification testing);
appraisals of role expectations and
individual abilities; academic nursing
education; continuing education directed
toward the nurse’s area of clinical
practice; and partnerships hetween the
regulatory body and employers for the
purpose of validating nurses’ competency
in practice (McGuire et al., 1998),
Nurses in Engiand are required to
maintain a personal professionai profile,
a portfolio, as a record of their professionai
development and how they
fulfilled the requirements for continuing
education (English National Board
for Nursing, Midwifery and Health
Visiting, 1998).
Portfolios are an effective way of
validating competencies for recertification.
In a portfolio nurses can collect
materials that provide evidence of
their continuing competencies and
how they developed them.
Documents to Include
in a Portfolio
The documents in a professional portfolio
are selected according to its purpose.
Materiais in a portfolio for self
growth and career development wiil
differ from ones in a portfolio designed
to justify a career ladder promotion.
Differences also occur because
of variations in nurses’ clinical
specialties, units
Sample Plan for Professional Development
Learning Needs
Patient
education
,1
Goal
Improve knowledge
and 5kills
for teaching
patients with
varied health
problems
Learning
Activities
with Due Dates
Develop teaching
plans for patients
on unit/adapt
standardized
plans; have manager
or another
expert nurse
review them
(due 10/01)
Attend CE
program on
patient teaching
(due before
1/02)
Read articles on
patient teaching
(due 9/01)
Review Internet
sites that could
be used by
patients on unit
(due 11/01)
Serve on unit
patient
education
committee
(join by 10/01)
Activity and
Date Done
3 plans
developed and
reviewed by
manager;
9/22/01
Attended
inservice
program on
11/12/01
Read two articles
(see portfolio
documents);
9/2/01
Served on committee
to rev\ew
sites; completed
literature review
and evaluated 28
Internet sites.
Project completed
1/4/02
Committee
member;
developed
pamphlet on
calcium
supplements
Contact
Hours
4 contact hours
Passed CE test
with article for
2 contact hours
Evaluation
Improved understanding
of how
to adapt teaching
materials for
patients. Written
plans met criteria
established by
manager and
used in facility
Passed posttest
Able to use
concepts in
own teaching;
improved
strategies for
teaching older
patients
Sites being
developed as
handout for
patients;
improved
knowledge of
using Internet for
health teaching
Continuing
committee
member
Supporting
Materials in
Portfolio
3 teaching plans
Copy of
program;
certificate of
attendance;
posttest results
Articles;
certificate
indicating
contact hours
received
Worksheets for
review of sites;
final document
Committee
minutes;
summary report
Annual Performance Appraisals
In addition to self growth and professional
development, the portfolio also
is a valuable tool for annual performance
appraisals. When portfolios are
used for self-growth, fhis is defined as
formative evaluation. This type of
evaluafion gives feedback to the nurse
about progress in developing competencies
for practice. Formative evaluation
identifies where further learning
and development are needed.
Annual performance appraisals, a
form of summative evaluation, are
done at periodic intervals to indicate
the extent to which the nurse has
achieved specific competencies. Summative
evaluation certifies the competencies
of the nurse at a particular
point in time (Oermann, 199K, 1999;
Oertnann & Gaberson, 1998).
For annual reviews the nurse can
collect and organize documents that
demonstrate achievement of the performance
standards. The portfoiio
then shows how the nurse met these
standards or exceeded them. The portfolio
can be subinifted to tiie manager
before tiie annual review so the manager
has this documentation when
Orthopaedic Nursing – March/April 2002 – Volume 21 • Number 2 75
It is best to save more materials
than needed for the current portfolio
because at a later time^ the purpose
of the portfolio might change.
completing the review. In this way the
portfoiio validates and supplements
known information about the nurse
(Brooks & Madda, 1999).
Accreditation Surveys
Portfolios also can be used for accreditation
surveys as a means of doaimenting
employees’ performance and
to provide additional data to support
the accreditation standards. With Joint
Commission on Accreditation of
Heaithcare Organizations surveys, the
portfolio complements the human
resource files by containing documents
tliat vaiidate the nurse’s competencies
(Brooks & Madda, f999).
Applications for Nursing
Education Programs
In some nursing education programs,
a portfoiio can be submitted with the
application materials. The portfolio
carl be used to summarize past educational
and work experiences as a basis
for advanced placement in tiie nursing
program. Once accepted into the
program, the nurse can expand the
portfoiio to include new knowledge
and skills acquired in the program.
Continuing Competence
Documentation
Portfolios provide documentation of
continued competence of the nurse.
There are some proposals being considered
that would require RNs to
maintain a professional portfolio for
relicensure and certification.
Exampies of documents for the
portfolio are skili assessment inventories;
testing at specified intervais (e.g..
computer-simulated testing in the
practice specialty, initial specialty certification,
or recertification testing);
appraisals of role expectations and
individual abilities; academic nursing
education; continuing education directed
toward the nurse’s area of clinical
practice; and partnerships hetween the
regulatory body and employers for the
purpose of validating nurses’ competency
in practice (McGuire et al., 1998),
Nurses in Engiand are required to
maintain a personal professionai profile,
a portfolio, as a record of their professionai
development and how they
fulfilled the requirements for continuing
education (English National Board
for Nursing, Midwifery and Health
Visiting, 1998).
Portfolios are an effective way of
validating competencies for recertification.
In a portfolio nurses can collect
materials that provide evidence of
their continuing competencies and
how they developed them.
Documents to Include
in a Portfolio
The documents in a professional portfolio
are selected according to its purpose.
Materiais in a portfolio for self
growth and career development wiil
differ from ones in a portfolio designed
to justify a career ladder promotion.
Differences also occur because
of variations in nurses’ clinical
specialties, units
Charlette:
thank you allow me to send the payment link please
Charlette:
hi please allow me to send
chic:
This page 75,I will send pages 76 and 77
Charlette:
ok
chic:
75
It is best to save more materials
than needed for the current portfolio
because at a later time^ the purpose
of the portfolio might change.
completing the review. In this way the
portfoiio validates and supplements
known information about the nurse
(Brooks & Madda, 1999).
Accreditation Surveys
Portfolios also can be used for accreditation
surveys as a means of doaimenting
employees’ performance and
to provide additional data to support
the accreditation standards. With Joint
Commission on Accreditation of
Heaithcare Organizations surveys, the
portfolio complements the human
resource files by containing documents
tliat vaiidate the nurse’s competencies
(Brooks & Madda, f999).
Applications for Nursing
Education Programs
In some nursing education programs,
a portfoiio can be submitted with the
application materials. The portfolio
carl be used to summarize past educational
and work experiences as a basis
for advanced placement in tiie nursing
program. Once accepted into the
program, the nurse can expand the
portfoiio to include new knowledge
and skills acquired in the program.
Continuing Competence
Documentation
Portfolios provide documentation of
continued competence of the nurse.
There are some proposals being considered
that would require RNs to
maintain a professional portfolio for
relicensure and certification.
Exampies of documents for the
portfolio are skili assessment inventories;
testing at specified intervais (e.g..
computer-simulated testing in the
practice specialty, initial specialty certification,
or recertification testing);
appraisals of role expectations and
individual abilities; academic nursing
education; continuing education directed
toward the nurse’s area of clinical
practice; and partnerships hetween the
regulatory body and employers for the
purpose of validating nurses’ competency
in practice (McGuire et al., 1998),
Nurses in Engiand are required to
maintain a personal professionai profile,
a portfolio, as a record of their professionai
development and how they
fulfilled the requirements for continuing
education (English National Board
for Nursing, Midwifery and Health
Visiting, 1998).
Portfolios are an effective way of
validating competencies for recertification.
In a portfolio nurses can collect
materials that provide evidence of
their continuing competencies and
how they developed them.
Documents to Include
in a Portfolio
The documents in a professional portfolio
are selected according to its purpose.
Materiais in a portfolio for self
growth and career development wiil
differ from ones in a portfolio designed
to justify a career ladder promotion.
Differences also occur because
of variations in nurses’ clinical
specialties, units and settings in wbicii
employed, responsibilities, and goais.
Nurses vary in the competencies they
need to maintain, which ultimately
affecfs the documents placed in a
portfolio. As a result, no two portfolios
will be fhe same.
Because there are so many documents
that could be placed in a portfolio,
the nurse should be selective
about what to include. The portfolio
should contain materials that iliustrate
the nurse’s competencies, highlight
achievements and educational
accomplishments, and achieve the
purpose of deveioping the portfolio,
rather than every document produced
ill a career.
For example, to demonstrate competencies
in muitidisciplinary collaboration,
the portfolio might include
materials developed by a collaborative
practice team on which the nurse
served, revised pathway and order set
developed by the team noting the
nurse’s role in this team effort, educational
program developed for nursing
staff to prepare them for using the
new pathway, minutes of meetings
and the nurse’s participation in them,
and a letter from selected team members
summarizing the nurse’s contributions.
Table 2 illustrates the
types of documents that might be
placed in a portfolio.
As documents are collected for the
portfolio, the nurse should label and
dafe fhem. It is best to save more
materials than needed for the current
portfolio because at a later time, the
purpose of the portfolio might change.
Materials can be organized in files so
they are not misplaced, or they may
be placed directly into the portfolio.
Rather than placing ail documents in
one file, it is best to develop a filing
system that matches the purposes of
the portfolio. For instance, if fhe portfolio
is intended to justify a career ladder
promotion, files can be prepared
for each criterion to be met; then as
documents are collected, they can be
placed in the file that relates to the criterion.
O’Halloran (1996) suggested using
at ieast four separate files:
• Education, which contains the resume
or curriculum vitae, other formal
education, the license number
and state, certifications with titles
and organizations, and awards
• Performance, including position descriptions
and evaluations of perfonnance,
reference letters, commendations,
and other evidence of meeting
performance expecfations
• Community service and profession-
76 Orthopaedic Nursing – March/April 2002 – Volume 21 • Number 2
TABLE 2
Materials for Professional Portfolio
• Resume
• Plan for professional development with supporting documents
that verify activities completed and learning outcomes
• Academic transcripts indicating completion of nursing
programs and additional course work
• Health records
• Job description
• Performance appraisals
• Competency checklists
• Certifications (e.g., ACLS and specialty certifications) with
renewal dates and hours completed toward recertification
• Continuing education (with documentation of contact hours)
and relationship to personal and professional goals
• Inservice education programs attended (e.g., skill updates,
competency validations, unit-based programs, and others) with
record of attendance
• Other types of educational experiences cbrhpleted in the organization
with record of attendance
I Materials produced for patients and staff (e.g., teaching
forms, skills checklists, and others); quality improvement
projects; and other materials that indicate knowledge,
competencies, and expertise of nurse
I List of committees, materials developed by committees, and
documentation of participation (e.g., minutes of meetings,
reports of committees, summary of responsibilities for
committee work)
> Presentations given on unit, in clinical agency, in community,
and in other settings; documents developed for presentations
(e.g., programs, lecture outlines, handouts, sample transparencies
and slides [hard copies], learning activities
completed by participants, and others); and summaries
of participants’ evaluations
I Projects on unit and institution-wide, grants, and research studies
with documentation of own role, funding if applicable, time
frame of project, results, and how findings were disseminated
(include reports of projects)
I Writing samples (e.g., published articles in refereed journals,
papers in non-refereed journals, columns, newsletters, book
reviews, summaries of literature reviews, letters to the editor,
flyers, and otber examples of writing skills)
al nursing activities in the community,
such as membership in nursing
and other types of organizations,
conimittee work, and other types of
participation
• Continuing education witb documentation
of programs attended,
CEUs and contact hours received,
and outcomes of learning from these
programs
When the portfolio will be reviewed
by others, the nurse should
select the most relevant documents to
include, orgariize them logically, and
label eacb one. In organizing and labeling
the materials, the nurse should
make the relationship clear between
tbe docaiments and competencies they
vaiidate, should indicate how the
materials support a performance appraisal
or career ladder promotion, and
should clarify how they demonstrate
tbe nurse’s knowledge and expertise.
Review of the portfoiio by a colleague
will often show where furtlier clarification
is needed.
The portfolio can be placed in a
three-ring binder with pockets, it is
time-saving to develop as many documents
as possible on the computer so
tbey can be updated easily. When the
portfolio is reviewed by others, for
instance, with annuai performance
appraisals or when applying for a new
position, it should “look professionai.”
Tbis means that materials should
be typed, sections should be labeled,
and a table of contents should be prepared.
The nurse’s name and contact
information should be easy to find.
Often nurses include their resumes or
curriculum vita in a portfolio, which
can be placed in the beginning.
Next Step
Nurses across clinical speciaities and
settings need a portfolio for the reasons
outlined in this article. The portfolio
should be started now if not
done already to avoid lost opportunities
to save documents for it. With so
many career opportunities avaiiaiiie
for nurses, the portfolio might be
needed at any time when the nurse is
pursuing a promotion in the clinical
setting, considering a new position in
the agency, or applying for a new position.
Once initiated, the portfolio can
then be maintained and reviewed
periodically to monitor growth and
development and to document progress
in meeting career goals.
References
Brooks, B.A., Barrett, S., & Zimmermann,
RG. (1998). Beyond your resume: A
nurse’s professional “portfolio.”
Juurnai of Emergency Nursing, 24, 555-
557.
Brooi
organize a professional portfolio for
staff and career development, journal
for Nurses in Staff Development, 15{1],
5-10.
English National Board (ENB) for Nursing,
Midwifery and Health Visiting. (1998).
The future of professional practice: The
UKCC’s .”Standards for education and
practice following registration. .Accessed
15 January 2001. Avai lable from http://
www,tjnb.org.uk/respspr’Ki26.htm.
Gaberson, K., & Oermann, M.H. (1999).
Clinical teaching strategies in nursing
education. New York: Springer.
Koch, L., Schultz, D., & Cusick,J. (1998).
Encouraging rehabilitation counseling
stude
G
Developing a Professional Portfolio in Nursing Sample Answer
Capstone Project: Developing a Professional Portfolio in Nursing
Professional portfolios are essential in nursing care as they help in the documentation of practices in which practitioners engage. Among the activities that nurses can document in their portfolios are those pertaining to their involvement in educative programs, community outreach, and professional organizations among others (Capan, Ambrose, Burkett, Evangelista, Flook, & Straka, 2013, Pg. 182). Portfolios serve as instruments of demonstrating developments from a professional perspective. As Hespenheider, Cottingham, and Muellar observed, portfolios are important in recognition and the rewarding of professionals who are excellent in their practice (2011, pg. 312). The growth and development portfolio as indicated in the case study offers nurses a chance to monitor their professional progress. With the portfolios, the healthcare practitioners can evaluate their attainment of both personal and professional goals. Also, the provisions within the portfolios ensure that while nurses can assess their own discoveries and knowledge acquisition, other people cannot review them. In its nature, the growth and development documentation allows for the viewing of the development of competencies within individuals. With the development in technology, nurses nowadays consider using portfolios that operate electronically. Green, Wyllie and Jackson wrote that electronic versions of portfolios allow nurses to stay more informed on current matters regarding healthcare (2014, Pg. 4).
Portfolios that focus on growth and development give nurses a chance to determine what they should share with others. Professionally, the portfolio can enhance development and may be used in considerations of job promotion among other serious situations. Within the professional sphere, the portfolios could also find use during evaluations and appraisals. With their varied applications, portfolios serve to satisfy both personal as well as professional requirements.
The development of a portfolio is done in a stepwise manner. To develop a portfolio, nursing professionals first assess themselves to understand their needs. After the understanding, they can then explore on the means of meeting the needs. As time progresses, nurses can then implement the plans they develop. Later, nurses can use the plan to evaluate their progress, and revise it so that it shows what they may feel necessary. Portfolios not only allow nurses to evaluate themselves, but they also enable them to make necessary plans for their professional well-being. Though portfolios are not meant to be the basis of determining the level of experience among nurses, they help in evaluating the extent in which the professionals get involved with matters pertaining to their practice.
My growth and Development Portfolio
Date
Year
Certification
March 4
2015
Received a certificate for participation in a wellness movement funded by the university’s nursing association
December 12
2014
Rewarded for heading a charity walk within the locality
August 10
2014
Promoted to be the chairperson of the health promotion association within the locality
May 19
2013
Joined a health promotion association within the locality
February 10
2013
Participated in a talk hosted by registered nurse practitioners in New York
January 1
2013
Recognized for actively participating in a strategy designed to educate the aged on healthy physical exercises
November 11
2012
Joined a local association that aimed at promoting the health of the aged
Venue
Date
Time
Meeting
Social welfare grounds
May 1 2015
1900hrs
Health welfare meeting
Addressing the entire community
Social welfare grounds
March 1 2015
1900hrs
Health welfare meeting
Addressing the young population
Community hall
January 1 2015
1800hrs
Health welfare meeting
Addressing the aged population
Community hall
November 1 2014
1800hrs
Health welfare meeting
Setting objectives
Developing a Professional Portfolio in Nursing References
Capan, M. L., Ambrose, H. L., Burkett, M., Evangelista, T. R., Flook, D. M., & Strake, K. L. (2013). Nursing portfolio study: the use in annual performance reviews. J Nurs Prof Dev, 29(4), 182-185
Green, J., Wyllie, A., & Jackson D. (2014). Electronic portfolios in nursing education: a review of the literature. Nurse du Prac, 14(1), 4-8
Hespenheider, M., Cottingham, T., & Muellar, G. (2011). Portfolio use as a tool to demonstrate professional development in advanced nursing practice. Clinic Nurs Spec, 25(6), 312-320
One of the reasons to assess a patient’s thoughts and beliefs about health and illness is to identify any patterns or beliefs that may affect his or her health and healing. How would past experience with cancer in another family member possibly impact a patient’s own health and healing if he/she was diagnosed with cancer? Choose one of AHNA’s core values (body, mind, emotions, spirit, social/cultural, relationship, context, and environment) and discuss how you can care for yourself in that area in order to improve well-being. Use examples from your clinical experience and cite sources from the readings or online library.
Prompt 2
From your clinical experience, provide two examples of healing rituals that your patients from different cultures have utilized to support their health and healing. Give a general description of the rituals including the type of ritual, who performed it, where and how often it was performed, and how the patient believed that it would help him or her to heal. Choose rituals from different cultures. Support your answer with sources from the readings or the online library.
AT LEAST 1 CITATION FOR EACH PROMPT
SAMPLE ANSWER
Holistic Nursing
ANHA outlines five core principles for holistic nursing including; holistic philosophy and ethics, caring process; communication which upholds cultural competency; research and nurse self-care as well as nurse reflection. For effective patient care in oncology, nurses must understand that self-care is important because it prevents burn out. In this context, I ensure that I have adequate time to nourish my mind, body and spirit. I take walk in the park to appreciate nature and to meditate at least twice a week. I also ensure that I surround myself with the right people. I ensure that my diet is balanced and always aim to sleep for at least six hours. This aims at nourishing my spirit, mind and body (Povlsen & Borup, 2011).
There are many rituals which have been practiced in order to improve health. For instance, Tea ceremony which is conducted by Buddhist leader is a ritual common in Hinduism. The patient must be present and awake when taking the tea. The person is only supposed to focus on the present activities such as warmth from the cup of tea, the aroma and sweetness of the delicacy. The tea has many ingredients which are important in herbal therapy, and its principles are based on meditation. This ceremony is done as often as possible. Smudging ceremony is performed to remove negative energy to help one start a new phase of life. It involves burning of sage, the smoke is believed to send away evil spirit and to bless the area. The activities include drumming and dancing to send evil spirit away. The event is conducted by a healer; it is done in the vicinity of the patient. It is recommended that it should be done regularly to scare demons. After these two rituals, the patients were contented and there was a massive improvement with chemotherapy (Richardson, 2012).
References
Povlsen, L., & Borup, I. (2011). Holism in nursing and health promotion: distinct or related perspectives? – A literature review. Scandinavian Journal Of Caring Sciences, 25(4), 798-805. doi:10.1111/j.1471-6712.2011.00885.x
Richardson, C. (2012). Witnessing Life Transitions with Ritual and Ceremony in Family Therapy: Three Examples from a Metis Therapist. Journal Of Systemic Therapies, 31(3), 68-78. https://www.doi:10.1521/jsyt.2012.31.3.68
We can write this or a similar paper for you! Simply fill the order form!
A strategic planning cycle is used when there is a health issue to be addressed and there are various methods available for addressing this issue. It aims at finding and implementing the most appropriate method that will last longer than any other method (Dunham-Taylor & Pinczuk, 2015, pg 555). The following are the concepts that affect the strategic planning cycle.
Involvement of the appropriate people
For an effective and strategic planning cycle, it is essential to involve an appropriate number of stakeholders. The number of participating members should also be a considerable and appropriate one. These members should also be relevant to the planning process. (Hood, 2013, pg 475)
Addressing of critical issues
A strategic planning cycle will require that all the critical issues are addressed before starting the planning cycle and during the process period so as to avoid the focusing on minor issues and ignoring the critical ones. This can be achieved through choosing a topic that is not too difficult for the members to comprehend and also choosing a manageable amount of issues. (Hood, 2013, pg 475)
Planning within an ethical time
The planning of the strategic planning process should be done within a framework of an appropriate time so as to ensure that enough amount of time is allocated to the implementation of the planning cycle. (Hood, 2013, pg 476)
Financial planning
An effective planning cycle will require adequate funding and this requires financial planning to be done before the starting of the planning cycle and the financial planning should not be done independent of the strategic planning. If this is not done then it is highly likely that the strategies may not be feasible (Penner, 2013, pg 54)
Flexibility of plans in relation to the dynamic environment
The plans set out in the strategic planning cycle should not be too rigid as it is required to encompass the dynamic changing environment so as to enable for the implementation of these plans. (Hood, 2013, pg 476)
Resistance to change
This can cause the derailment of the implementation of a critical issue thus it is important for any resistance to be addressed in a swift manner so as to avoid any effects that may be devastating. (Hood, 2013, pg 476)
In the strategic planning process, a nurse manager has important roles to play and these are as follows. (Roussel, 2013, pg 360)
Firstly, the nurse manager oversees the appropriate implementation of the financial planning that has been drafted for the strategic planning process.
Secondly, it is the work of the nurse manager to interpret the issues set out in the strategic planning concept to the other nurses and also prioritizes what might be seemed to be the most crucial issues. The nurse manager is also expected to oversee the addressing of these critical issues.
Thirdly, the nurse manager is expected to provide an environment that is conducive to the participating members of a strategic planning will work in during the implementation of the issues of the planning cycle. This works through continuous communication between the nurse manager and the participating members.
Fourthly, a nurse manager is required to choose the participating members of the health planning process. This is supposed to be done in a systematic manner so as to avoid the selecting of many or too few members or members who are irrelevant to the planning process.
Lastly, the nurse manager is expected to choose the method to be used in the planning process since strategic planning involves the choosing of an appropriate method out of a number of available methods to address a certain health issue.
References
In Dunham-Taylor, J., & In Pinczuk, J. Z. (2015). Financial management for nurse managers. Merging the heart with the dollar.
Hood, L. (2013). Leddy & Pepper’s conceptual bases of professional nursing. Lippincott, Williams & Wilkins.
Penner, S. J. (2013). Economics and financial management for nurses and nurse leaders. Springer Publishing Company.
Capstone Project
Legislative Changes for the Future
Directions:
You have been asked to address a group of the American Association for Retired Persons (AARP) about the roles that the following types of nurses can offer to adults over 50. In one role you are a Geriatric Nurse Specialist in another role you are a REGISTERED Nurse with a BSN.
Explain the difference in the two roles above and the potential impact of each of those roles could have on the health of seniors. Be sure to explain the NURSING role so that your lay audience can understand. You will want to cover the roles separately and what differences in the types of services each could offer.
Knowing the AARP is one of the most influential lobbying groups in the US, are there specific legislative agendas that you would like them to support in expanding the role of nurses?
SAMPLE ANSWER
Currently, it has been evident that the population of the elderly is growing faster as it has never been. It is now the responsibility of nurses and you the American Association for the retired persons (AARP) to assure these old people live long.In the care of this care of the aged you will encounter two categories of nurses.You should be able to differentiate between the two categoriesof nurses. Geriatric nurse specialists are nurses who have advanced knowledge elderly care. This group of nurses possess an extra education on the care of elderly people.
Roles of geriatric nurse specialist
They advocate for the elderly and educate the community against the myths related to old age.
They also act as clinical practitioners who entail assessing and identify problems.
These nurses do research pertaining the aged people.(Brinkman&any Widener University, 2013, Pg.85).
Those having a bachelor of science in nursing offer their services to the elderly just like to any other individual of age.
Differences between Geriatric nurse specialist and BSN nurses
Geriatric nurse specialists have carried out further studies specializing in care for old age people while BSN nurses only have a degree in nursing which Geriatric nurses also have.
Geriatric nurse specialists have management and leadership positions in elderly day health care centers while BSN nurses are their juniors.
They do researches on old age diseases while the BSN nurses do not.
Nurses have a great impact on the society. Their existence have increased the lifespan of the elderly people.
American Association of Retired Persons (AARP) should chip in to provide funds that will help in expanding services of these nurses. They should also inform the society about the import roles nurses play to the elderly. By doing this they will be giving credit to the nurses.
Reference
Brinkman, M. A., & Widener University. (2013). A focused ethnography: Experiences of registered nurses transitioning to the operating room.
Select an advanced professional or advanced practice nursing specialty. How has past and current regulation/legislation affected the role and scope of this nursing role? What, if any, discussions are currently underway relative to the scope and role of this specialty? What resources are available to assist nurses in advocating for these roles?
Select a professional or specialty nursing association. What impact has this organization had on health care legislation in the past 2 years?
This task is due 22nd may 2015\
SAMPLE ANSWER
Health Care: Ambulatory Care Nursing
This case focuses on ambulatory nursing, which significantly differs from other nursing specialties at the level of the scope of practice. Patient care demands change with time and adjustment in various practices in ambulatory nursing are vital. In most cases, the changes require allocation of more roles to nurses. As such, the scope of ambulatory nursing has expanded to improve patient care.
Both past and current regulations have affected ambulatory nursing from different perspectives. As Stokowski (2011) noted, the current views on ambulatory nursing are different from what used to be the understanding ten years ago. The earlier regulation allowed only a narrow scope for ambulatory nursing. Policy makers have made changes in the scope of the field to suit the current patient care requirements. Differences in health care setting have necessitated most of the changes. For instance, there are differences in the occurrence of chronic diseases, lengths of hospitalization, as well as the complexity of procedures performed on patients (Stokowski, 2011). With the new regulations, nurses can attend patients from other more different settings. They can attend patients from offices, community health facilities, homes, schools, and gastrointestinal laboratories among others (Stokowski, 2011).
There are discussions on ambulatory nursing that aim at defining the practice, and describing it in a comprehensive manner. In addition, there are discussions on relating the specialty to general practice as well as those on framework expansion. Stakeholders also address the standards of performance expected from the ambulatory nursing specialists.
To advocate for their roles, nurses use general practice as well as specialty associations. For instance, the American Academy of Ambulatory Care Nurses (AAACN) offers a platform on which nurses in the ambulatory field can discuss and express their opinions. Within the last two years, the AAACN has expressed that ambulatory nurses have a rich background in nursing and that they employ their knowledge to offer quality ambulatory services. In so doing, the association backs nurses in their practice.
Breaking the Chain: the Patient with a Communicable Disease Paper
Order Instructions:
he M6A4: Breaking the Chain: the Patient with a Communicable Disease Paper counts as 30% of your grade for this course.
We suggest that you develop and outline and use the following time-line as your guide for completing your paper:
Week 1: Review the requirements for the paper.
Week 2: Begin developing an outline for your paper.
Week 3: You should have your outline completed.
Week 4: You should be using your outline to write your paper.
Week 5: Continue work on your paper.
Week 6: Finalize your paper and submit by the end of the week.
Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page.
Information on using an outline and writing a scholarly paper is available through the Excelsior College Online Writing Lab (OWL).
If you have questions, reach out to your instructor via My Messages.
linked item M6A4: Breaking the Chain: Patient with a Communicable Disease Paper
The registered professional nurse plays an important role in infection control and prevention. The purpose of this written assignment is for you to apply your findings from evidence-based practice (professional nursing references) to a patient with an infectious and communicable disease.
Using APA format, write a six (6) to ten (10) page paper (excludes cover and reference page) that addresses the topic. A minimum of three (3) current professional references must be provided. Current references include professional publications or valid and current websites dated within five (5) years. Additionally, a textbook that is no more than one (1) edition old may be used.
The paper consists of two (2) parts and must be submitted by the close of week six (6). Each part must be a minimum of three (3) pages in length.
Choose one (1) of the following diseases:
Human Immunodeficiency Virus infection/Acquired
Immunodeficiency Syndrome (HIV/AIDS)
Hepatitis A
Hepatitis B
Hepatitis C
Pertussis
Tuberculosis
Part 1 – The Chain of Infection (minimum of three (3) pages)
Describe each of the six (6) elements in the chain of infection in terms of the disease you chose for this paper (infectious agent, reservoir, portal of exit, means of transmission, portal of entry, susceptible host). Provide supporting evidence, epidemiologic statistics, and pertinent laboratory data where appropriate.
Part 2 – Nursing Management (minimum of three (3) pages)
Identify treatment options utilized to break the chain of infection and prevent contagion for the disease you chose for this paper. Explore evidence-based practice nursing interventions when managing short-term and long-term consequences for the patient with the disease you chose for this paper. Consider and describe how the registered professional nurse would support patient adherence to these treatment options.
Compose your work using a word processor (or other software as appropriate) and save it frequently to your computer. Use a 12 font size, double space your work and use APA format for citations, references, and overall format. Information on how to use the Excelsior College Library to help you research and write your paper is available through the Library Help for AD Nursing Courses page. Assistance with APA format, grammar, and avoiding plagiarism is available for free through the Excelsior College Online Writing Lab (OWL). Be sure to check your work and correct any spelling or grammatical errors before you submit your assignment.
You are required to submit your paper to Turnitin (a plagiarism prevention service) prior to submitting the paper in the course submission area for grading. Access is provided by email to the email address on record in your MyExcelsior account during week 2 of the term. Once you submit your paper to Turnitin check your inbox in Turnitin for the results. After viewing your originality report correct the areas of your paper that warrant attention. You can re-submit your paper to Turnitin after 24-hours and continue to re-submit until the results are acceptable. Acceptable ranges include a cumulative total of less than 15% for your entire paper, and no particular area greater than 2% (excluding direct quotes and/or references).
SAMPLE ANSWER
Patient with a Communicable Disease
Human immunodeficiency virus infection/ Acquired Immunodeficiency Syndrome (HIV/AIDS) is the number one infectious killer in the world with reported 39 million deaths since the first cases were reported in 1981.The majority of people living with this disease leave in low-income and middle-income countries. (Organization, 2014, pg 16) The following report is about the HIV/AIDS and it is divided into two parts.
The first part is meant to look at the chain of infection of the disease.
Infectious agent
The infectious agent for HIV/AIDS is the human immune deficiency virus (HIV). This virus has a single strand, positive sense and the RNA virus enveloped in the genus Lentivirus .For the infection to occur, a significant amount and concentration of the virus must be present. Once in the body the virus affects one’s immune system this is through destroying a special type of cells called the T helper lymphocytes (T-cells). The T-cells are crucial in the functioning of the immune system and the immune response.HIV then replicates itself over a number of times and eventually outnumbers the number of T-cells. (Lala & Merchant, 2012, pg 39)
Reservoir
The virus leaves in the human blood or other body fluids of the infected person. In the blood the virus stays in blood cells whereby it is usually able to remain hidden within the cells. The cells after time adapt the HIV genetic code and remain invisible to the immune defense mechanisms of the body and become insensitive to the drugs. (Lala & Merchant, 2012, pg 39)
Portal of exit
The HIV leaves the body of the infected person to the body of another person through the following mediums.
Firstly, it can be through the infected blood that is if the blood of the infected person comes into contact with the blood of another person. The blood contact can occur through a number of ways for example, through blood transmission, sharing of syringes and through the transplantation of body organs and tissues with an infected person.
Secondly, it can be through the semen and other vaginal secretions. This usually occurs when an infected person has unprotected sex with another person.
Thirdly, it can be through breast milk whereby an infected mother breast feeds a baby.
Statistics show that the concentration of HIV is usually high in the blood followed by the semen and vaginal secretions then the breast milk. (Hall, Hall & Cockerell, 2011, pg 57)
Means of transmission
Transmission usually occurs when there is an interaction between the blood or body fluids of two people and one of them is infected with the virus. There a number of ways through which the infection can be transmitted and this is as follows.
Firstly, it can be through unprotected sexual contact with an infected person and this is usually transmitted through the semen, blood or vaginal secretions. Sexual intercourse can either be through penile, vaginal or rectal tissues. The risk to acquire the infection through this means of transmission usually depends on: the number of sexual partners, one has, the infection prevalence among these partners and lastly the probability of the transmission of the virus during sexual intercourse. Apart from sexual intercourse the virus can also be transmitted through deep kissing.
Secondly, it can be through the direct injection of with syringes and needles which contains HIV infected blood or blood products. This means of transmission has usually been found to be common among drug users who share such needles and syringes when using drugs such as cocaine.
Thirdly, it can be transmitted from a HIV-infected mother to the baby and this is usually through two main ways. Firstly, it can be during the process giving birth. Secondly, an infected mother can transmit the virus to the baby through breastfeeding. This occurs although, the concentration of the virus in the breast milk is minimum because the immune system of a newborn baby is usually very week.
Fourthly, the transmission can be through the transfusion of blood from an infected person to another person. The same can also be transmitted through the transplant of body organs and tissues from an infected person (Hall, Hall & Cockerell, 2011, pg 63)
Portal of entry
There are three main ways through which the HIV can enter into the body of a healthy person. For the virus to enter into the body of a healthy person, the number of the virus must be adequate to cause the infection.
Firstly, the main means of entry of the virus is usually through the blood. This occurs when the blood from an infected person comes into direct contact with the blood of another person for example, sharing of syringes with an infected person. The entry can also be through semen, for example, during sexual contact.
Secondly, the entry can be through semen and vaginal secretions. This usually occurs during sexual contact for example, unprotected sex.
Lastly, the entry can be through the skin membrane which occurs when the membrane is splashed with a body fluid from an infected person. It has been shown that the entry of the virus through this means is usually rare and accounts for less than 1% risk of infection. (Lala & Merchant, 2012, pg 41)
Susceptible host
Any person whose blood or body fluids come into contact with HIV infected blood or body fluids can become infected with the same disease. Statistics show that the people who usually have unprotected sex with a number of different people are at the highest risk of contracting HIV/AIDS. In 2013, an approximated 35 million people worldwide were living with HIV/AIDS. Out of this population, children under the age of 15 years were 240,000. (Organization, 2014, pg 16)
The second part is meant to look at the treatment options that can be used to break down the chain of infection and prevent contagion for the disease, explore evidence based practice nursing interventions when managing short-term and long term consequences for the patients suffering from the disease and describe how a registered professional nurse can support patient adherence to the treatment options.
Treatment options utilized to prevent transmission of HIV
The main treatment use to break down the chain of infection of the disease and prevent contagion is the antiretroviral treatment (ART). The treatment usually works through minimizing the number of microorganisms (HIV) in the blood, semen, vaginal and rectal fluid to an undetectable number. There are a number of options in using this treatment and this is as follows:
Treatment can be given to infected pregnant mothers and a newborn baby so at to prevent transmission through the mother to child infection. The pregnant mother and the baby is given zidovudine (AZT). It has been shown that this treatment has been able to reduce the mother to child prevention from 25% to 8%. Infected mothers using Antiretroviral drugs (ARVs) have also been found to reduce the risk of a mother to transmit the disease while breastfeeding.
The other treatment option used is the Pre-exposure prophylaxis (PrEP). This treatment usually works through people who are HIV-negative using ARV drugs before being exposed to HIV. This treatment has been showed to reduce the risk of the disease up to 92%.
Post-exposure prophylaxis treatment is also used although it is a short term treatment It usually involves using the ARV after being exposed to the virus. Initially, this treatment was used by health workers who had been exposed to infected fluids. Recently, treatment has been used on those who might have been exposed in only one event for example, in cases of sexual assault (Sachdeva & Dutta, 2012, 377)
Evidenced based practice nursing interventions
There are two types of nursing interventions based on whether the consequences are short-term or long-term.
For the long-term consequences, the following nursing interventions would be necessary;
Firstly there is the recommending of the patient to guidance and counseling sessions so as to boost their morale. This will be very useful when it comes to taking the treatment since the patient would now be able to positively appreciating the disease.
Secondly, there would be need to subject the patient to HIV/AIDS awareness education and this is so as to minimize the risk of the patient in transmitting the disease to other people.
Thirdly, the infected person should be supplied with sex protection such as condoms so as to reduce the risk of one infecting his/her spouse. There is also need of counseling the spouse of an infected person and this is also aimed at reducing the risk of infection to the spouse.
Lastly, there is the need of making the patient to appreciate the importance of the treatment that is prescribed to him/her and ensure that the patient adheres to the treatment as prescribed.
As for the short term consequences, the following interventions would be necessary;
Firstly, the nurse can conduct once in a while visits to the patient’s home so as to ensure that the patient is using drugs as prescribed.
Secondly, the nurse can prescribe preferable nutrition to the patient that will ensure that the immune system of the patient is properly working so as to prevent the patient from being infected with other diseases which are related to HIV/AIDS such as Tuberculosis (TB).
Lastly, the nurse could ensure that he/she has the contacts of the close family of the infected person and this is to help in case of any emergency or any other problem (J & S, 2012, pg 690).
Supporting of the patients to adhere to the treatments
There are a number of ways through which a registered professional nurse would support patients in the adherence to the treatment options. Some of these ways are as follows.
The nurse can conduct some guidance and counseling sessions on the patient. During these sessions, the nurse could explain to the patient the importance of adhering to the treatment and also remember to explain to the patient the danger of not taking the treatment.
The nurse can carry out some follow-up on patients. This can be achieved in a number of ways for example, through carrying out of routine visits to the home of the patient so as to ensure that the patient adheres to the treatment.
A professional nurse can keep in touch with the close family of an infected person; the importance is so as to make sure that the patient uses the prescribed treatment. The nurse has to make sure that he/she has explained to the family the importance of the infected person to take the treatment and also remember to explain to this family the danger of the patient in failing to take the treatment. (M, C & M, 2012, pg. 904). In conclusion, although HIV/AIDS has no cure it can easily be prevented once its chain of infection has been understood.
References
Organization, W. H. (2014). World Health Statistics 2014. Geneva: World Health Organization.
Lala, M. M. & Merchant, R. H. (2012). Principles of perinatal and pediatric HIV/AIDS. New Delhi. Jaypee Brothers Medical Publishers.