Essay is on Propaganda in world war one: I will send you photos of what you have to do. please read this CAREFULLY.
1. Make sure you make up 10 questions and on the page put them in bullet point and explain them all. Example: 1.How did propaganda affect the war? blah blah blah 2. Did propaganda help bolster the army? blah blah blah etc…
2. You have to do a website evaluation: the information on that will be on one of the photos i will send you. look at out for it. ITS THE ONE THAT SAYS
WEBSITE EVALUATION and follow what it says to do i.e: Bibliographical details, Information about author, Summary of website, Quotes and then how useful it
was for the investigation.
3. You need to do a research task and this links back to the questions. You need to refer back to the questions and then answer them in notes from different sources. You need to get some notes from actual books, 2 sets of notes to be exact from books, the other notes need to be on the internet. one again do this in bullet point form. you will see what the page looks like when i send the photo to you. THE PAGE IS THE ONE THAT SAYS NOTES- WITH PAGE REFERENCE WITH SOURCE TO THE LEFT OF THAT. MAKE SURE YOU PUT THE WEBSITES OR BOOKS YOU USED OVER THE TOP OF THE SET OF NOTES AND USE THE HARVARD SYSTEM FOR THE
BIBLIOGRAPHY. Make sure the notes are like this:
Website/book:
Notes
For the next one repeat but with another book or website
Website/book:
Notes
*Make sure you are using the Harvard system bibliography way.
4. Do a 200 word reflection on how the project went: What topic did i choose? why did i choose this topic? what did I learn? etc…
We can write this or a similar paper for you! Simply fill the order form!
Every bit of information must be cited
must also write a treatment plan with 2 long term goals and 2 short term goals for each of the long term goals and 2 interventions for each short term goal.
USE PEER REVIEWED SOURCES AND SCHOLARLY SOURCES FOR ACCURATE INFORMATION AND WELL RESEARCHED ASSIGNMENTS FOR VALIDITY.
Review the grading rubric on turntin to avoid penalization which will lead to low grades.
We can write this or a similar paper for you! Simply fill the order form!
This is scientific reports about (ultra heat treatment of milk) have to be Your 2500 word report, prepared using the Template file from should be structured as follows:
Appropriate illustrative mater use intent referencing (name and date),, EMBO Journal references in references list if you can use 6 or 8 journals or more, and 3 or 5 books that should be fine so there are no specific number of references.
We can write this or a similar paper for you! Simply fill the order form!
In 1965, Sir Austin Bradford Hill proposed guidelines for assessing causality. His intention was not for these to be used in a rigid manner but rather to be used as a guide.
For this Application Assignment, review your resources on Hill’s guidelines for causality. Then find a review journal article dealing with an association where causality is hypothesized based on an assessment of the body of literature on a topic. Analyze this article using Hill’s guidelines. Then respond to the following questions:
•Does the article use Hill’s guidelines to determine causality?
•If so, are they each addressed thoroughly?
•If not, describe the alternative means used for assessing causality.
•How well do you believe Hill’s guidelines work as a tool for determining causality for the association your review article addresses?
SAMPLE ANSWER
Assessing Causality
Hill’s Criteria of Causation basically delineates the minimal condition that is required to ascertain a causal relationship between 2 items. Sir Austin Bradford Hill originally presented these criteria as a method that can be utilized to determine the causal link between a given factor, for instance tobacco use, and an ill health, like lung cancer or emphysema (Doll, 2010). The criteria forms the starting point of contemporary epidemiological research that tries to find out scientifically valid causal links between possible disease agents and the multiple sicknesses which afflict people (Crislip, 2010). The criteria are nine. (i) Strength of the association: undoubtedly, if condition Y brings about outcome Z, then it has to be that Y and Z can be demonstrably related with each other. Simply put, the association should be sufficiently strong to be considered as clinically significant by the person reading the argument (Van Reekum, Streiner & Conn, 2009). (ii) Consistency of the evidence: if Y causes Z, then one should expect that evidence that supports this relationship would actually be found consistently (Crislip, 2010).
(iii) Specificity: given that illnesses could have different etiologies as well as therapies, this criteria is weaker. (iv) Temporal sequence: without a doubt, if Y causes Z, then Y must necessarily occur before Z. This is an essential criterion used to establish a causation argument (Crislip, 2010). (v) Biological gradient or dose-response: a large exposure has to result in a large effect, and a little exposure has to cause little effect. (vi) Biological rationale or plausibility: there is a higher chance of a causative relationship being present if it actually makes biological sense that Y results in Z. The association is in agreement with presently accepted understanding of pathological processes (Susser, 2008). (vii) Coherence: there is a higher probability that Y results in Z if this assumed causal relationship is similar to what is already known regarding the disorder or sickness. (viii) Experimental evidence: the health condition could be improved or prevented by a suitable experimental regimen. (ix) Analogous evidence: this criterion basically takes the form of supposing that if some condition which is the same as Y brings about an outcome the same as Z, then this is evidence that Z is caused by Y (Crislip, 2010; Doll, 2010).
Van Reekum, R., Cohen, T., & Wong, J. (2000). Can Traumatic Brain Injury Cause Psychiatric Disorders? The Journal of Neuropsychiatry and Clinical Neurosciences. 12:316-327. https://www.doi:10.1176/appi.neuropsych.12.2.316
Van Reekum et al. (2000) reviewed the evidence in supporting the argument that Traumatic Brain Injury (TBI) might result in psychiatric disorders and they employed the structure presented by some of Hill’s most pertinent criteria with the aim of critically examining the strength of this argument. The article uses some of Hill’s guidelines in determining causality. Not all of the criteria are addressed thoroughly.
In the article, Van Reekum et al. (2000) presented consistent evidence of an association between traumatic brain injury and several disorders from many studies. Nonetheless, most of this research was in fact narrowed to naturalistic follow-up studies. Not any of the studies used pre-TBI – prospective – psychiatric evaluations, so that the evidence for the apt temporal sequence was limited. Retrospective psychiatric evaluations suggested that nearly all of the psychiatric disorders start for the first time after traumatic brain injury. There is little evidence in the article of biological gradient for psychiatric disorders after traumatic brain injury in adults. This suggests either that presently available approaches to measuring the severity of traumatic brain injury are insufficient or, on the other hand, that traumatic brain injury increases the risk of psychiatric disorders notwithstanding the TBI severity (Van Reekum et al., 2000). There was substantial evidence supporting a biologic rationale that is in fact cohesive with the existing, modern knowledge; it has been found that traumatic brain injury actually disrupts neuronal systems that underlie behavior and mood (Van Reekum, Streiner & Conn, 2009). The other causal factors to psychiatric disorders post traumatic brain injury were also preliminarily recognized, for instance the existence of pre-TBI psychiatric disorders in some instances.
Hill’s guidelines are very effective as a tool for determining causality for the association that the article review addresses. In essence, Hill’s guidelines in reviewing the evidence for the argument of causation presented by Van Reekum et al. (2000) was useful for several reasons. The structure provided by the guidelines allowed for systematic review of every available evidence and to find its place within the argument. It is of note that where the data were not consistent with the causation argument, this served to encourage the creation of new hypotheses, for instance the lack of a biological gradient indicated that traumatic brain injury of even mild seriousness can be able to disrupt neuronal circuits that underlie psychiatric disorders. Using the guidelines emphasized the methodological drawbacks in future research. Moreover, using the guideline permitted the review to move further than the ascertainment of a simple connection between psychiatric disorders and TBI by encouraging consideration of extra criteria which support the argument.
References
Crislip, M. (2010). Causation and Hill’s Criteria. Boca Raton, Fl: CRC Press.
Doll, R. (2010). Sir Austin Bradford Hill and the Progress of Medical Science. British Medical Journal, 305: 1521-1526
Susser, M. (2008). Judgment and Causal Inference: Criteria in Epidemiologic Studies. American Journal of Epidemiology, 105:1-15
Van Reekum, R., Cohen, T., & Wong, J. (2000). Can Traumatic Brain Injury Cause Psychiatric Disorders? The Journal of Neuropsychiatry and Clinical Neurosciences. 12:316-327. http://www.doi:10.1176/appi.neuropsych.12.2.316
Van Reekum, R., Streiner, D. L., & Conn, D. K. (2009). Applying Bradford Hill’s Criteria for Causation to Neuropsychiatry: Challenges and Opportunities. J Neuropsychiatry Clin Neurosci,13(3).
We can write this or a similar paper for you! Simply fill the order form!
Use at least three (3) quality references Note: Wikipedia and other related websites do not qualify as academic resources.
Your assignment must follow these formatting requirements:
Be typed, double spaced, using Times New Roman font (size 12), with one-inch margins on all sides; citations and references must follow APA or school-specific format. Check with your professor for any additional instructions.
Include a cover page containing the title of the assignment, the student’s name, the professor’s name, the course title, and the date. The cover page and the reference page are not included in the required assignment page length.
We can write this or a similar paper for you! Simply fill the order form!
The critique of an epidemiologic study involves an assessment of the methods of data collection (which includes the type of study design), the analysis of the data and the interpretation of the data. For this application you are to read the following case control research article. After reading the article, complete the Case Control Template is below
•Lamontagne, F., Garant, M., Carvalho, J., Lanthier, L., Smieja, M., & Pilon, D. (2008). Pneumococcal vaccination and risk of myocardial infarction. Canadian Medical Association Journal, 179(8), 773-777.
Use the Academic Search Premier database, and search using the article’s Accession Number: 34526279
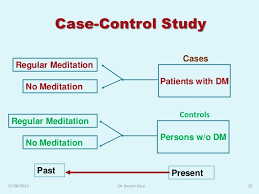
Case-Control Study
Submitted By (make sure your name and date are included here):
Article Citation in APA format:
Research Question:
Health Outcome of Interest:
Exposure(s) of Interest:
Diagnostic Criteria for Cases:
Case Ascertainment (include whether this was a single site or multi-site study):
Number of Cases (include information, if available, about the number who participated and the number who refused; indicate whether any information was provided about those who refused to participate):
Control Population (type/number/selection):
Type(s)/Method(s) of Data Collection (e.g. questionnaire, medical records, whether or not there was any procedure for validating some or the data):
Type of Data Analysis:
Results/Main Findings of Study:
Assessment of Bias (selection/information):
Assessment of Confounders:
Comments:
SAMPLE ANSWER
Case-Control Study
Article Citation in APA format: Lamontagne, F., Garant, M., Carvalho, J., Lanthier, L., Smieja, M., & Pilon, D. (2008). Pneumococcal Vaccination and Risk of Myocardial Infarction. Canadian Medical Association Journal, 179(8), 773-777.
Research Question/Hypothesis: in this article, the research question for the case study is not stated. However, the hypothesis is specified. The hypothesis was that: pneumococcal vaccination will be able to protect patients from myocardial infarction.
Health Outcome of Interest: patients being free from myocardial infarction
Exposure(s) of Interest: the authors regarded patients to have had the exposure to pneumococcal polysaccharide vaccine if these patients had been given this vaccine within the ten years prior to the index date, as documented in the Logivac database. Exposure was stratified by the interval between vaccination and index data (Lamontagne et al., 2008).
Diagnostic Criteria for Cases: patients who took part are those who were considered to be at high risk of having myocardial infarction, and had been admitted at the health care organization between 1/1/1997 and 12/31/2003. The risk for myocardial infarction is defined as the presence of diabetes; hypertension; or dyslipidemia in women aged over 50 years and in men aged over 45 years (Lamontagne et al., 2008; Lachaine, Rinfret & Merikle, 2006).
Case Ascertainment (include whether this was a single site or multi-site study): this was a single site study given that the authors carried out a case-control study of patients at risk of myocardial infarction, and these patients had been admitted at only one healthcare organization, which was a tertiary care hospital in Quebec, Canada.
Number of Cases (include information, if available, about the number who participated and the number who refused; indicate whether any information was provided about those who refused to participate):
There were 999 cases. The cases, according to the authors, were less likely compared to controls to have been vaccinated. The cases were matched according to sex, age, as well as year of hospitalization. For cases, the authors considered the admittance date for myocardial infarction to be the date of index (Lamontagne et al., 2008). No information is provided about the participants who refused to participate.
Control Population (type/number/selection): there were 3,996 controls in this study who were matched according to sex, age, as well as year of hospital admission. Controls were defined as patients who had 1 or more of the described risk factors as stated in the medical record, and had not been earlier diagnosed with atherosclerotic disease, and who never experienced a new myocardial infarction all through the study period. The authors only included those patients who had been admitted to the surgical departments of the hospital. For the controls, the authors considered the admission date into one of the departments as the index date. Four controls were matched to every case basing on sex; index, within 12 months; and age, within 24 months (Lamontagne et al., 2008).
Type(s)/Method(s) of Data Collection (e.g. questionnaire, medical records, whether or not there was any procedure for validating some or the data):
Data was collected through the use of medical records. Two sources of data collection were used. The first one was the research-purpose database of the hospital. This database, besides demographic data, comprised, for every hospital administration from the year 1996, complete information on all secondary and primary diagnoses, which were coded appropriate to the International Classification of Diseases, version 9. Logivac database was also utilized; a database that is maintained by the government and records all pneumococcal vaccination that have been administered in Quebec (Grayston, Kronmal & Jackson, 2005; Hansson, 2005).
Type of Data Analysis: The authors performed statistical analysis in which they estimated exposure to the pneumococcal polysaccharide vaccine at 20 percent. The authors utilized conditional logistic regression in estimating adjusted OR and 95 percent CI for new myocardial infarctions in relation to receiving of the pneumococcal polysaccharide vaccine. They performed both multivariable and univariable analyses and several covariables were incorporated. For all analyses, the authors matched controls and cases by index date, sex and age (Lamontagne et al., 2008).
Results/Main Findings of Study: Compared to controls, cases had a less likelihood of having been vaccinated – 95 percent confidence level 0.40-0.70, adjusted odds ration 0.53. The putative protective role of the pneumococcal polysaccharide vaccine was not noticed for patients who had been administered with the vaccine up to 12 months prior to the myocardial infarction. On the contrary, if vaccination had been administered 24 months or more prior to the hospital admission, then the association was stronger (Lamontagne et al., 2008).
Assessment of Bias (selection/information): At 3,999, the number of controls who were selected to take part in the study was considerably high compared to the cases, who were just 999.
Assessment of Confounders: After several modifying and confounding variables were considered, the findings showed that the chances of having received a vaccination within the group who had experienced myocardial infarction was roughly ½ that within the control group. In this study, there might have been residual confounding. It is of note that other cardiovascular risk factors including medication use, tobacco use, obesity, and lifestyle factors for instance exercise and diet could not be included in the model given that these traits are not documented within the research database (Lamontagne et al., 2008).
Comments: the study is of major importance since it demonstrates that there is an effect of pneumococcal vaccination in decreasing the incidents of new myocardial infarction. Nonetheless, the population of this study was restricted to only one hospital comprising largely Caucasian males. As such, future study should incorporate participants from other demographics and from multiple sites.
References
Grayston, J. T., Kronmal, R. A., & Jackson, L. A. (2005). Azithromycin for the Secondary Prevention of Coronary Events. N Engl J Med 2005;352:1637-45.
Hansson, G. K. (2005). Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med, 352:1685-95
Lachaine, J., Rinfret, S., & Merikle, E. P. (2006). Persistence and Adherence to Cholesterol Lowering Agents: Evidence from Régie de l’assurance maladie du Québec data. Am Heart J 2006;152:164-9.
Role of p-values and confidence intervals within epidemiological research
Order Instructions:
Week 6
Epidemiologists control for variables such as confounding and random error by carefully developing research studies. Although there are not guarantees to eliminate or reduce all possible errors, it is important to minimize their effects.
For this Discussion, review your readings from this week. Then addressing the following:
•
• Identify the role of p-values and confidence intervals within epidemiological research and provide examples of how these are used to interpret research findings.
•
• Discuss the effect sample size has on p-values and confidence intervals and how this affects interpretation of statistical results.
SAMPLE ANSWER
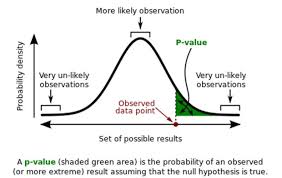
Role of p-values and confidence intervals
Confidence intervals and p-values are reported in almost every epidemiological research and are used in interpreting statistical analysis results. These measures are used by medical investigators and researchers to answer such questions as: “are the results significant?” or “is the hypothesis accepted?” Epidemiological researchers do not have to worry about testing the significance of results when carrying out statistical researches because they can depend on the p-value and the confidence interval. The p-value is the probability of a value that is similarly extreme or even more extreme as the one in the study if the hypothesis is true. Confidence interval on the other hand can be defined as is an array of values within which there is reasonable confidence that the parameter of the population lies. The reporting of confidence intervals and p-values basically follows that testing of hypothesis or significance, (Bland & Peacock, 2012).
For instance, when testing a hypothesis using the p-value, the particular cutoff or level of significance (conventionally 0.05) is used to test whether values are significant or not; those less are significant, while those above are not. For instance in the study of differences in low birth weight prevalence between singletons and multiple pregnancies, the p value can be used to “endorse” the hypothesis that there is a difference. For the confidence interval, consider a test for difference in mean sugar reduction between a standard hypoglycemic and a new drug. The null hypothesis in this case should state that there is no difference in the blood sugar reduction mean; that can be accepted or rejected, (Gardner& Altman, 2013).
P-values and confidence intervals tend to decrease in size with an increase in sample size unless the null hypothesis is true. As the sample size increases, for the case of the p-value, there is an increased certainty on where the proportion mean might be, and hence large samples are more consistent with smaller ranges of possible population values. For the confidence interval, a larger sample size means a decreased error margin. The effect this has on interpretation of results is that larger samples report small marginal errors and the certainty of finding the true population parameter increases, hence the certainty of the results increases too, (Houle, 2007).
References
Bland M, Peacock J. (2012). Interpreting statistics with confidence. The Obstetrician and Gynaecologist;4:176–180
Gardner MJ, Altman DG. (2013). Confidence intervals rather than P-values: estimation rather than hypothesis testing. Br Med J. 292:746–750
When conducting research, your design and methods are developed around what you are trying to find or assess. Different research methods are used to answer and address different types of questions. In epidemiology, there are multiple forms of research studies and as a public health official, it is important for you to understand when it is best to use these different types of research.
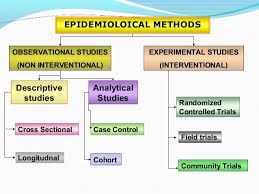
For this discussion, review the different types of epidemiology study designs listed in Table 6-1 on page 141.
Then address the following:
•Pick three epidemiological study designs to discuss. Summarize their main characteristics and discuss at least one strength and one limitation of each study design you select.
•Discuss which measure of association is most appropriate for each of the three study designs you’ve selected and why
We can write this or a similar paper for you! Simply fill the order form!
For this application you are to read the following cohort study article. After reading the article, complete the Cohort Study Template is below.
•Beelen, R., Hoek, G., Van Den Brandt, P., Goldbohm, R., Fischer, P., Schouten, L., et al. (2008). Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR Study). Environmental Health Perspectives, 116(2), 196-202.
Use the Academic Search Premier database, and search using the article’s Accession Number: 31169911
Cohort Study
Submitted By (make sure your name and date are included here):
Article Citation in APA format:
Research Question:
Health Outcome of Interest:
Exposure(s) of Interest:
Type of Study (please indicate whether this is a prospective (concurrent) or retrospective (non-concurrent) or ambidirectional study:
Type, Frequency and Duration of Follow-Up (indicate something about loss to follow-up and any efforts that were made to minimize loss to follow-up and include information on the characteristics of those who were lost to follow-up and comment on why this is important):
Type of Data Analysis (include measure of association used):
Results/Main Findings of Study:
Assessment of Bias (selection and information):
Assessment of Confounders:
Comments:
SAMPLE ANSWER
Cohort Studies
Article Citation: Beelen, R., Hoek, G., Van Den Brandt, P., Goldbohm, R., Fischer, P., Schouten, L., et al. (2008). Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR Study). Environmental Health Perspectives, 116(2), 196-202.
Research Question: what is the association between mortality and continuing exposure to traffic-related air pollution?
Health Outcome of Interest: decreased respiratory mortality by reducing exposure to ambient air pollution
Exposure(s) of Interest: long-term exposure to traffic-related air pollution. In essence, exposure to sulfur dioxide (SO2), nitrogen dioxide (NO2), black smoke (BS), particulate matter (PM) in addition to a variety of exposure variables to traffic comprised the exposures of interest in the study which were estimated at the home address (Beelen et al., 2008).
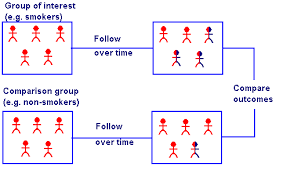
Type of Study: this is a prospective cohort study. In essence, a prospective cohort study is understood as a study in which the effects of a given variable are plotted over time, and the research study becomes a continuing and long-term process (Gehring et al., 2006). This cohort study is prospective given that it fits the definition of prospective; it was initiated in the year 1986, and the authors assessed mortality between 1/1/1987 and 31/12/1996, meaning that it was an ongoing process.
Description/Ascertainment of Cohort: the Netherlands Cohort Study on Diet and Cancer was started with enrolling 120,852 subjects that consisted of 62,573 women and 58,279 men aged between 55 years to 69 years, who lived in 204 municipalities all through the nation (Beelen et al., 2008).
Data Collection at Baseline: Baseline questionnaire was used to collect data. At baseline, every subject filled out an 11-page questionnaire on nutritional habits, as well as other factors for cancer. For every subject, data obtained from one page of the questionnaire were entered at baseline – with information pertaining to smoking status, sex, and age.
Type, Frequency and Duration of Follow-Up: After recruitment of the subjects, all of them were followed up for cancer incidence by record linkage to registries of cancer. The authors assessed mortality between January 1st 1987 and December 31st 1996, meaning that the participants were actually followed from the year 1987 to the year 1996; a period of 10 years. The authors have not stated anything about loss of follow-up as well as any efforts that were made to reduce loss to follow-up. The authors estimated exposure to nitrogen dioxide, particulate matter, black smoke and other traffic-related air pollutants at the home address of the subjects.
Type of Data Analysis: the authors analyzed the effects of air pollution for overall concentrations, and a mixture of background concentrations and traffic variables for the purpose of identifying effects of living close to busy highways separately. They calculated relative risks for concentrations and traffic variable dissimilarities between the 95th and 5th percentiles of the distributions (Beelen et al., 2008). The authors performed Cox analyses in the entire cohort with the use of Cox proportional hazards models. They computed person-years for every subject from baseline until end of follow-up or death. The authors adjusted for smoking, sex, age, as well as area-level. Cox-Poisson random effects survival software was used in incorporating spatial clustering at the neighborhood and/or municipal scale in the entire cohort analyses (Beelen et al., 2008).
Results/Main Findings of Study: the intensity of traffic on the closest road was independently linked to mortality. Relative risks at 95 percent CI for a 10-µg/m3 rise in the concentrations of black smoke – difference between 95th and 5th percentile – were 1.05 for natural cause, 1.03 for lung cancer, 1.22 for respiratory, 1.04 for cardiovascular, and 1.04 for mortality besides lung cancer, respiratory, or cardiovascular. The results were the same for PM2.5 and NO2, but there was no association for SO2 and mortality
Assessment of Bias: The authors selected subjects who were living near busy roads in 204 municipalities across the Netherlands. Those who lived far from busy highways were not chosen.
Assessment of Confounders: analysis in the case-cohort sample illustrated little distinction between the effect estimates adjusted for every confounder and adjusted for only the narrow set of confounders that were available in the entire cohort. The effect estimates were not sensitive to dissimilar models of confounders for both the case cohort and full cohort analyses.
Comments: The study is of major importance in contributing to the evidence that continuing and lasting exposure to traffic-related air pollution is linked to increased mortality. This is because traffic-related air pollution in addition to other traffic exposure variables were found to have an association with mortality in the cohort
Gehring, U., Heinrich, J., Kramer, U., Grote, V., Hochadel, M., Sugiri, D. (2006). Long-term Exposure to Ambient Air Pollution and Cardiopulmonary Mortality in Women. Epidemiology. 17:545–651.
We can write this or a similar paper for you! Simply fill the order form!
Write and essay about Road sharing between bicyclists and motorists, advantages and inconvenient. It should be elaborate using proper grammatical terms.
SAMPLE ANSWER
Advantages and Inconvenience of Road Sharing
Different countries and states have different laws pertaining to how cyclists and motorists should share roads to ensure safety. Both the cyclists as well as motorists have a right to use the roads to move from point A to B. This discussion investigates on the advantages and inconveniences of road sharing between the motorists and cyclists.
A number of advantages exist when bicyclists and motorists share the same road. One of them is that it helps to improve the level of maturity of the drivers and bicyclists as drivers and riders become more careful. The level of responsible driving is improved because drivers are required to drive safely putting into consideration the lives of riders (Commute Orlando.com. 2014). Therefore, a sense of responsibility tends to improve. Another advantage is that the cyclists get to enjoy their rights especially those that ride as a hobby as well those that use bicycles as means of their transport. The level of pollution as a result of emissions from motorists reduce to some levels promoting a healthy environment.
On the other hand, sharing road between cyclists and motorists has a number of inconveniences. One of the inconveniences is increased conflict between the drivers and riders. It becomes a challenge for many riders and drivers specially when turning, and crossing roads and during traffic jams (Commute Orlando.com. 2014). The rate of accidents are likely to increase as most of the times drivers disregard motorists. Some drivers have a mentality that cyclists are not supposed to use roads and this contributes to injuries and accidents. Furthermore, sharing of road between the motorists and bicyclists increase instances of traffic jams especially in urban centers. The motorists in such instances may end up spending more time on roads, which affects their productivity.
In conclusion, even though bicyclists and motorists are required to share roads, both must respect each other. The advantage of road sharing is that it improves the level of carefulness, which may help to reduce accidents as everyone becomes responsible. However, sharing roads causes inconveniences such as delays and increases risks of injuries and accidents