select only one (1) of the case studies provided :
• Remember this is an essay and should be structured as such with an introduction body and conclusion. Do not simply answer the questions provided, these are given as a guide. You will be expected to use research or evidence-based journal articles, textbooks and appropriate authoritative web sites (not Better Health Channel, Virtual Hospital, etc.).
• All referencing is to be formatted using the APA referencing style. Please ensure carefully to follow the marking criteria
SAMPLE ANSWER
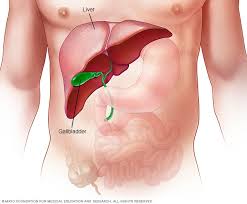
Liver disease
Introduction
Alcohol is a hepatotoxic compound that is commonly consumed across the globe. It is linked to a broad range of liver associated injury, ranging from simple steatosis, fibrosis to cirrhosis (Torruellas, French, & Medici, 2014). Alcohol liver disease refers to a spectrum of alcohol-related injuries that are potentially reversible especially when the progression of the disease is detected early enough. Therefore, regular screening and early diagnosis are essential. Excessive alcohol consumption adversely affects the health of an individual and is one of the primary causes of death in the world. Harmful or excessive use of alcohol results in a mortality rate of up to 2.5 million and an approximate disability of adjusted life years of up to o 69.4 million (Shield, Parry, & Rehm, 2013). As a result, it has been ranked as one of the leading risk factors for death and disability worldwide. The toxicity of alcohol components including ethanol largely contribute to increased chances of developing liver disease. The liver controls most of the body support systems, therefore, a disease of the liver is fatal as it will lead to malfunction of all the major body systems
Causes of confusion and other symptoms.
Various factors contribute to the occurrence of liver disease. Of these, duration and amount of alcohol consumed are most significant. Host factors such as IPNPLA3 gene polymorphisms and obesity and environmental factors also contribute to an increased risk of developing liver disease (Singal, Chaha, Rasheed, & Anand, 2013). Disease of the liver leads to reduced functionality of the liver which consequently cause accumulation of toxic substances in the bloodstream. These instances lead to alterations in the level of consciousness of an individual, confusion, and other cases coma. In Mr. McGrath’s case, hepatic encephalopathy may be the cause of disorientation.
Abdominal swelling by the patient indicates extensive complications. Life-threatening complications associated with portal hypertension including ascites may be present in the patient. Increased pressure on the portal vein leads to ascites characterized by fluid build-up in the abdominal cavity. Yellowish skin, delirium, and confusion are also observed in this condition (A.D.A.M, 2013). Varices are likely to develop in instances of portal hypertension, as a means of providing alternative pathways for diverted blood.
Oesophageal varices pathophysiology and management strategies.
Almost half of the patients suffering from cirrhosis during diagnosis have been found to have gastroesophageal varices (Pericleous et al., 2016). The varices arise due to portal hypertension resulting from an increase in portal blood flow resistance in cirrhosis and also due to the rise in blood inflow into the portal vein. An increase in resistance is said to be structural, due to a destruction of the vascular architecture of the liver by regenerative nodules and fibrosis as a result of an increase in the tone of the hepatic vasculature primarily due to the dysfunction of the endothelium and a decrease in the bioavailability of nitric oxide.
Three principal events cause portal hypertension. First, it can be due to a physical obstruction arising from a fibrosis or at other instances from regenerative nodules resulting in an increase in the resistance to blood flow. An imbalance between vasoconstrictors and vasodilators in the liver also develops. Such imbalance results in a reduction of the activity of eNOS in the liver. The event is, however, rectifiable using medications such as nitrates and beta-blockers. A combination of these events leads to the occurrence of porto-systemic collateral circulation of aiming to decompress the portal circulation (Frazier, Stocker, Kershner, Marasano, & McClain, 2014). Splanchnic vasodilation occurs due to a relative extra-hepatic and ischaemic liver increase in Nitrite Oxide, with the signalling of the sGC-PKG and smooth muscle cell relaxation. This leads to increased blood flow volume into the portal which maintains hypertension. This results in a hyper-dynamic circulation that is linked to these hemodynamic variations in portal hypertension and cirrhosis. This is manifested as high cardiac output with little arterial hypotension and systematic vascular resistance (Pericleous, et al., 2016).
Hepatic pressure can be applied to obtain hepatic venous pressure gradient (HVPG) that ranges normally from 1 to 5mmHg. This procedure is performed by inserting a catheter into a hepatic vein to get the hepatic vein pressure. HVPG is equal to WHVP minus free (HVP) where HVPG is used to represent the gradient between caval pressure and the portal (Molina et al., 2016). FHVP acts as an internal zero by cancelling out variations in abdominal pressure. Sinusoidal hypertension differs from pre-sinusoidal portal hypertension which associated with an increase in HVPG as flow resistance builds up in the portal vein. Varices therefore develop in the event that HVPG is greater than ten mmHg.
Antibiotics have been introduced in variceal hemorrhage management, a factor which has significantly improved clinical outcomes. Bacterial infections, both primary and secondary, are common in cirrhotic patients as bacteria actively translocate from the impaired mucosal surface into the portal system and the patient’s impaired immune function (Molina, Gardner, Souza-Smith, & Whitaker, 2014). In these patients, antibiotics decrease the bacterial load, reducing infections, recurrent bleeding, and reduce morbidity and mortality in patients with gastroesophageal varices. Broad spectrum antibiotics prophylaxis is thus recommended in individuals with suspected and confirmed variceal hemorrhage (Shah, 2016).
Nonselective beta blockers can be used in patients having a low-risk small varices, as they can delay variceal growth preventing variceal bleeding (Runyon, 2015, September 23). The treatment is applied in absence of severe liver disease, and where the varices are without red wale marks. In persons with varices containing red wale marks and others associated with a high risk of haemorrhage, non-selective beta-blockers are used.
For patients that have medium and large varices, endoscopic variceal ligation or beta-blockers can be used. Non-selective beta-blockers are advantageous as they are cheap and use requires no expertise. These medications also prevent against other medical conditions like spontaneous bacterial peritonitis and bleeding from ascites and portal hypersensitive gastropathy (Garcia-Tsao & Bosch, 2011).
The role of abdominal paracentesis and possible complications.
The presence of excess fluid in a patient’s abdominal cavity cause significant discomfort to the patient and shortness of breath. Abdominal paracentesis is a simple procedure that involves insertion of a needle into the peritoneal cavity of the patient to remove the ascetic acid. Removal of a small amount of the fluid for testing is referred to as diagnostic paracentesis, while therapeutic paracentesis is considered the removal of up to five litres of the excess fluid so as to decrease the resultant intra-abdominal pressure helping in relieving related abdominal pain, dyspnea and early satiety (Runyon, 2015).
Paracentesis should be performed by a properly trained physician. Performing this procedure at the time the patient is admitted to a hospital, to patients suspected or suffering from cirrhosis and ascites decrease the mortality rates in a health care setting. In instances where paracentesis was conducted on admission, a lower in-hospital mortality rate was recorded compared to those who did not perform the procedure (Cavazzo, Bugiantella, Graziosi, Franceschini, & Donini, 2013).
Paracentesis also helps clarify the primary cause of ascites when testing for infection. Unexpected diagnoses including chylous, eosinophilic or hemorrhagic ascites can also be indicated by this procedure (Pericleous et al., 2016). Analysis of the fluid shed light on the cause of the ascites and if present, the bacterial infection. Upon culturing antibiotic susceptibility of the bacteria can be identified therefore easier treatment.
Despite the benefits of paracentesis, various complications occur. The ascitic fluid leak is the most common complication associated with the procedure. Failure to peform a Z-track properly can lead to a leakage of the ascetic fluid leak. In this case, a large-bore needle may be used, or when the skin incision created is overly large. If the leak on the surface is prolonged, cellulitis may develop (Wedro, 2015).
Bleeding from a blood vessel may arise if a vein or artery is torn by the needle. Bleeding can be extremely severe and potentially fatal especially if an artery is affected. A further disastrous situation may arise in the presence of renal failure. In patients with primary fibrinolysis, three-dimensional hematomas may develop requiring anti-fibrinolytic treatment (Molina et al., 2014). Bowel infection may occur in instances where the bowel has been injured by the paracentesis needle. Fortunately, this does not usually result to clinical peritoritis, and thus treatment is not necessitated, not unless patients indicate signs of infections. Death may also occur due to paracentesis.
Mr. McGrath educational requirements.
Mr. McGrath should be advice on the importance of total abstinence from alcohol to prevent further complications. He should also be educated to take a diet low on ammonia to reduce the amount of toxic products that will be produced by the body. High cholesterol containing foods should also be avoided to reduce the arterial pressure and therefore amount of fluid in the stomach. The prescribed medicine should be strictly adhered to prevent further complications. Garcia-Tsao & Bosch, (2011) enlighten that support groups and peer help especially from other patients and medical practitioners can be employed to provide additional moral support to patients. Sharing of past experiences by the patients will boost the recovery of Mr. McGrath. Mr.Grath should be advised on the importance of abstinence from cigarettes as they significantly increase the level of toxic compounds in his blood system.
Analysis of Mr. McGrath current prescription.
Propranolol or otherwise known as Inderal is prescribed to the patient for pharmacologic crophylaxis of variceal bleeding. Varices may probably have been identified in the patient. Propranolol reduces the portal pressure through reduction in the cardiac output, and reducing portal blood inflow via splanchnic vasoconstriction (Runyon, 2015, September 23). Spironolactone is an aldosterone antagonist which act on the distal tubules to conserve potassium and increase natriuresis. The drug is mainly used as a diuretic. Furosemide is prescribed to Mr. McGrath to treat the fluid build-up in the body. The drug is an anthranilic acid derivative and a diuretic. It inhibits absorption of sodium and chloride in the proximal, the loop of Henle and distal tubes.
Conclusion
Alcohol liver disease is one of the primary causes of liver-related mortality in the United States. Clinicians, therefore, should be well versed in diagnosis and treatment procedure for the condition. Education to the population may play a significant role in reducing severe forms of the conditions by advocating for early testing and treatment. In Mr McGrath case, follow-up after treatment should be conducted to facilitate a full recovery. In cases of total failure of the liver a transplant should be considered in order to maintain the acceptable toxicity levels of blood ammonia.
Cavazzo, E., Bugiantella, W., Graziosi, L. A., Franceschini, M. S., & Donini, A. (2013, February). Malignant ascites: pathophysiology and treatment. International Journal of Clinical Oncology, 18(1), 1-9. doi:10.1007/s10147-012-0396-6
Frazier, T. H., Stocker, A. M., Kershner, N. A., Marasano, L. S., & McClain, C. J. (2014, May 1). Critical pathophysiological process and contribution to disease burden. Physiology, 203-215. Retrieved September 04, 2016
Garcia-Tsao, G., & Bosch, J. (2011, March 4). Management of varices and variceal hemorrhage in cirrhosis. The New England Journal of Medicine, 362, 823-832. doi:10.1056/NEJMra0901512
Molina, P. E., Gardner, J. D., Souza-Smith, F. M., & Whitaker, A. M. (2014). Alcohol abuse: Critical pathophysiological processes and contribution to disease burden. Physiology, 29, 203-215. doi:10.1152/physiol.00055.2013
Pericleous, Marinos, Sarowski, Alexander, Moore, Alice, . . . Murtaza. (2016, March). The clinical management of abdominal ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome: a review of current guidelines and recommendations. European Journal of Gastroenterology & Hepatology, 28(3), e10-e19. Retrieved September 04, 2016, from http://www.ingentaconnect.com/content/wk/ejghe/2016/00000028/00000003/art00001?crawler=true
Shield, K. D., Parry, C., & Rehm, J. (2013). Focus on: Chronic diseases and conditions related to alcohol use. The Journal of National Institute on Alcohol Abuse and Alcoholism, 35(2). Retrieved September 4, 2016, from http://pubs.niaaa.nih.gov/publications/arcr352/155-173.htm
Singal, A. K., Chaha, K. S., Rasheed, K., & Anand, B. S. (2013, September 28). Liver transplantation in alcoholic liver diseases current status and controversies. World Journal of Gastroenterology, 19(36), 5953-5963. doi:10.3748/wjg.v19.i36.5953
Torruellas, C., French, S. W., & Medici, V. (2014, September 7). Diagnosis of alcoholic liver disease. World Journal of Gastroenterology, 20(33), 11684-11699. doi:10.3748/wjg.v20.i33.11684
Child Maltreatment and Rating Its Severity in the US 4 pages in length with a title page, abstract and reference page (total of 7 pages).
Child Maltreatment and Rating Its Severity in the US
12 point font using Times New Roman. 1" margins all around double spaced. 5 sources to include: Juvenile Justice 6th edition by Karen M. Hess, Christine Hess Orthmann and John Paul Wright 2017. Other sources may be from journal articles, books or the internet. NO Wikipedia. Sources must be cited throughout paper. Children and their primary caregivers participating in a consortium of ongoing longitudinal studies were interviewed when they were approximately 4 and 8 years of age to assess behavior problems and developmental and psychological functioning.
Insulin Glargin in type 2 Diabetes Case Study -For the three articles, please evaluate each article individually by answering based on these questions:
1. What’re the endpoints of the study?
Insulin Glargin in type 2 Diabetes Case Study
Do the endpoints of the trial truly represent what is claimed as being studies or clinically significant? Why or why
not?
2. What’re the statistical analyses? We discuss the appropriateness of each statistical test used in the study. Are the statistic tests used to evaluate the
data appropriately? What’s the type of data is assessing (nominal, ordinal, or continuous)if any? Is the effects size clinically relevant?
3. What’s are baseline characteristics? Is it appropriated? If not, would this affect the results?
4. What’s the efficacy of the study and the results?
5. What’s safety/adverse events.
6. What’s the limitation of the study if any.
Lastly, after critique these three articles, please come up a few “LEARNING OBJECTIVES” as you are going to presenting this topic to the audiences, what you
want the audiences to know and/or to learn from? (Be concise with each objective.
-In addition, from the 3 articles, please provide recommendations to the audiences. Would you recommend exenatide over insulin as second therapy in treating
type 2 diabetes? Why or why not? (Like is it apply for all population or just certain populations with high-risk factors might benefit from it? Be more
specific)
-Also, who is funding these study? Comment whether this can be bias or not bias in testing since they want the drugs to be market. If you think not, why not?
How does the Energy Drinks Effects Our Body and Health
.helps determine wether subject has been researched before
.helps decide if research is necessary
.helps decide if research is worth doing
topic:
.reflect on topic and ask questions:
.is it practical to undertake research?
.will it be useful to do the research?
Action:
.draft a simple, clear title following these words: ‘my study is about…’
.or write what question needs to be answered
.consider whether the subject can or should be researched
.check existing research would ass something, or just replicate what already exists
.consider the amount of time and resources that the research will require.
The use of a literature review:
.To summarise the important literature available on the subject
.to frame the problem to be addressed
.to provide direction for future research
.to uncover a proposed theory of or explanations of the problem
.for use as a comparison
Discuss the different types of vegetarian diets; Vegetarianism, Semi-vegetarian, Lacto-ovo vegetarian, Lacto vegetarian, and Pescetarian. What are the
benefits of consuming a vegetarian diet? What are some of the nutrients that are at risk of deficiency in vegetarian diets? How can individuals meet their
protein needs with a vegetarian or vegan diet? Please answer with at least 350 words for this
We can write this or a similar paper for you! Simply fill the order form!
Why Clinton Health Reform Plan in 1990s Never Passed Order Instructions: Consider why the Clinton Health Reform Plan in the 1990s never passed.
Include the following:
1. How does Obama’s Affordable Care Act of 2010 compare with the Clinton Health Reform Plan?
2. Discuss the pros and cons of the Affordable Care Act.
3. Discuss three changes would you recommend to improve on the legislation?
Why Clinton Health Reform Plan in 1990s Never Passed
Your paper should have a word count of 800-1,200 words and a minimum of three scholarly sources must be cited.
Prepare this assignment according to the guidelines found in the GCU Style Guide located in the Student Success Center.
This assignment uses a grading rubric. Please review the rubric prior to beginning the assignment to become familiar with the expectations for successful completion.
No Plagiarism!!
Why Clinton Health Reform Plan in 1990s Never Passed Sample Answer
There are two comparable health reforms which result from the proposals developed by Obama and Clinton. Hillary reforms were initiated in the early 1990s when President Clinton proposed that Hillary lead the efforts that could lead to the enactment of major legislation regarding the health reforms. However, despite the initiation of these efforts they failed infamously. The sketchy reforms plans contributed to the failure of the Clintons’ reform. The Obama care, on the other hand, saw the need to reform the federal health law and came up with the enactment of patient protection and affordable care to its citizens (Rudnicki et al, 2016). According to Obama, the health reforms developing process would involve complete transparency and open negotiations which are different to Clinton’s proposals as these factors were major issues of procedural criticism of his reforms. The Obama care act was consistently lobbied by the president as compared to Clinton’s reforms. There emerged a difference where a health insurer identified as a scape goat was present during the enactment of the Obama care as compared to Clinton’s act. The Democratic congressional leaders and major interest groups benefited the Obama care act leading to its massive success as compared to Clinton’s reforms which failed.
The Obama care act focused on reconfiguring regulations relating to health insurance reforms with the objective of fixing the problems in health care (Rudnicki et al, 2016). On the other hand, Clinton’s care was far more reaching focusing on changing the management, financing and regulation of care and also called for more involvement of the government in these reforms. During the development of the Obama care act, the lawmakers were continually pushed to keep at it against the long odds. On the other hand, Clinton reforms did not emphasize on the same where the transparency was compromised making which was a factor contributing to failure since the reforms were seen to be sketched out inappropriately. Obama care act capitalized on the mistakes made during forming Clinton’s reforms to ensure the regulation and affordable care act succeeded effectively (Stapletown et al, 2015).
The Affordable care act had its advantages and disadvantaged since the development of its reforms. The affordable care act has made it possible for more citizens to have health insurance obtaining coverage and insured. The act has enhanced the affordability of insurance by eliminating unreasonable rate increases and enhancing lower premiums. A wider coverage of options is provided to the American citizens. No time limits on care have been made possible where the coverage issues have been minimized. Through the Obama care act, there is lower prescription to drug costs making medication easily affordable for all people. More screening is covered courtesy of Obama care act. There are also cons associated with the Affordable Act which includes payment of higher premiums in the name of wider coverage and a range of benefits (Stapletown et al, 2015). The possibility of been fined due to failure to possess an insurance cover as the government argues that it is mandatory for one to have insurance to cover their healthcare cost. The Affordable Act has resulted in increasing the tax rates, e.g., on the pharmaceutical sales and medical devices. The affordable care acts have made enrollment be complicated due to delays and lower number of signups resulting from website problems (Kriner et al, 2014). Addressing the cons effectively would ensure the problems are converted into pros and benefits of the act. The first change I would make on the legislation is ensuring sufficient funds are provided to finance the insurance adequately amending the high costs and affordability problems. The budgeting and financing would influence the implementation of the reforms to the letter. Changes in the healthcare field such as having more qualified administrators and improving the technology used in the implementation of the act are essential. The changes would address problems such as complications during enrollment and other inefficiencies. Enacting reforms that control the high premiums and also restricting unnecessary fines on the uninsured rather than having measures to have them covered is a crucial change in the legislation (Kriner et al, 2014).In a nutshell, the adherence and implementation of the right reforms would enhance full coverage of all people.
Why Clinton Health Reform Plan in 1990s Never Passed References
Kriner, D. L., & Reeves, A. (2014). Responsive Partisanship: Public Support for the Clinton and Obama Health Care Plans. Journal Of Health Politics, Policy & Law, 39(4), 717-749. doi:10.1215/03616878-2743015
Rudnicki, M., Armstrong, J., Clark, C., Marcus, S., Sacks, L., Moser, A., & … Public Policy and Advocacy Committee of the, S. (2016). Expected and Unexpected Consequences of the Affordable Care Act: The Impact on Patients and Surgeons-Pro and Con Arguments. Journal Of Gastrointestinal Surgery, 20(2), 351-360. doi:10.1007/s11605-015-3032-8
Stapletonw, P., & Skinner, D. (2015). The Affordable Care Act and assisted reproductive technology use. Politics & The Life Sciences, 34(2), 71-90. doi:10.1017/pls.2015.13
Ebola Virus Disease Patients Should not Receive CPR Order Instructions: Using the assigned readings and information from the literature, compose a response to the following statement:
Ebola Virus Disease Patients Should not Receive CPR
Question: Patients with Ebola virus disease (EVD) should not receive CPR. For this paper, you will weigh in on the RN’s ethical obligation when providing care to patients with EVD and the performance of CPR.
Please cite two references from the textbook & article below. APA style
Required Textbooks and assigned reading for this paper:
Brunner and Suddarth’s textbook of medical-surgical nursing**
• Chapter 3: Critical Thinking, Ethical Decision Making, and the Nursing Process
• Chapter 23: Management of Patients With Chest and Lower Respiratory Tract Disorders (section on “Pulmonary Tuberculosis”)
• Chapter 35: Assessment of Immune Function (section on “Function of the Immune System”)
• Chapter 37: Management of Patients With HIV Infection and AIDS
• Chapter 42: Management of Patients with Musculoskeletal Disorders (section on Musculoskeletal Infections”).
• Chapter 49: Assessment and Management of Patients With Hepatic Disorders (sections on “Viral Hepatitis, “Hepatitis A, B, and C”, and “Nonviral Hepatitis”)
• Chapter 55: Management of Patients With Urinary Disorders (sections on “Infections of the Urinary Tract”)
• Chapter 69: Management of Patients With Neurologic Infections, Autoimmune Disorders, and Neuropathies (section on “Infectious Neurologic Disorders”)
• Chapter 71: Management of Patients with Infectious Diseases
Pharmacology: A patient-centered nursing process approach**
• Chapter 14: Medications and Calculations
• Chapter 29: Penicillins and Cephalosporins
• Chapter 31: Sulfonamides
• Chapter 32: Antituberculars, Antifungals, Peptides, and Metronidazole
• Chapter 34: Drugs for Urinary Tract Disorders
• Chapter 36: Vaccines
Maternal & Child Health Nursing**
• Chapter 40: Nursing is of a Family When a Child has a Respiratory Disorder (section on Disorders of the lower respiratory tract: influenza and tuberculosis)
• Chapter 42: Nursing Care of a Family When a Child has an Immune Disorder
• Chapter 43: Nursing Care of a Family When a Child has an Infectious Disorder (section on “Infection”)
•Chapter 45: Nursing Care of a Family When a Child has a Gastrointestinal Disorder (section on “Hepatitis”)
• Chapter 49: Nursing Care of a Family When a Child has a Neurologic Disorder (section on “Bacterial Meningitis”)
• Chapter 51: Nursing Care of a Family When a Child has a Musculoskeletal Disorder (section on “Infectious and Inflammatory Disorders of the Bones and Joints”)
Nursing Diagnosis
• Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Web-based and Other Professional Resources:
• Hand Hygiene in Healthcare Settings
• Hospital: 2016 National Patient Safety Goals**
• Pre-licensure KSAs (2014)**
• Ebola virus disease: an emerging threat (2014)**
• Zika virus (2016)**
M1D1: The Ethical Obligations of the RN Providing care to the Patient with Ebola Virus Disease
The article:
Ethical Issues in the Response to Ebola Virus Disease in US Emergency Departments: A Position Paper of the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine
Arvind Venkat, MD, FACEP,
Lisa Wolf, Ph.D., RN, CEN, FAEN,
Joel M. Geiderman, MD, FACEP,
Shellie L. Asher, MD, FACEP,
Catherine A. Marco, MD, FACEP,
Jolion McGreevy, MD, MBE, MPH,
Arthur R. Derse, MD, JD, FACEP,
Edward J. Otten, MD, FACMT, FAWM,
John E. Jesus, MD, FACEP,
Natalie P. Kreitzer, MD,
Monica Escalante, MSN, BA, RN,
Adam C. Levine, MD, MPH, FACEP,
on behalf of the
American College of Emergency Physicians,
the
Emergency Nurses Association,
and the
Society for Academic Emergency Medicine
Show more
http://dx.doi.org.vlib.excelsior.edu/10.1016/j.jen.2015.01.012Get rights and content
Referred to byAnne Manton
Editor’s Note regarding the on-line position paper, “Ethical Issues in the Response to Ebola Virus Disease in US Emergency Departments: A Position Paper of the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine”
Journal of Emergency Nursing, Volume 41, Issue 2, March 2015, Page 99
PDF (58 K)
M1D1: The Ethical Obligations of the RN Providing care to the Patient with Ebola Virus Disease
The 2014 outbreak of Ebola Virus Disease (EVD) in West Africa has presented a significant public health crisis to the international health community and challenged US emergency departments to prepare for patients with a disease of exceeding rarity in developed nations. With the presentation of patients with Ebola to US acute care facilities, ethical questions have been raised in both the press and medical literature as to how US emergency departments, emergency physicians, emergency nurses and other stakeholders in the healthcare system should approach the current epidemic and its potential for spread in the domestic environment. To address these concerns, the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine developed this joint position paper to provide guidance to US emergency physicians, emergency nurses and other stakeholders in the healthcare system on how to approach the ethical dilemmas posed by the outbreak of EVD. This paper will address areas of immediate and potential ethical concern to US emergency departments in how they approach preparation for and management of potential patients with EVD.
Keywords
Ethics;
Ebola virus disease;
Emergency department
Introduction
In March 2014, an outbreak of Ebola Virus Disease (EVD) was confirmed in the West African nation of Guinea with subsequent rapid spread to the neighboring countries of Liberia and Sierra Leone. Given the underdeveloped health infrastructures in the 3 primary affected nations and the high transmission and mortality rate of the disease, domestic and international public health agencies called for aid and personnel to be rapidly deployed to the affected nations to treat infected patients and prevent further spread of the Ebola outbreak. Yet despite significant efforts from the international community, EVD continues to represent a significant challenge in the region. As of January 2015, the Centers for Disease Control and Prevention (CDC) reports that the total case count stands at 21,689 with 8,626 deaths and continues to rise.1
In the United States, the transfer of Ebola-infected healthcare workers from the outbreak zone to US hospitals raised public awareness and fear of the spread of the disease. This fear was heightened after the initial missed diagnosis in a US emergency department of a patient with EVD who later died,2 the transmission of Ebola to 2 nurses who cared for this patient3 and a subsequent case of an emergency physician who traveled to West Africa to care for patients with EVD and required hospitalization after returning to the United States.4 These cases raised significant concerns that US emergency departments and hospitals were not adequately prepared to diagnose and treat patients with EVD. In addition, the infection of healthcare personnel created the specter of a more widespread outbreak in the general population due to poor infection control guidelines, inadequate training, and management protocols in US medical centers and initially absent mechanisms to identify potentially infected individuals arriving through US ports of entry.5 A subsequent controversy surrounding a nurse who returned from West Africa without symptoms of EVD and was held in quarantine highlighted concerns about how personal liberty and public health should be appropriately balanced.6 In response, both emergency medicine and emergency nursing organizations and federal agencies have issued guidance on the nature of EVD, approaches to identification, isolation, and treatment of potential patients and standards for use of personal protective equipment (PPE) by healthcare providers.7, 8 and 9
While the number of cases in the United States remains low to date (10 total patients, 4 diagnosed in the US and 2 deaths), the outbreak of EVD has raised ethical issues relevant to US emergency departments and hospitals, emergency physicians and emergency nurses. Issues articulated in the medical literature and by the press include the following: how resources should be used in preparation for the likely rare event of an undiagnosed patient with EVD who presents to a US emergency department,10 whether there should be a different standard for care of Ebola-infected patients than for other patients with less contagious and lethal diseases11 and whether healthcare providers are obligated to place themselves at a significant degree of risk while caring for these patients due to their professional status.12 To address these concerns, the American College of Emergency Physicians (ACEP), the Emergency Nurses Association (ENA), and the Society for Academic Emergency Medicine (SAEM) developed this joint position paper to provide guidance to US emergency physicians, emergency nurses and other stakeholders in the healthcare system on how to approach the ethical issues posed by the outbreak of EVD. This paper will address areas of immediate and potential ethical concern to US emergency departments in how they approach preparation for and management of potential patients with EVD.
Ebola Virus Disease Patients Should not Receive CPR and Characteristics of EVD of Ethical Relevance
Since the outbreak of EVD, numerous articles have been published on the epidemiologic characteristics of this condition and the microbiological details of the causative organism.13, 14, 15 and 16 However, particular characteristics of EVD are worth highlighting to provide the factual basis for addressing the ethical questions raised in this outbreak for US emergency departments. First, it is well recognized that individuals with EVD will often have relatively non-specific symptoms, common to many viral infections, in their initial stages of presentation (eg, fever, headache, myalgias).15 and 17 Such non-specific presentations make unrecognized infection with Ebola a realistic concern. Lack of prompt identification of potential patients by emergency department staff can increase the risk of spread of the disease and mandates a heightened awareness of the risk factors for the disease. Second, the pathophysiology of contagion is related to contact with blood or bodily fluids from an infected individual, with rising viremia in the late stages of disease presenting a particular risk for human-to-human transmission. However, even a low level of viral inoculation can lead to EVD.18 This recognized pathway of spread aids in evaluating the risk of transmission from patient to healthcare providers or the general public. At the same time, knowledge of how the Ebola virus is transmitted heightens the ethical concerns posed by the potential presence of highly symptomatic and contagious patient(s) to an emergency department, especially if to a center without specialized experience in the care of EVD patients. Finally, the lack of specific effective treatment and the high mortality rate posed by EVD exacerbates public fears, may create irrational panic relative to the actual risk and lead to unexpected institutional consequences such as the avoidance of the use of healthcare facilities where EVD patients are being or have been treated.
Characteristics of Emergency Department Practice of Ethical Relevance
The emergency department in the United States and increasingly worldwide serves as the primary gateway to the acute healthcare system. It is estimated that 50% of admissions to hospitals in the US are initially assessed and treated in emergency departments.20 The emergency department is also the only access point in the US acute healthcare system available to patients 24 hours per day-7 days per week. In the US there is a legal obligation under EMTALA to provide a medical screening exam for an emergency medical condition and treatment until the emergency medical condition is resolved or stabilized to the extent of that hospital’s capability (until appropriate transfer) regardless of insurance status or other socioeconomic factors.21 and 22 Finally, the emergency department is the primary location for the initial evaluation, diagnosis, and treatment of the acutely ill undifferentiated patient. These facts together help define the ethical construct of emergency medical practice where access to quality emergency care is a right of all patients in the US. As noted in the ACEP Code of Ethics, “Emergency physicians shall respond promptly and expertly, without prejudice or partiality, to the need for emergency medical care.”23 The ANA Code of Ethics states that “The emergency nurse works to improve public health and secure access to health care for all.”24 The Society for Academic Emergency Medicine, through its mission statement “to lead the advancement of emergency care through education and research, advocacy, and professional development in academic emergency medicine,”25 also supports the ethical mandate for all patients in the United States to have access to quality emergency medical care regardless of disease process, ability to pay or other characteristics.
While the above ethical framework emphasizes the critical importance of the availability of emergency care to all, it is clear from both published codes of ethics and the literature on the “duty to treat” that there are rare circumstances in which risk to the individual healthcare provider and institution should be weighed in determining the treatment plan for a patient who poses a significant risk to providers or the general public. The ACEP Code of Ethics notes the requirement of the adequacy of in-hospital and outpatient resources in the provision of emergency care.23 The American Medical Association Code of Ethics states that “Because of their commitment to care for the sick and injured, individual physicians have an obligation to provide urgent medical care during disasters. This ethical obligation holds even in the face of greater than usual risks to their own safety, health or life. The physician workforce, however, is not an unlimited resource; therefore, when participating in disaster responses, physicians should balance immediate benefits to individual patients with ability to care for patients in the future.”26 The American Nurses Association Code of Ethics specifically states, “The nurse owes the same duties to self as to others, including the responsibility to preserve integrity and safety.”27 Within the larger ethics literature, explorations of whether there is a duty to treat on the part of healthcare providers at risk to themselves also indicate that codes of ethics, historical references, and theoretical analysis do not mandate an absolute obligation. Rather, particular factors of disease process, availability of resources and training, countervailing responsibilities outside of the professional realm, personal viewpoints on the virtues of courage and resilience as well as relational ethics perspectives and obligations imposed by professional status have guided the evaluations of the obligations of healthcare providers in the face of outbreaks of infectious disease.28, 29, 30 and 31 For emergency departments, emergency physicians and emergency nurses, there is a need to weigh all of these considerations against the special role played by emergency departments in the US healthcare system and the duties that accompany the professional status of emergency physicians and emergency nurses.
Current and Potential Future Ethical Considerations with the Outbreak of EVD
With this background, we will present an ethical framework that has potential application for emergency departments, emergency physicians and emergency nurses along with other health system stakeholders in the particular response to EVD in the United States. This framework will address questions relevant to US emergency departments and separate consideration of the current situation (few confirmed cases within the United States with a relative abundance of resources to respond) versus 2 potential scenarios (increasing number of potential and confirmed domestic cases of EVD in a variety of locations due to spread in the US and widespread number of potential and confirmed domestic cases that would strain existing resources and creates a necessity of disaster triage response) where appropriate.
What are the Ethical Obligations of US Emergency Departments and Hospitals to Support or Encourage the Volunteering of Emergency Physicians and Emergency Nurses to Serve as Healthcare Providers in those Countries Most Affected by the Current Outbreak of EVD?
In the current outbreak of EVD, as of January 1, 2015, there are no extant active cases in the United States. As such, the most immediate issue is how to contain the spread of the disease from its present locus in West Africa and end the current epidemic there. With the underdeveloped nature of the health infrastructure in the primarily affected nations and the declaration of a Public Health Emergency of International Concern by the World Health Organization,32 there is widespread recognition that ending the epidemic does and will continue to require the volunteering of healthcare providers to serve in the outbreak zone.
Under the ethical principle of reciprocity, which calls for acting in a manner that one would want others to act in return, there is an obligation to support emergency physicians and nurses who volunteer to serve in the nations primarily affected by the current Ebola epidemic, just as we would welcome support or available expertise in a time of health crisis in the US. Yet as a practical matter, support of volunteerism needs to be weighed against the special logistical concerns faced by most emergency departments, where local staffing levels must be maintained to provide safe patient care. An application of the principle of reciprocity in this outbreak would include support of emergency physician and nurse volunteerism in the current outbreak through the covering of shifts and other professional obligations in the volunteer’s absence and acceptance by volunteering emergency physicians nurses of any potential risk of contagion on return to the US and the resultant need for monitoring for signs of the disease and possibly prolonged isolation.
We would propose that in considering the support of volunteerism by emergency physicians and nurses, the specific background, training, and education of the provider is a key decision making a factor. Education and training are essential components of preparation prior to disaster or disease outbreak response. Medical volunteers should be appropriately trained in disease management, including rendering effective supportive care within the resource constraints in the primary outbreak zone, prior to travel to infected areas. They should ensure to the extent possible that malpractice, health, and life insurance are in place to cover potential events, likely with the assistance of the Non-Governmental Organization or other agency sponsoring their volunteer efforts. They should be willing to undertake the risks of volunteerism, including infection or threats to individual safety and security.33, 34 and 35 Volunteers should be prepared to ensure appropriate infection control practices in their international work and to follow recommended protocols upon return for monitoring for symptoms of EVD and the isolation that might result.36, 37 and 38 Without this preparation, volunteering emergency physicians and nurses may be a liability rather than a benefit to the resource-poor countries primarily affected by the Ebola outbreak and a risk to the domestic population upon their return to the US.
It is appropriate for emergency departments and hospitals to query volunteering staff on their willingness to undergo the necessary training to be effective in the primary outbreak zone. With the continuing spread of the disease in West Africa, those volunteering emergency physicians and nurses with existing experience in Ebola and disaster response should be given priority over those without such training. Specific decisions regarding support for volunteer efforts should also include the number of volunteers and impact on ED staffing and potential impact on public health domestically (i.e., will the loss of experienced providers adversely affect the care of patients in the local area served by the emergency department?). If the current outbreak were to spread significantly within the US, the ethical evaluation of the appropriateness of supporting volunteerism overseas would likely change since this could result in the expertise on the management of EVD being shifted out of the country rather than being available domestically. This emphasizes the importance of supporting present efforts of containing and ending the current epidemic in West Africa, including with the volunteerism of trained emergency physicians and nurses, as the most effective means of preventing the spread of EVD to the US and other countries.
Some emergency departments have supported the volunteerism of emergency physicians in particular through altruistic coverage of shifts to allow staff to travel to the primary outbreak zone.39 In addition, private foundations have provided grant funding to alleviate the financial burden of volunteerism of emergency department staff in the outbreak zone.40 While these novel approaches have been largely confined to academic settings, they do suggest that there may be methods for individual centers to address the logistical difficulties that can arise when US emergency department providers volunteer in the primary outbreak zone. The application of these options to individual centers is one that is best judged on a case-by-case basis based on the factors noted above.
Finally, emergency departments, emergency medicine, and nursing professional societies, Non-Governmental Organizations and government agencies can aid volunteer efforts by educating health care providers and the lay public using published evidence on the pathophysiology of Ebola and its transmission to alleviate the stigma that returning volunteer staff may experience after their efforts. At the same time, as noted above, volunteering emergency physicians and nurses have an obligation to adhere to monitoring and isolation protocols upon return to the US as a reciprocal ethical obligation for the support their efforts have received.
What are the Ethical Obligations of Emergency Departments and Hospitals to Support other Centers in the Domestic Response to EVD?
As of December 2014, 44 medical centers have been designated by the Centers for Disease Control and Prevention as having the necessary capability and equipment to care for patients diagnosed with EVD.41 It is anticipated that patients with a confirmed EVD diagnosis will be transferred to these hospitals which will have enough PPE and other treatment requirements (isolation rooms, dedicated equipment and designated physicians, nurses and other necessary health care professionals and staff with proper training under CDC guidelines) to manage patients for at least 7 days, after which governmental agencies would assist in acquiring more supplies and expertise if needed.42 However, not every state or locality has such a facility, nor is it likely that an undiagnosed patient would necessarily present to one of these centers. Therefore, the CDC has provided guidelines for so-called frontline (any emergency department or acute care facility) and Ebola assessment hospitals, which can safely isolate, treat and transfer patients with suspected or confirmed EVD. To meet these standards, the CDC has called for all emergency departments to have protocols in place for the recognition of potential Ebola patients and training for the proper isolation and assessment of these individuals.42
The hierarchy of treatment facilities for EVD codifies the reciprocity-based obligations that hospitals have to each other in the current state of the outbreak. Such reciprocity should extend to the sharing of PPE, trained staff and other necessary equipment as needed to care for a suspected or confirmed Ebola patient until the transfer can be effected to a designated treatment center. Hospitals and emergency departments should consider and develop relevant protocols for rapid credentialing of staff and transfer of equipment to allow resources to be brought to bear should there be additional cases in the US. If the current epidemic were to spread significantly in the US, hospitals should consider whether and how they can upgrade their capabilities to meet the needs of rising numbers of patients, presumably with the assistance of government resources.
Another ethical consideration is the reputational impact upon hospitals caring for Ebola patients. As has been reported in the press, hospitals have expressed concern that the potential costs and risks accrued in treating an Ebola patient along with the public fear generated by the disease may have an adverse impact on volumes and financial results for medical centers. The facility in Dallas that treated a recent case reported that afterward emergency department volumes dropped and still have not returned to their expected level.19 It is therefore imperative, in the face of a disease such as Ebola that has generated such public scrutiny and at times hysteria, for hospitals to be cognizant of their ethical responsibility to support the efforts of designated treatment centers as well as frontline facilities that might encounter Ebola patients and potentially be perceived adversely by the public. We affirm that the principle of reciprocity extends beyond physical means of support (equipment, personnel) to reputational support in the setting of an outbreak of EVD. Such support could, where appropriate, take the form of publicly confirming the safety and quality of other healthcare facilities with Ebola patients, educating other facilities on effective policies and procedures in caring for EVD patients and avoiding messages that implicitly suggest a competitive advantage from not treating patients with this highly infectious disease. Through such support, hospitals ensure that the public is aware and reassured of the unified response the medical system will take towards both the existing epidemic and the potential for worsening if the outbreak spreads from West Africa. Without such reputational support and cohesion in the healthcare system, should the epidemic worsen, it is conceivable that public doubt and panic may lead to untenable consequences such as facilities avoiding the care of at-risk patients and the public fearing certain hospitals as being sites of contagion rather than medical care?
Should Trainees be Allowed to Participate in the Care of Suspected or Confirmed EVD Patients?
Trainees (nursing students, medical students, residents, and fellows) routinely care for patients with infectious diseases in the ED and should understand and use proper measures to protect themselves while caring for patients with potential or confirmed contagious diseases. Both the Accreditation for Graduate Medical Education program requirements in emergency medicine and guidance on Ebola affirm that trainees should know how to recognize, treat and isolate patients with infectious disease in general and Ebola specifically.43 and 44 The 2013 Model of the Clinical Practice of Emergency Medicine goes further by listing within the domain of emergency medicine “understand[ing and apply[ing] the principles of disaster and mass casualty management including preparedness, triage, mitigation, response, and recovery.”45 Additional content areas in the Model relevant to Ebola response include the following: personal protection (equipment and techniques); universal precautions and exposure management; and emerging infections, pandemics and drug resistance.45 Together, these raise the issue of whether the current EVD outbreak should be viewed as an opportunity for trainees in emergency medicine and emergency nursing to care for patients during an international infectious disease epidemic. Few health care professionals in the United States have experience with the diagnosis and treatment of Ebola or the infection control precautions required to safely care for patients with this disease. Yet some such individuals may include trainees either with specific backgrounds in infectious diseases or previous experience with the PPE utilized in caring for such patients.
Historically, the outbreak of an unknown or uncommon infectious disease has led to initial concerns by health providers about the risk to self that ultimately gives way with time and knowledge to acceptance of an affirmative duty for trainees to learn to treat patients with these conditions. For example, the early fear and stigma surrounding HIV-infected patients in the 1980s gave way to a widely recognized duty to treat these patients and instill the same ethic in trainees.46 As knowledge of the pathophysiology and epidemiology of EVD and its implications for healthcare providers become more widely disseminated, a similar evolution may take place. However, based on the current conditions of the Ebola outbreak, it is likely that very few of these professionals will need to be called upon to fulfill this duty.
As long as the Ebola incidence in the United States remains low, each institution can and should manage its burden of suspected Ebola cases with a cadre of nurses and physicians highly trained in Ebola treatment and prioritize infection control. The ethical justification to restrict the number of caregivers who come in contact with Ebola-infected patients is that, given the limited experience with the disease in the United States, unnecessary exposure to infected patients would increase the risk to providers, other patients, and the public. It is prudent to limit the potential chain of infection when possible.
Because experienced or specially-trained nurses and attending physicians can effectively manage suspected or confirmed Ebola cases, trainee involvement is not required and would entail unnecessary risks to trainees and their patients. Trainees should, however, be fully prepared in case they find themselves in a position where their duty to treat an individual patient outweighs a duty to the public to limit exposure to the disease.44 However, if not trained or equipped properly, their duty to reasonably protect their own safety should not be superseded.
Non-participation of trainees in the care of Ebola-infected patients is then an instance of exclusion, rather than exemption. Institutions exclude trainees as an infection control strategy; trainees do not opt out. Some trainees may object to these policies, as they may feel ethically compelled to care for Ebola-infected patients as a function of their professional role and view their exclusion as a restriction of their own moral agency and liberty (to fulfill their commitment to treating the sick).39 However, this restriction is justified by the greater good of protecting public health. Ensuring trainee well-being and availability to care for other ED patients as well as limiting contagion are ethically justifiable reasons to exclude trainees. Exclusion of trainees from the care of Ebola-infected patients is not simply paternalistic because the primary aim is to protect patients and the public and represents a proportional response relative to the professionalism and moral agency consideration of trainees.47
At the same time, a blanket exclusion of trainees from the care of Ebola patients in the primary outbreak zone may be ethically inappropriate. If the trainee has the relevant experience and is able to meet the other requirements outlined above for volunteerism in the countries most affected by Ebola currently, a case-by-case evaluation would seem appropriate for supporting the participation of volunteering trainees in the international response where there is a desperate need for available healthcare providers.39 Such support would have the added benefit of growing the cadre of individuals with the relevant expertise in caring for patients with EVD should the current outbreak spread to the US. However, it is worthy of consideration whether academic medical centers can appropriately manage the risk to their trainees in the conditions posed by the outbreak in West Africa. There are additional reputational risks should a trainee contract Ebola or the public adversely view institutions where a large cadre of providers, including trainees, have traveled to care for patients in the primarily affected countries.39
As such, we affirm the ethical appropriateness of academic medical centers to consider on an individual provider basis whether a trainee should be supported in volunteering to travel to Africa rather than endorsing a policy of automatic exclusion or support of providers in this regard. Such individualized evaluations should take specific account of the level of training, previous background, experience with Ebola and the PPE required to care for patients with this disease, the ability to undergo the necessary preparation for functioning effectively in the primary outbreak zone and the willingness to comply with monitoring and isolation protocols upon return to the US.
Is it Ethically Appropriate for Emergency Physicians or Emergency Nurses to Opt Out of the Care of Patients With EVD?
Under the current state of the Ebola outbreak, it is anticipated that cases in the US would be scattered and readily managed at designated treatment centers.41 At the same time, it is recognized that suspected patients may present to frontline emergency departments without specialized expertise in the management of EVD,42 and, as seen in the case of the patient in Dallas, this may pose a risk to health care providers, including emergency physicians and emergency nurses.3 As a result, various health care providers have expressed reluctance to care for patients with Ebola.48, 49, 50 and 51 Historically, such provider reluctance has often arisen with the emergence of unknown infectious diseases.29 A 2008 survey of thousands of healthcare workers in New York found that half would hesitate or refuse to report to work during a Severe Acute Respiratory Syndrome (SARS) outbreak (though 84% would report to work during a mass casualty situation). Most cited concern for family, followed by concern for self, as reasons not to report to work during a SARS epidemic. 52 Individual conscience then, rather than professional tradition, seems to be the main force that compels nurses and physicians to risk their lives in the service of patients. 29 and 46
With this background, it is fair to ask whether there are circumstances under which emergency department providers could opt out of the care of Ebola patients. Under US law, nurses and physicians have a legal duty to treat patients with whom they have entered into a therapeutic relationship. Once undertaken, the duty continues until the patient and professional mutually agree to end the relationship or the care is transferred to another professional.53 Nurses and physicians have special duties in service of the sick, and since this obligation holds even in face of greater than usual risks to one’s own safety, healthcare professionals consequently accept greater risks than ordinary, balancing immediate benefits to individual patients with the professional’s own health and ability to treat future patients.54 But there is no consensus on the specific limits of this duty.30 and 55
Emergency nurses and physicians are the front line in an outbreak and, implicit in their specialty choice, accept additional risk beyond what is typical for many of their colleagues. As noted above, this is acknowledged in professional codes of ethics and statutory mandates (e.g., EMTALA).21, 22, 23, 24 and 26 There are potential additional penalties for those health care professionals who refuse to work or treat patients during a pandemic, including reduction in pay, termination and, in some states that have adopted variations of the Model State Emergency Health Powers Act (MHEHPA), the possibilities of licensure actions, fines or imprisonment.56 and 57
Though the legal foundations of the duty to treat and its consequences are significant, the most compelling ground for these obligations is that health care is a moral enterprise.29 and 58 “All its efforts converge ultimately on decisions and actions which are presumed to be good for some person in need of help and healing.”58 Nurses and physicians have a professional commitment to healing the sick. They are morally accountable to this commitment and are expected to demonstrate the virtues that it entails—such as courage, compassion and fidelity.29 and 59 This virtue-based ethics is independent of the patient’s right to access to healthcare and the contract between the patient and physician. Rights-based and contract-based accounts of the duty to treat would allow nurses and physicians to opt out of caring for patients in an epidemic as long as others were willing to take their place.28 But nurses and physicians who opt out in such cases still fall short of their moral commitment.29
Emergency nurses and physicians, therefore, have a duty to care for Ebola-infected patients and, in most instances, accept the associated risks.30 and 60 But the duty is not unlimited. An “abstract limitless duty” obscures the discussion about reasonable risk acceptance among nurses and physicians.60 Allowing for reasonable and practical limits to the duty to treat—applied equitably to all clinicians—may increase the likelihood that nurses and physicians will live up to their individual obligations during an outbreak.30
The limit is illustrated by an account of a physician who, during the 1995 Ebola outbreak in the Democratic Republic of the Congo, “found 30 dying patients in an abandoned hospital, left to care for themselves amid rotting corpses, sometimes in the same bed.”30 A nurse or physician should not be expected to treat patients in a context where the risks are extraordinarily high and the potential benefit to patients extremely low.30 Indeed, the first duty of emergency nurses and physicians in the current Ebola outbreak or other emerging infectious disease is to protect themselves in the care of patients, if for no other reason than to ensure their availability to treat subsequent patients.61 By contrast, care of Ebola-infected patients in a US hospital with the proper PPE and training would fall well within the duty to treat.15
In the current state of the Ebola outbreak, establishing cadres of highly trained clinicians at well-resourced institutions may be the best way to deliver uniform care under a duty to treat and limit potential spread of infection in the US.42 Under the above-noted virtue and professionalism-based ethical framework,23, 24, 26, 58 and 59 emergency nurses and physicians may also volunteer in place of colleagues who they see experiencing exceptional moral or emotional distress over caring for Ebola-infected patients—for example, as a result of unusually severe consequences for loved ones should they become ill. But as the burden of Ebola-infected patients rises, the duty to treat is a responsibility of all emergency nurses and physicians who have the necessary training, skills and experience.
While the duty to treat is intrinsic to health care professionals, institutions may also hold emergency nurses and physicians accountable to this standard. However, institutions may not invoke the duty to treat to coerce hospital employees into accepting unnecessarily dangerous conditions: for example, to expect them to deliver care to Ebola-infected patients without proper PPE or training. Institutional leaders have an ethical responsibility to prepare for outbreaks, ensure that the providers who risk their lives in the service of patients do so with as much protection and support as possible and make available appropriate channels for emergency physicians and nurses to communicate concerns about the adequacy of the training and preparation they receive. Preparation includes, but is not limited to, making high-quality PPE readily available, ensuring that all relevant staff is educated and trained to use it properly (especially proper donning and doffing) and limiting exposure to only those individuals needed to care for patients and prevent the spread of infection.
Experience with the 2003 SARS epidemic in Canada suggests that hospital leaders owe even more than merely providing equipment and training to nurses and physicians who fulfill their duty to treat under hazardous conditions. Some healthcare workers died from SARS, and some spread the disease to their families.55 Healthcare workers have moral obligations to their families, and institutions should make it possible for them to care for patients without abandoning their responsibility to their families or risking their families’ lives. Institutions should, for example, assist with childcare and provide temporary living quarters to reduce the risk of disease transmission to family members and the associated anxiety and moral distress.62 Institutions, as well as public health agencies, may also consider additional acts of reciprocity toward healthcare workers who fulfill their duty to treat, such as insurance to protect them and their families should they become ill or die as a result of caring for Ebola-infected patients. Ultimately, however, emergency nurses and physicians care for the sick primarily out of personal moral obligation; financial incentives alone are not likely to increase the likelihood that they will discharge their duty under epidemic conditions.63
The protections that institutions and society provide healthcare workers—for themselves and their families—are ethically required. Just as emergency nurses and physicians may not generally opt out of caring for the sick, institutions and communities may not opt out of caring for healthcare professionals and their families. In sum, the duty to treat patients with infectious diseases, including Ebola, is both a legal responsibility and an ethical obligation of the healthcare professions. The duty should be borne equitably by professionals, who in turn, should be adequately supported by institutions and society as a whole.
Given the expected low number of US cases, there is a role for institutions to ask healthcare providers to volunteer to serve on treatment teams for suspected Ebola patients as a means of limiting training efforts, time and expenditures (eg, credentialing of the ability to perform invasive procedures with PPE), reducing the potential risk of infection and ensuring relevant personnel and expertise are available to provide care. However, such volunteer-based plans do not address the special role of emergency departments where patients may present in an undifferentiated manner and potentially in acute distress, and where alternative providers may simply not be available. For emergency physicians and nurses, who through their choice of profession knowingly accept the above circumstances of patient care,23 and 24 the current state of the Ebola outbreak does not justify opting out of the care of suspected or confirmed Ebola patients who may present to the emergency department, but this obligation is contingent upon institutional and governmental resources that provide adequate training and equipment to fulfill this duty. There also needs to be a recognition by healthcare personnel, hospitals and other public health and legal authorities as well as patients that the duty of emergency physicians and nurses to treat must be absolutely contingent on first ensuring personal safety through the proper use of PPE.61 and 64 Should Ebola rise in prevalence in the US, contingency planning to meet the duty to treat should move beyond training and equipment to mechanisms to support the weighty obligations of emergency physicians and nurses to protect themselves and their families while caring for affected patients.
Are the Goals of Care Different in Patients Critically Ill with EVD?
With the high mortality rate, lack of specific treatment and need for specialized PPE in order to prevent transmission, there have been legitimate questions whether the goals of care should change in patients critically ill with EVD. Specifically, in the circumstance where a patient requires procedural interventions (central venous access, intubation, dialysis, etc) to provide intensive care level support, is the risk posed to providers too high compared to the low potential of benefit, if any, to a patient whose illness may have progressed to a point where such interventions are unlikely to be successful? Furthermore, given the time needed to don PPE—an absolute requirement prior to any procedural intervention on an EVD patient—should cardiopulmonary resuscitation during an arrest event be considered futile due to the potential delay in its initiation and again the likely prognosis of the patient?11, 64 and 65
Since the initial posing of these concerns about the risk versus benefit posed by critical care and resuscitation interventions in patients with EVD, case reports have appeared showing that aggressive, intensive care level interventions, including intubation, central venous access, large volume and blood resuscitation and dialysis, can be successful in treating critically ill individuals with this disease and do not pose an automatic risk to providers if PPE is properly used.66 and 67 While anecdotal and representative more of what is possible in idealized circumstances (specialized care units with previous expertise and training in care of EVD patients and a high number of dedicated providers), these cases imply that utilizing the full panoply of critical care resources for this patient population may be appropriate treatment. However, the highly contagious nature of EVD and the need for specialized PPE, along with the experience in Africa of rapid transmission to family members caring for ill patients, makes it appropriate for hospitals to not allow family presence during such procedures as is allowed in other critical care or resuscitation circumstances.
With respect to cardiopulmonary resuscitation, to our knowledge, no published report has indicated the successful or unsuccessful use of cardiopulmonary resuscitation in an arrest event in an Ebola patient, through resuscitation success in a US healthcare facility may be similar to other infectious diseases at similar stages, from initial manifestations to overwhelming sepsis. At this time, consideration of do-not-resuscitate status in a late-stage EVD patient is best determined on a case-by-case basis, taking into account potential benefit to the patient, any limitations of interventions imposed by the disease and the potential risks to the treatment team.
However, the circumstances described for the above patients are not typical of that seen in most emergency departments in the US. While the current state of the outbreak would likely lead to a typical ED encountering a patient early in their EVD process, if at all, and being able to isolate such an individual until transfer to a higher level of care, should the number of cases rise due to spread of the disease, it is conceivable that emergency departments could encounter patients in a variety of stages of Ebola with the risk-benefit calculation on procedural interventions being highly relevant. Unlike the above cases, should the current outbreak spread, emergency departments would encounter patients with fewer resources (fewer isolation facilities, lower ratios of providers to the patient) than those expended in the above-reported cases and having to simultaneously care for other patients with a variety of conditions. Here there is a need to refer to the special role played by emergency physicians and nurses in the healthcare system. The assumptions that accompany the choice of these professional roles (exposure to acutely ill, undifferentiated patients) and the specialized training and skills that emergency physicians and nurses possess impose a higher obligation than other medical professionals to be prepared to treat an acutely ill Ebola patient in the emergency department setting.23 and 24
At the same time, as we noted above, the duty to treat is not absolute. There is no obligation for an emergency physician or nurse to implement treatment measures in an acutely ill Ebola patient without training in the use of PPE, the availability of such supplies and, at a minimum, simulated experience with performing critical care procedures while utilizing PPE.15, 28 and 61 Without such minimum standards, the social contract that accompanies the professional standing and obligations of emergency physicians and nurses breaks down. This social contract calls for a rational person to expect an emergency physician or nurse to apply their skills to aid an acutely ill patient but at the same time for those professionals to have the requisite training and equipment to provide such aid in an appropriate manner.68
All emergency departments and hospitals should, therefore, consider that protocols for PPE training and isolating suspect patients, as called for in the current interim CDC guidelines,42 are likely inadequate should the current epidemic spread more prominently to the US. To fulfill the ethical obligations imposed by the duty to treat should the current outbreak become more prevalent domestically, more robust training with PPE and the performance of procedures with such equipment will be necessary for a wider cadre of emergency physicians and nurses to appropriately treat acutely ill Ebola patients in intermediate or late stages of the disease while ensuring the maximum feasible protection of the healthcare provider. Weighing when such expanded training may be warranted should take into account the continued status of the outbreak, the cost of such preparation and the availability of appropriate resources to be effective.
In the unexpected scenario where the number of patients with EVD overwhelms existing resources, more traditional disaster triage protocols would be applicable. Such protocols attempt to apply resources in a manner to benefit the largest number of patients. In the case of Ebola, where the evidence to date is that an overwhelming amount of critical care resources are required to effectively treat a late-stage patient, disaster triage protocols would need to weigh at what point in the treatment spectrum such resource expenditure would become untenable. Such protocols, to be ethically appropriate, would need to be transparent, proportionate and accountable to oversight along with having a legal imprimatur to be effective in the emergency department and acute care setting.69 To avoid such a crisis situation, the devotion of resources now to end the epidemic in the primary outbreak zone in Africa is vital.
Ebola Virus Disease Patients Should not Receive CPR Future Considerations
The outbreak of EVD in West Africa has presented a significant challenge to the health systems of the primarily affected nations and, even with a low case count, raised concerns about the preparedness of the US healthcare system to respond to uncommon infectious diseases. In some ways, Ebola is a unique test for US emergency departments, emergency physicians, emergency nurses, and other stakeholders are given its rarity in the US, high mortality rate, high risk of transmission to healthcare staff and non-specific presenting symptoms that can make initial diagnosis more difficult. However, as shown with other unanticipated infectious disease outbreaks (HIV, SARS, MERS), emergency departments will almost certainly be a key location for patient identification and treatment. The ethical concepts applied in this paper are relevant, especially reciprocity, duty to treat and grounding in the specific facts of the disease process in question when considering how acute care facilities should prepare for likely future outbreaks of infectious disease. We propose that preparation for future emergency department responses to unanticipated infectious disease outbreaks should include ethical as well as logistical and medical factors.69 Given the multiple stakeholders represented in emergency department practice, the model shown here of multi-disciplinary and organizational consideration of the ethical issues involved would likely have application when considering the approach to future infectious disease challenges.
Ebola Virus Disease Patients Should not Receive CPR Conclusion
The outbreak of EVD in West Africa and the presentation of patients to US acute care facilities have raised a series of intertwined logistical and ethical issues of relevance to US emergency departments, emergency physicians and emergency nurses. While the current state of the epidemic has not led to a large number of EVD patients presenting to US facilities, consideration of ethical questions that are relevant now and of potential relevance in the future will allow emergency physicians, emergency nurses and other stakeholders to prepare appropriately for the challenges posed by Ebola and consider its implications for future epidemic infectious disease events. An emphasis on the principle of reciprocity, the obligations imposed by and underlying assumptions of the duty to treat and the specific characteristics of the disease process will aid in addressing the ethical challenges posed in the current outbreak of EVD.
Acknowledgments
The drafting authors wish to thank the ACEP Ebola Expert Panel and SAEM Global Academy of Emergency Medicine for their critical review of the manuscript during preparation and the leadership of ACEP, ENA, and SAEM for their sponsorship of this effort.
References
1
Centers for Disease Control and Prevention
Ebola outbreak in West Africa—case counts
http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html (2014) Updated February 4, 2015. Accessed February 5, 2015
2
R Dunklin, S Thompson
ER doctor discusses the role in Ebola patient’s initial misdiagnosis
Dallas Morning News (2014) http://www.dallasnews.com/ebola/headlines/20141206-er-doctor-discusses-role-in-ebola-patients-initial-misdiagnosis.ece, Accessed February 5, 2015
3
G Botelho, J Hanna, A Fantz
Nurse’s discharge leaves one Ebola case in the U.S., though larger battle continues. CNN Web site
http://www.cnn.com/2014/10/28/health/us-ebola/ Accessed February 5, 2015
4
A Hartocollis, M Santora
Plenty of hugs as Craig Spencer, recovered New York Ebola patient, goes home
N Y Times (2014) http://www.nytimes.com/2014/11/12/nyregion/craig-spencer-new-york-ebola-patient-bellevue.html?_r=0, Accessed February 5, 2015
5
C Moskowitz
Are U.S. Hospitals Prepared for the Next Ebola Case?
Sci Am (2014) Available from http://www.scientificamerican.com/article/are-us-hospitals-prepared-for-the-next-ebola-case/, Accessed February 5, 2015
6
A Soergel
Ebola quarantine questioned
US News and World Report (2014) http://www.usnews.com/news/newsgram/articles/2014/10/27/ebola-ethics-quarantine-questioned, Accessed February 5, 2015
7
American College of Emergency Physicians
Healthcare resources for suspected Ebola cases
http://www.acep.org/ebola/ Published 2014, Accessed February 5, 2015
8
Emergency Nurses Association
ENA topic brief: Ebola virus disease
http://www.ena.org/practice-research/Practice/Documents/EbolaTopicBrief.pdf Accessed February 5, 2015
9
Centers for Disease Control and Prevention
Ebola (Ebola virus disease)
http://www.cdc.gov/vhf/ebola/ Updated February 4, 2015, Accessed February 5, 2015
10
R Perl
Ebola response reveals a double standard in U.S. health care
Forbes (2014) http://www.forbes.com/sites/robertpearl/2014/12/11/ebola-double-standard/, Accessed February 5, 2015
11
L Altman
Ethicist calls CPR too risky in Ebola
N Y Times (2014) http://www.nytimes.com/2014/10/21/health/-ethicist-calls-cpr-too-risky-in-ebola-.html, Accessed February 5, 2015
12
N Kass
Ebola, ethics, and public health: what next?
Ann Intern Med, 161 (10) (2014), pp. 744–745
Full Text via CrossRef | View Record in Scopus | Citing articles (13)
13
Toner E, Adalja A, Inglesby T. A primer on Ebola for clinicians published online ahead of print October 17, 2014. Disaster Med Public Health Prep.
14
G Donovan
Ebola, epidemics, and ethics—what we have learned
Philos Ethics Humanit Med, 9 (2014), p. 15
Full Text via CrossRef
15
K Koenig, C Majestic, M Burns
Ebola virus disease: essential public health principles for clinicians
West J Emerg Med, 15 (7) (2014), pp. 728–731
Full Text via CrossRef | View Record in Scopus | Citing articles (9)
16
L Meyers, T Frawley, S Goss, et al.
Ebola virus outbreak 2014: the clinical review for emergency physicians
Ann Emerg Med, 65 (1) (2015), pp. 101–108
Article | PDF (1103 K)
| View Record in Scopus | Citing articles (14)
17
H Feldmann, T Geisbert
Ebola hemorrhagic fever
Lancet, 377 (9768) (2011), pp. 849–862
Article | PDF (2175 K)
| View Record in Scopus | Citing articles (429)
18
Centers for Disease Control and Prevention
Review of human-to-human transmission of Ebola virus
http://www.cdc.gov/vhf/ebola/transmission/human-transmission.html Updated October 29, 2014, Accessed February 5, 2015
19
L Sun, B Dennis
U.S. hospitals wary of caring for Ebola patients because of cost and stigma
The Washington Post (2014) http://www.washingtonpost.com/national/health-science/us-hospitals-wary-of-caring-for-ebola-patients-because-of-cost-and-stigma/2014/11/28/928aa2bc-71cc-11e4-893f-86bd390a3340_story.html, Accessed February 5, 2015
20
J Pines, R Mutter, M Zocchi
Variation in emergency department admission rates across the United States
Med Care Res Rev, 70 (2013), pp. 218–231
Full Text via CrossRef | View Record in Scopus | Citing articles (35)
21
Emergency Treatment and Active Labor Act (EMTALA), 42 USC §1395dd
(2008)
22
Center for Clinical Standards and Quality/Survey and Certification Group
Center for Medicare and Medicaid Services. Emergency Medical Treatment and Labor Act (EMTALA) requirements and implications related to Ebola virus disease (Ebola)
http://www.aha.org/content/14/141121-sc15-10emtala-ebola.pdf Published November 21, 2014. Accessed February 5, 2015
23
American College of Emergency Physicians
Code of ethics for emergency physicians
http://www.acep.org/Clinical—Practice-Management/Code-of-Ethics-for-Emergency-Physicians/ Accessed February 5, 2015
24
Emergency Nurses Association
ENA code of ethics
http://www.ena.org/about/ethics/Pages/Default.aspx Accessed February 5, 2015
25
Society for Academic Emergency Medicine
SAEM mission statement
http://www.saem.org/about-saem/mission Accessed February 5, 2015
26
American Medical Association
Opinion 9.067—Physician obligation in disaster preparedness and response
http://www.ama-assn.org.vlib.excelsior.edu/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion9067.page Accessed February 5, 2015
27
American Nurses Association
Code of ethics for nurses
http://www.nursingworld.org/codeofethics Accessed February 5, 2015
28
H Malm, T May, L Francis, et al.
Ethics, pandemics, and the duty to treat
Am J Bioeth, 8 (8) (2008), pp. 4–19
Full Text via CrossRef | View Record in Scopus | Citing articles (44)
29
A Zuger, S Miles
Physicians, AIDS, and occupational risk: historic traditions and ethical obligations
JAMA, 258 (14) (1987), pp. 1924–1928
Full Text via CrossRef | View Record in Scopus | Citing articles (110)
30
D Sokol
Virulent epidemics and scope of healthcare workers’ duty of care
Emerg Infect Dis, 12 (8) (2006), pp. 1238–1241
Full Text via CrossRef | View Record in Scopus | Citing articles (52)
31
W Austin
Ethics in a time of contagion: a relational perspective
Can J Nurs Res, 40 (4) (2008), pp. 10–24
View Record in Scopus | Citing articles (7)
32
World Health Organization
Statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa
http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/ Published August 8, 2014, Accessed February 5, 2015
33
Wildes R, Kayden S, Goralnick E, et al. Sign me up: rules of the road for humanitarian volunteers during the Ebola outbreak published online ahead of print October 24, 2014. Disaster Med Public Health Prep.
34
E Weiner
The nursing curriculum for emergency preparedness
http://www.nursing.vanderbilt.edu/advantage/emergency.html Accessed February 5, 2015
35
George Washington University School of Nursing
The National Nurse Emergency Preparedness Initiative (NNEPI)
http://nnepi.gwnursing.org/ Accessed February 5, 2015
36
Centers for Disease Control and Prevention
For general healthcare settings in West Africa: four keys to infection control
http://www.cdc.gov/vhf/ebola/hcp/international/keys-to-infection-control.html Updated December 19, 2014, Accessed February 5, 2015
37
M McCarthy
CDC rejects mandatory quarantine for travelers arriving from Ebola-stricken nations
BMJ, 349 (2014), p. g6499
Full Text via CrossRef | View Record in Scopus | Citing articles (3)
38
ACEP Ebola Expert Panel
Consensus statement on restrictive movement including quarantine of health care workers
http://www.acep.org/uploadedFiles/ACEP/practiceResources/issuesByCategory/publichealth/ACEP%20Ebola%20Expert%20Panel%20Consensus%20Statement.111314.pdf Published November 13, 2014, Accessed February 5, 2015
39
L Rosenbaum
License to Serve — U.S. Trainees and the Ebola Epidemic
New England Journal of Medicine, 372 (6) (2015), pp. 504–506
Full Text via CrossRef | View Record in Scopus | Citing articles (7)
40
Academic Consortium Combating Ebola in Liberia. http://accel.mit.edu/. Accessed December 30, 2014.
41
Centers for Disease Control and Prevention
Current Ebola Treatment Centers
http://www.cdc.gov/vhf/ebola/hcp/current-treatment-centers.html Accessed December 22, 2014
42
Centers for Disease Control and Prevention
Interim guidance for U.S. hospital preparedness for patients under investigation (PUIs) or with confirmed Ebola virus disease (EVD): a framework for a tiered approach
http://www.cdc.gov/vhf/ebola/hcp/us-hospital-preparedness.html Updated January 22, 2015, Accessed February 5, 2015
43
Accreditation Council for Graduate Medical Education
ACGME program requirements for graduate medical education in emergency medicine
https://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQ-PIF/110_emergency_medicine_07012013.pdf Published July 1, 2013, Accessed February 5, 2015
44
Accreditation Council for Graduate Medical Education
ACGME guidance statement on Ebola virus infection and resident/fellow training in the United States
https://www.acgme.org/acgmeweb/Portals/0/PDFs/Nasca-Community/ACGME-GME-Ebola-Final1.pdf Published October 2014, Accessed February 5, 2015
45
FL Counselman, MA Borenstein, CD Chisholm, et al.
The 2013 model of the clinical practice of emergency medicine
Acad Emerg Med, 21 (5) (2014), pp. 574–598
Full Text via CrossRef | View Record in Scopus | Citing articles (17)
46
R Bayer, GM Oppenheimer
AIDS Doctors: Voices From the Epidemic: An Oral History
Oxford University Press, Oxford, UK (2002)
47
JF Childress, RR Faden, RD Gaare, et al.
Public health ethics: mapping the terrain
J Law Med Ethics, 30 (2) (2002), pp. 170–178
Full Text via CrossRef | View Record in Scopus | Citing articles (257)
48
BBC News
Ebola: When health workers’ duty to treat is trumped
http://www.bbc.com/news/health-29573993 Published October 29, 2014, Accessed February 5, 2015
49
L Gruson
Montana nurses concerned about Ebola
Great Falls Tribune (2014) http://www.greatfallstribune.com/story/news/local/2014/10/15/montana-nurses-concerned-ebola/17340921/, Accessed February 5, 2015
50
J Schram, L Celona
Bellevue staffers call in “sick” after Ebola arrives
New York Post (2014) http://nypost.com/2014/10/25/many-bellevue-staffers-take-sick-day-in-ebola-panic/, Accessed February 5, 2015
51
Fox News
Hospital staffers reportedly take sick day rather than treat New York’s first Ebola patient
http://www.foxnews.com/health/2014/10/25/hospital-staffers-reportedly-take-sick-day-rather-than-treat-new-yorks-first/ Published October 25, 2014, Accessed February 5, 2015
52
K Qureshi
Health care workers’ ability and willingness to report to duty during catastrophic disasters
J Urban Health, 82 (3) (2005), pp. 378–388
Full Text via CrossRef | View Record in Scopus | Citing articles (184)
53
Payton v. Weaver, 131 Cal App 3d 38, 182 Cal Rptr 225 (Cal App 1 Dist 1982).
54
K Morin, D Higginson, M Goldrich
for the Council on Ethical and Judicial Affairs of the American Medical Association. Physician obligation in disaster preparedness and response
Camb Q Healthc Ethics, 15 (2006), pp. 417–421
View Record in Scopus | Citing articles (8)
55
P Singer, S Benatar, M Bernstein, et al.
Ethics and SARS: lessons from Toronto
BMJ, 327 (7427) (2003), p. 1342
Full Text via CrossRef | View Record in Scopus | Citing articles (90)
56
Center for Law and the Public’s Health
Model State Emergency Health Powers Act
http://www.publichealthlaw.net/MSEHPA/MSEHPA.pdf Accessed February 5, 2015
57
C Coleman, A Reis
Potential penalties for health care professionals who refuse to work during a pandemic
JAMA, 299 (2008), pp. 1471–1473
Full Text via CrossRef | View Record in Scopus | Citing articles (15)
58
E Pellegrino
Ethics and the moral center of the medical enterprise
Bull N Y Acad Med, 54 (7) (1978), p. 625
View Record in Scopus | Citing articles (3)
59
E Pellegrino
Toward a virtue-based normative ethics for the health professions
Kennedy Inst Ethics J, 5 (3) (1995), pp. 253–277
Full Text via CrossRef | View Record in Scopus | Citing articles (99)
60
M Meerschaert
Physicians’ duty to participate in pandemic care
JAMA, 300 (3) (2008), p. 284
Full Text via CrossRef | View Record in Scopus | Citing articles (2)
61
Koenig K. Ebola triage screening and public health: the new “vital sign zero” published online ahead of print October 29, 2014. Disaster Med Public Health Prep.
62
L Hawryluck, S Lapinsky, T Stewart
Clinical review: SARS–lessons in disaster management
Crit Care, 9 (4) (2005), p. 384
Full Text via CrossRef | View Record in Scopus | Citing articles (28)
63
C Irvin, L Cindrich, W Patterson, et al.
Survey of hospital healthcare personnel response during a potential avian influenza pandemic: will they come to work?
Prehosp Disaster Med, 23 (2008), pp. 328–335
Full Text via CrossRef | View Record in Scopus | Citing articles (56)
64
American Society of Anesthesiology
Recommendations from the ASA Ebola Workgroup
http://www.asahq.org/For-Members/Clinical-Information/Ebola-Information/Ebola-Guidelines-from-COH.aspx Accessed February 5, 2015
65
J Fins
Responding to Ebola: questions about resuscitation
http://www.thehastingscenter.org/Bioethicsforum/Post.aspx?id=7135&blogid=140 Published October 10, 2014, Accessed February 5, 2015
66
B Kreuels, D Wichmann, P Emmerich, et al.
A case of severe Ebola virus infection complicated by gram-negative septicemia
N Engl J Med, 37 (2014), pp. 2394–2401
Full Text via CrossRef | View Record in Scopus | Citing articles (106)
67
G Lyon, A Mehta, J Varkey, et al.
Clinical care of two patients with Ebola virus disease in the United States
N Engl J Med, 371 (2014), pp. 2402–2409
Full Text via CrossRef | View Record in Scopus | Citing articles (109)
68
J Rachels, S Rachels
The Idea of a Social Contract: The Elements of Moral Philosophy
(6th ed.)McGraw-Hill, Boston, MA (2010)
69
Institute of Medicine
Crisis Standards of Care: A Systems Framework for Catastrophic Disaster Response
National Academies of Science, Washington, DC (2012)
For correspondence, write Arvind Venkat, MD, FACEP, Department of Emergency Medicine, Allegheny Health Network, 320 East North Avenue, Pittsburgh, PA 15212.
Vitae
Arvind Venkat (ACEP, SAEM), Department of Emergency Medicine, Allegheny Health Network, Pittsburgh, PA.
Lisa Wolf (ENA), Institute of Emergency Nursing Research, Des Plaines, IL.
Joel M. Geiderman (ACEP), Department of Emergency Medicine, Cedars-Sinai Medical Center, Los Angeles, CA.
Shellie L. Asher (SAEM), Department of Emergency Medicine, Albany Medical Center, Albany, NY.
Catherine A. Marco (ACEP), Department of Emergency Medicine, Boonshoft School of Medicine, Wright State University, Dayton, OH.
Jolion McGreevy (SAEM), Department of Emergency Medicine, Boston Medical Center, Boston University School of Medicine, Boston, MA.
Arthur R. Derse (ACEP), Center for Bioethics and Medical Humanities (Institute for Health and Society) and Department of Emergency Medicine, Medical College of Wisconsin, Milwaukee, WI.
Edward J. Otten (SAEM), Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH.
John E. Jesus (ACEP), Department of Emergency Medicine, Christiana Care Health System, Wilmington, DE.
Natalie P. Kreitzer (SAEM), Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH.
Monica Escalante (ENA), Institute for Quality, Safety and Injury Prevention, Des Plaines, IL.
Adam C. Levine (SAEM), Department of Emergency Medicine, Warren Alpert Medical School of Brown University, Providence, RI.
ED Ebola Triage Algorithm: A Tool and Process for Compliance
2015, Journal of Emergency Nursing
more
Nursing and complex humanitarian emergencies: Ebola is more than a disease
2015, Nursing Outlook
more
Arterial Blood Gas Review
2015, Journal of Emergency Nursing
more
View more articles »
Related book content
For this week you should:
1. Use the assigned readings, web and professional resources, and the M1A1 interactive tutorial to compose an initial discussion post M1D1, complete with in-text citations and references of a minimum of 250 words Carefully look at the AD Discussion Rubric prior to composing your post and make sure you answer every component of the discussion question.
2. Develop and post two (2) responses to the initial posts of two (2) different peers who have chosen a different idea than your initial post. Be sure to use the module content and reference it to support your post. Make every attempt to post on different days earlier in the week to provide a scholarly exchange of ideas. References, citations, repeating the question, and quoting your peer do not count towards the 100-word minimum.
nursing 104 modules 1 paper.
The RN is developing a plan of care for an 86 year old patient who was admitted after falling at home. The patient is confused to place and time and has a right hip fracture that will be repaired tomorrow.
Question:
Develop A plan of care for this patient that includes the actions the RN will take for each step of the nursing process. Be sure to include how critical thinking will be used in the development of the plan.
Please cite two references from the textbook APA style
Textbook to use for this paper: Treas, L. & Wilkinson, J, (2014). Basic nursing: concepts, skills & reasoning. Philadelphia; F. A. Davis, Company.
Specific areas & chapters to read and collect information for this paper?
Basic nursing: concepts, skills & reasoning**
• Chapter 2: Critical thinking and the nursing process
• Chapter 3: Assessment
• Chapter 4: Diagnosis
• Chapter 5: Planning Outcomes
• Chapter 6: Planning Interventions
• Chapter 7: Implementation and Evaluation
• Chapter 18: Documenting and Reporting
• Chapter 44: Nursing
• Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Nursing Diagnosis Guidebook – A pocket-size nursing diagnosis guidebook of your choice that is no more than one edition old, that includes NANDA International-approved nursing diagnoses, definitions, defining characteristics, and possible nursing Interventions.
Nur213 module 1 paper.
Using the assigned readings and information from the literature, compose a response to the following statement:
Question: Patients with Ebola virus disease (EVD) should not receive CPR.
For this activity, you will weigh in on the RN’s ethical obligation when providing care to patients with EVD and the performance of CPR.
Please cite two references from the textbook APA style
Required Textbooks and assigned reading for this paper:
Brunner and Suddarth’s textbook of medical-surgical nursing**
• Chapter 3: Critical Thinking, Ethical Decision Making, and the Nursing Process
• Chapter 23: Management of Patients With Chest and Lower Respiratory Tract Disorders (section on “Pulmonary Tuberculosis”)
• Chapter 35: Assessment of Immune Function (section on “Function of the Immune System”)
• Chapter 37: Management of Patients With HIV Infection and AIDS
• Chapter 42: Management of Patients with Musculoskeletal Disorders (section on Musculoskeletal Infections”).
• Chapter 49: Assessment and Management of Patients With Hepatic Disorders (sections on “Viral Hepatitis, “Hepatitis A, B, and C”, and “Nonviral Hepatitis”)
• Chapter 55: Management of Patients With Urinary Disorders (sections on “Infections of the Urinary Tract”)
• Chapter 69: Management of Patients With Neurologic Infections, Autoimmune Disorders, and Neuropathies (section on “Infectious Neurologic Disorders”)
• Chapter 71: Management of Patients with Infectious Diseases
Pharmacology: A patient-centered nursing process approach**
• Chapter 14: Medications and Calculations
• Chapter 29: Penicillins and Cephalosporins
• Chapter 31: Sulfonamides
• Chapter 32: Antituberculars, Antifungals, Peptides, and Metronidazole
• Chapter 34: Drugs for Urinary Tract Disorders
• Chapter 36: Vaccines
Maternal & Child Health Nursing**
• Chapter 40: Nursing is of a Family When a Child has a Respiratory Disorder (section on Disorders of the lower respiratory tract: influenza and tuberculosis)
• Chapter 42: Nursing Care of a Family When a Child has an Immune Disorder
• Chapter 43: Nursing Care of a Family When a Child has an Infectious Disorder (section on “Infection”)
•Chapter 45: Nursing Care of a Family When a Child has a Gastrointestinal Disorder (section on “Hepatitis”)
• Chapter 49: Nursing Care of a Family When a Child has a Neurologic Disorder (section on “Bacterial Meningitis”)
• Chapter 51: Nursing Care of a Family When a Child has a Musculoskeletal Disorder (section on “Infectious and Inflammatory Disorders of the Bones and Joints”)
Nursing Diagnosis
• Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Web-based and Other Professional Resources:
• Hand Hygiene in Healthcare Settings
• Hospital: 2016 National Patient Safety Goals**
• Pre-licensure KSAs (2014)**
• Ebola virus disease: an emerging threat (2014)**
• Zika virus (2016)**
M1D1: The Ethical Obligations of the RN Providing care to the Patient with Ebola Virus Disease
Ethical Issues in the Response to Ebola Virus Disease in US Emergency Departments: A Position Paper of the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine
Arvind Venkat, MD, FACEP, ,
Lisa Wolf, PhD, RN, CEN, FAEN,
Joel M. Geiderman, MD, FACEP,
Shellie L. Asher, MD, FACEP,
Catherine A. Marco, MD, FACEP,
Jolion McGreevy, MD, MBE, MPH,
Arthur R. Derse, MD, JD, FACEP,
Edward J. Otten, MD, FACMT, FAWM,
John E. Jesus, MD, FACEP,
Natalie P. Kreitzer, MD,
Monica Escalante, MSN, BA, RN,
Adam C. Levine, MD, MPH, FACEP,
on behalf of the
American College of Emergency Physicians,
the
Emergency Nurses Association,
and the
Society for Academic Emergency Medicine
Show more
http://dx.doi.org.vlib.excelsior.edu/10.1016/j.jen.2015.01.012Get rights and content
Referred to byAnne Manton
Editor’s Note regarding the on-line position paper, “Ethical Issues in the Response to Ebola Virus Disease in US Emergency Departments: A Position Paper of the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine”
Journal of Emergency Nursing, Volume 41, Issue 2, March 2015, Page 99
PDF (58 K)
M1D1: The Ethical Obligations of the RN Providing care to the Patient with Ebola Virus Disease
The 2014 outbreak of Ebola Virus Disease (EVD) in West Africa has presented a significant public health crisis to the international health community and challenged US emergency departments to prepare for patients with a disease of exceeding rarity in developed nations. With the presentation of patients with Ebola to US acute care facilities, ethical questions have been raised in both the press and medical literature as to how US emergency departments, emergency physicians, emergency nurses and other stakeholders in the healthcare system should approach the current epidemic and its potential for spread in the domestic environment. To address these concerns, the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine developed this joint position paper to provide guidance to US emergency physicians, emergency nurses and other stakeholders in the healthcare system on how to approach the ethical dilemmas posed by the outbreak of EVD. This paper will address areas of immediate and potential ethical concern to US emergency departments in how they approach preparation for and management of potential patients with EVD.
Keywords
Ethics;
Ebola virus disease;
Emergency department
Introduction
In March 2014, an outbreak of Ebola Virus Disease (EVD) was confirmed in the West African nation of Guinea with subsequent rapid spread to the neighboring countries of Liberia and Sierra Leone. Given the underdeveloped health infrastructures in the 3 primary affected nations and the high transmission and mortality rate of the disease, domestic and international public health agencies called for aid and personnel to be rapidly deployed to the affected nations to treat infected patients and prevent further spread of the Ebola outbreak. Yet despite significant efforts from the international community, EVD continues to represent a significant challenge in the region. As of January 2015, the Centers for Disease Control and Prevention (CDC) reports that the total case count stands at 21,689 with 8,626 deaths and continues to rise.1
In the United States, the transfer of Ebola-infected healthcare workers from the outbreak zone to US hospitals raised public awareness and fear of the spread of the disease. This fear was heightened after the initial missed diagnosis in a US emergency department of a patient with EVD who later died,2 the transmission of Ebola to 2 nurses who cared for this patient3 and a subsequent case of an emergency physician who traveled to West Africa to care for patients with EVD and required hospitalization after returning to the United States.4 These cases raised significant concerns that US emergency departments and hospitals were not adequately prepared to diagnose and treat patients with EVD. In addition, the infection of healthcare personnel created the specter of a more widespread outbreak in the general population due to poor infection control guidelines, inadequate training, and management protocols in US medical centers and initially absent mechanisms to identify potentially infected individuals arriving through US ports of entry.5 A subsequent controversy surrounding a nurse who returned from West Africa without symptoms of EVD and was held in quarantine highlighted concerns about how personal liberty and public health should be appropriately balanced.6 In response, both emergency medicine and emergency nursing organizations and federal agencies have issued guidance on the nature of EVD, approaches to identification, isolation, and treatment of potential patients and standards for use of personal protective equipment (PPE) by healthcare providers.7, 8 and 9
While the number of cases in the United States remains low to date (10 total patients, 4 diagnosed in the US and 2 deaths), the outbreak of EVD has raised ethical issues relevant to US emergency departments and hospitals, emergency physicians and emergency nurses. Issues articulated in the medical literature and by the press include the following: how resources should be used in preparation for the likely rare event of an undiagnosed patient with EVD who presents to a US emergency department,10 whether there should be a different standard for care of Ebola-infected patients than for other patients with less contagious and lethal diseases11 and whether healthcare providers are obligated to place themselves at a significant degree of risk while caring for these patients due to their professional status.12 To address these concerns, the American College of Emergency Physicians (ACEP), the Emergency Nurses Association (ENA), and the Society for Academic Emergency Medicine (SAEM) developed this joint position paper to provide guidance to US emergency physicians, emergency nurses and other stakeholders in the healthcare system on how to approach the ethical issues posed by the outbreak of EVD. This paper will address areas of immediate and potential ethical concern to US emergency departments in how they approach preparation for and management of potential patients with EVD.
Characteristics of EVD of Ethical Relevance
Since the outbreak of EVD, numerous articles have been published on the epidemiologic characteristics of this condition and the microbiological details of the causative organism.13, 14, 15 and 16 However, particular characteristics of EVD are worth highlighting to provide the factual basis for addressing the ethical questions raised in this outbreak for US emergency departments. First, it is well recognized that individuals with EVD will often have relatively non-specific symptoms, common to many viral infections, in their initial stages of presentation (eg, fever, headache, myalgias).15 and 17 Such non-specific presentations make unrecognized infection with Ebola a realistic concern. Lack of prompt identification of potential patients by emergency department staff can increase the risk of spread of the disease and mandates a heightened awareness of the risk factors for the disease. Second, the pathophysiology of contagion is related to contact with blood or bodily fluids from an infected individual, with rising viremia in the late stages of disease presenting a particular risk for human-to-human transmission. However, even a low level of viral inoculation can lead to EVD.18 This recognized pathway of spread aids in evaluating the risk of transmission from patient to healthcare providers or the general public. At the same time, knowledge of how the Ebola virus is transmitted heightens the ethical concerns posed by the potential presence of highly symptomatic and contagious patient(s) to an emergency department, especially if to a center without specialized experience in the care of EVD patients. Finally, the lack of specific effective treatment and the high mortality rate posed by EVD exacerbates public fears, may create irrational panic relative to the actual risk and lead to unexpected institutional consequences such as the avoidance of the use of healthcare facilities where EVD patients are being or have been treated.
Ebola Virus Disease Patients Should not Receive CPR and Characteristics of Emergency Department Practice of Ethical Relevance
The emergency department in the United States and increasingly worldwide serves as the primary gateway to the acute healthcare system. It is estimated that 50% of admissions to hospitals in the US are initially assessed and treated in emergency departments.20 The emergency department is also the only access point in the US acute healthcare system available to patients 24 hours per day-7 days per week. In the US there is a legal obligation under EMTALA to provide a medical screening exam for an emergency medical condition and treatment until the emergency medical condition is resolved or stabilized to the extent of that hospital’s capability (until appropriate transfer) regardless of insurance status or other socioeconomic factors.21 and 22 Finally, the emergency department is the primary location for the initial evaluation, diagnosis, and treatment of the acutely ill undifferentiated patient. These facts together help define the ethical construct of emergency medical practice where access to quality emergency care is a right of all patients in the US. As noted in the ACEP Code of Ethics, “Emergency physicians shall respond promptly and expertly, without prejudice or partiality, to the need for emergency medical care.”23 The ANA Code of Ethics states that “The emergency nurse works to improve public health and secure access to health care for all.”24 The Society for Academic Emergency Medicine, through its mission statement “to lead the advancement of emergency care through education and research, advocacy, and professional development in academic emergency medicine,”25 also supports the ethical mandate for all patients in the United States to have access to quality emergency medical care regardless of disease process, ability to pay or other characteristics.
While the above ethical framework emphasizes the critical importance of the availability of emergency care to all, it is clear from both published codes of ethics and the literature on the “duty to treat” that there are rare circumstances in which risk to the individual healthcare provider and institution should be weighed in determining the treatment plan for a patient who poses a significant risk to providers or the general public. The ACEP Code of Ethics notes the requirement of the adequacy of in-hospital and outpatient resources in the provision of emergency care.23 The American Medical Association Code of Ethics states that “Because of their commitment to care for the sick and injured, individual physicians have an obligation to provide urgent medical care during disasters. This ethical obligation holds even in the face of greater than usual risks to their own safety, health or life. The physician workforce, however, is not an unlimited resource; therefore, when participating in disaster responses, physicians should balance immediate benefits to individual patients with ability to care for patients in the future.”26 The American Nurses Association Code of Ethics specifically states, “The nurse owes the same duties to self as to others, including the responsibility to preserve integrity and safety.”27 Within the larger ethics literature, explorations of whether there is a duty to treat on the part of healthcare providers at risk to themselves also indicate that codes of ethics, historical references, and theoretical analysis do not mandate an absolute obligation. Rather, particular factors of disease process, availability of resources and training, countervailing responsibilities outside of the professional realm, personal viewpoints on the virtues of courage and resilience as well as relational ethics perspectives and obligations imposed by professional status have guided the evaluations of the obligations of healthcare providers in the face of outbreaks of infectious disease.28, 29, 30 and 31 For emergency departments, emergency physicians and emergency nurses, there is a need to weigh all of these considerations against the special role played by emergency departments in the US healthcare system and the duties that accompany the professional status of emergency physicians and emergency nurses.
Current and Potential Future Ethical Considerations with the Outbreak of EVD
With this background, we will present an ethical framework that has potential application for emergency departments, emergency physicians and emergency nurses along with other health system stakeholders in the particular response to EVD in the United States. This framework will address questions relevant to US emergency departments and separate consideration of the current situation (few confirmed cases within the United States with a relative abundance of resources to respond) versus 2 potential scenarios (increasing number of potential and confirmed domestic cases of EVD in a variety of locations due to spread in the US and widespread number of potential and confirmed domestic cases that would strain existing resources and creates a necessity of disaster triage response) where appropriate.
What are the Ethical Obligations of US Emergency Departments and Hospitals to Support or Encourage the Volunteering of Emergency Physicians and Emergency Nurses to Serve as Healthcare Providers in those Countries Most Affected by the Current Outbreak of EVD?
In the current outbreak of EVD, as of January 1, 2015, there are no extant active cases in the United States. As such, the most immediate issue is how to contain the spread of the disease from its present locus in West Africa and end the current epidemic there. With the underdeveloped nature of the health infrastructure in the primarily affected nations and the declaration of a Public Health Emergency of International Concern by the World Health Organization,32 there is widespread recognition that ending the epidemic does and will continue to require the volunteering of healthcare providers to serve in the outbreak zone.
Under the ethical principle of reciprocity, which calls for acting in a manner that one would want others to act in return, there is an obligation to support emergency physicians and nurses who volunteer to serve in the nations primarily affected by the current Ebola epidemic, just as we would welcome support or available expertise in a time of health crisis in the US. Yet as a practical matter, support of volunteerism needs to be weighed against the special logistical concerns faced by most emergency departments, where local staffing levels must be maintained to provide safe patient care. An application of the principle of reciprocity in this outbreak would include support of emergency physician and nurse volunteerism in the current outbreak through the covering of shifts and other professional obligations in the volunteer’s absence and acceptance by volunteering emergency physicians nurses of any potential risk of contagion on return to the US and the resultant need for monitoring for signs of the disease and possibly prolonged isolation.
We would propose that in considering the support of volunteerism by emergency physicians and nurses, the specific background, training, and education of the provider is a key decision making a factor. Education and training are essential components of preparation prior to disaster or disease outbreak response. Medical volunteers should be appropriately trained in disease management, including rendering effective supportive care within the resource constraints in the primary outbreak zone, prior to travel to infected areas. They should ensure to the extent possible that malpractice, health, and life insurance are in place to cover potential events, likely with the assistance of the Non-Governmental Organization or other agency sponsoring their volunteer efforts. They should be willing to undertake the risks of volunteerism, including infection or threats to individual safety and security.33, 34 and 35 Volunteers should be prepared to ensure appropriate infection control practices in their international work and to follow recommended protocols upon return for monitoring for symptoms of EVD and the isolation that might result.36, 37 and 38 Without this preparation, volunteering emergency physicians and nurses may be a liability rather than a benefit to the resource-poor countries primarily affected by the Ebola outbreak and a risk to the domestic population upon their return to the US.
It is appropriate for emergency departments and hospitals to query volunteering staff on their willingness to undergo the necessary training to be effective in the primary outbreak zone. With the continuing spread of the disease in West Africa, those volunteering emergency physicians and nurses with existing experience in Ebola and disaster response should be given priority over those without such training. Specific decisions regarding support for volunteer efforts should also include the number of volunteers and impact on ED staffing and potential impact on public health domestically (i.e., will the loss of experienced providers adversely affect the care of patients in the local area served by the emergency department?). If the current outbreak were to spread significantly within the US, the ethical evaluation of the appropriateness of supporting volunteerism overseas would likely change since this could result in the expertise on the management of EVD being shifted out of the country rather than being available domestically. This emphasizes the importance of supporting present efforts of containing and ending the current epidemic in West Africa, including with the volunteerism of trained emergency physicians and nurses, as the most effective means of preventing the spread of EVD to the US and other countries.
Some emergency departments have supported the volunteerism of emergency physicians in particular through altruistic coverage of shifts to allow staff to travel to the primary outbreak zone.39 In addition, private foundations have provided grant funding to alleviate the financial burden of volunteerism of emergency department staff in the outbreak zone.40 While these novel approaches have been largely confined to academic settings, they do suggest that there may be methods for individual centers to address the logistical difficulties that can arise when US emergency department providers volunteer in the primary outbreak zone. The application of these options to individual centers is one that is best judged on a case-by-case basis based on the factors noted above.
Finally, emergency departments, emergency medicine, and nursing professional societies, Non-Governmental Organizations and government agencies can aid volunteer efforts by educating health care providers and the lay public using published evidence on the pathophysiology of Ebola and its transmission to alleviate the stigma that returning volunteer staff may experience after their efforts. At the same time, as noted above, volunteering emergency physicians and nurses have an obligation to adhere to monitoring and isolation protocols upon return to the US as a reciprocal ethical obligation for the support their efforts have received.
What are the Ethical Obligations of Emergency Departments and Hospitals to Support other Centers in the Domestic Response to EVD?
As of December 2014, 44 medical centers have been designated by the Centers for Disease Control and Prevention as having the necessary capability and equipment to care for patients diagnosed with EVD.41 It is anticipated that patients with a confirmed EVD diagnosis will be transferred to these hospitals which will have enough PPE and other treatment requirements (isolation rooms, dedicated equipment and designated physicians, nurses and other necessary health care professionals and staff with proper training under CDC guidelines) to manage patients for at least 7 days, after which governmental agencies would assist in acquiring more supplies and expertise if needed.42 However, not every state or locality has such a facility, nor is it likely that an undiagnosed patient would necessarily present to one of these centers. Therefore, the CDC has provided guidelines for so-called frontline (any emergency department or acute care facility) and Ebola assessment hospitals, which can safely isolate, treat and transfer patients with suspected or confirmed EVD. To meet these standards, the CDC has called for all emergency departments to have protocols in place for the recognition of potential Ebola patients and training for the proper isolation and assessment of these individuals.42
The hierarchy of treatment facilities for EVD codifies the reciprocity-based obligations that hospitals have to each other in the current state of the outbreak. Such reciprocity should extend to the sharing of PPE, trained staff and other necessary equipment as needed to care for a suspected or confirmed Ebola patient until the transfer can be effected to a designated treatment center. Hospitals and emergency departments should consider and develop relevant protocols for rapid credentialing of staff and transfer of equipment to allow resources to be brought to bear should there be additional cases in the US. If the current epidemic were to spread significantly in the US, hospitals should consider whether and how they can upgrade their capabilities to meet the needs of rising numbers of patients, presumably with the assistance of government resources.
Another ethical consideration is the reputational impact upon hospitals caring for Ebola patients. As has been reported in the press, hospitals have expressed concern that the potential costs and risks accrued in treating an Ebola patient along with the public fear generated by the disease may have an adverse impact on volumes and financial results for medical centers. The facility in Dallas that treated a recent case reported that afterward emergency department volumes dropped and still have not returned to their expected level.19 It is therefore imperative, in the face of a disease such as Ebola that has generated such public scrutiny and at times hysteria, for hospitals to be cognizant of their ethical responsibility to support the efforts of designated treatment centers as well as frontline facilities that might encounter Ebola patients and potentially be perceived adversely by the public. We affirm that the principle of reciprocity extends beyond physical means of support (equipment, personnel) to reputational support in the setting of an outbreak of EVD. Such support could, where appropriate, take the form of publicly confirming the safety and quality of other healthcare facilities with Ebola patients, educating other facilities on effective policies and procedures in caring for EVD patients and avoiding messages that implicitly suggest a competitive advantage from not treating patients with this highly infectious disease. Through such support, hospitals ensure that the public is aware and reassured of the unified response the medical system will take towards both the existing epidemic and the potential for worsening if the outbreak spreads from West Africa. Without such reputational support and cohesion in the healthcare system, should the epidemic worsen, it is conceivable that public doubt and panic may lead to untenable consequences such as facilities avoiding the care of at-risk patients and the public fearing certain hospitals as being sites of contagion rather than medical care?
Should Trainees be Allowed to Participate in the Care of Suspected or Confirmed EVD Patients?
Trainees (nursing students, medical students, residents, and fellows) routinely care for patients with infectious diseases in the ED and should understand and use proper measures to protect themselves while caring for patients with potential or confirmed contagious diseases. Both the Accreditation for Graduate Medical Education program requirements in emergency medicine and guidance on Ebola affirm that trainees should know how to recognize, treat and isolate patients with infectious disease in general and Ebola specifically.43 and 44 The 2013 Model of the Clinical Practice of Emergency Medicine goes further by listing within the domain of emergency medicine “understand[ing and apply[ing] the principles of disaster and mass casualty management including preparedness, triage, mitigation, response, and recovery.”45 Additional content areas in the Model relevant to Ebola response include the following: personal protection (equipment and techniques); universal precautions and exposure management; and emerging infections, pandemics and drug resistance.45 Together, these raise the issue of whether the current EVD outbreak should be viewed as an opportunity for trainees in emergency medicine and emergency nursing to care for patients during an international infectious disease epidemic. Few health care professionals in the United States have experience with the diagnosis and treatment of Ebola or the infection control precautions required to safely care for patients with this disease. Yet some such individuals may include trainees either with specific backgrounds in infectious diseases or previous experience with the PPE utilized in caring for such patients.
Historically, the outbreak of an unknown or uncommon infectious disease has led to initial concerns by health providers about the risk to self that ultimately gives way with time and knowledge to acceptance of an affirmative duty for trainees to learn to treat patients with these conditions. For example, the early fear and stigma surrounding HIV-infected patients in the 1980s gave way to a widely recognized duty to treat these patients and instill the same ethic in trainees.46 As knowledge of the pathophysiology and epidemiology of EVD and its implications for healthcare providers become more widely disseminated, a similar evolution may take place. However, based on the current conditions of the Ebola outbreak, it is likely that very few of these professionals will need to be called upon to fulfill this duty.
As long as the Ebola incidence in the United States remains low, each institution can and should manage its burden of suspected Ebola cases with a cadre of nurses and physicians highly trained in Ebola treatment and prioritize infection control. The ethical justification to restrict the number of caregivers who come in contact with Ebola-infected patients is that, given the limited experience with the disease in the United States, unnecessary exposure to infected patients would increase the risk to providers, other patients, and the public. It is prudent to limit the potential chain of infection when possible.
Because experienced or specially-trained nurses and attending physicians can effectively manage suspected or confirmed Ebola cases, trainee involvement is not required and would entail unnecessary risks to trainees and their patients. Trainees should, however, be fully prepared in case they find themselves in a position where their duty to treat an individual patient outweighs a duty to the public to limit exposure to the disease.44 However, if not trained or equipped properly, their duty to reasonably protect their own safety should not be superseded.
Non-participation of trainees in the care of Ebola-infected patients is then an instance of exclusion, rather than exemption. Institutions exclude trainees as an infection control strategy; trainees do not opt out. Some trainees may object to these policies, as they may feel ethically compelled to care for Ebola-infected patients as a function of their professional role and view their exclusion as a restriction of their own moral agency and liberty (to fulfill their commitment to treating the sick).39 However, this restriction is justified by the greater good of protecting public health. Ensuring trainee well-being and availability to care for other ED patients as well as limiting contagion are ethically justifiable reasons to exclude trainees. Exclusion of trainees from the care of Ebola-infected patients is not simply paternalistic because the primary aim is to protect patients and the public and represents a proportional response relative to the professionalism and moral agency consideration of trainees.47
At the same time, a blanket exclusion of trainees from the care of Ebola patients in the primary outbreak zone may be ethically inappropriate. If the trainee has the relevant experience and is able to meet the other requirements outlined above for volunteerism in the countries most affected by Ebola currently, a case-by-case evaluation would seem appropriate for supporting the participation of volunteering trainees in the international response where there is a desperate need for available healthcare providers.39 Such support would have the added benefit of growing the cadre of individuals with the relevant expertise in caring for patients with EVD should the current outbreak spread to the US. However, it is worthy of consideration whether academic medical centers can appropriately manage the risk to their trainees in the conditions posed by the outbreak in West Africa. There are additional reputational risks should a trainee contract Ebola or the public adversely view institutions where a large cadre of providers, including trainees, have traveled to care for patients in the primarily affected countries.39
As such, we affirm the ethical appropriateness of academic medical centers to consider on an individual provider basis whether a trainee should be supported in volunteering to travel to Africa rather than endorsing a policy of automatic exclusion or support of providers in this regard. Such individualized evaluations should take specific account of the level of training, previous background, experience with Ebola and the PPE required to care for patients with this disease, the ability to undergo the necessary preparation for functioning effectively in the primary outbreak zone and the willingness to comply with monitoring and isolation protocols upon return to the US.
Is it Ethically Appropriate for Emergency Physicians or Emergency Nurses to Opt Out of the Care of Patients With EVD?
Under the current state of the Ebola outbreak, it is anticipated that cases in the US would be scattered and readily managed at designated treatment centers.41 At the same time, it is recognized that suspected patients may present to frontline emergency departments without specialized expertise in the management of EVD,42 and, as seen in the case of the patient in Dallas, this may pose a risk to health care providers, including emergency physicians and emergency nurses.3 As a result, various health care providers have expressed reluctance to care for patients with Ebola.48, 49, 50 and 51 Historically, such provider reluctance has often arisen with the emergence of unknown infectious diseases.29 A 2008 survey of thousands of healthcare workers in New York found that half would hesitate or refuse to report to work during a Severe Acute Respiratory Syndrome (SARS) outbreak (though 84% would report to work during a mass casualty situation). Most cited concern for family, followed by concern for self, as reasons not to report to work during a SARS epidemic. 52 Individual conscience then, rather than professional tradition, seems to be the main force that compels nurses and physicians to risk their lives in the service of patients. 29 and 46
With this background, it is fair to ask whether there are circumstances under which emergency department providers could opt out of the care of Ebola patients. Under US law, nurses and physicians have a legal duty to treat patients with whom they have entered into a therapeutic relationship. Once undertaken, the duty continues until the patient and professional mutually agree to end the relationship or the care is transferred to another professional.53 Nurses and physicians have special duties in service of the sick, and since this obligation holds even in face of greater than usual risks to one’s own safety, healthcare professionals consequently accept greater risks than ordinary, balancing immediate benefits to individual patients with the professional’s own health and ability to treat future patients.54 But there is no consensus on the specific limits of this duty.30 and 55
Emergency nurses and physicians are the front line in an outbreak and, implicit in their specialty choice, accept additional risk beyond what is typical for many of their colleagues. As noted above, this is acknowledged in professional codes of ethics and statutory mandates (e.g., EMTALA).21, 22, 23, 24 and 26 There are potential additional penalties for those health care professionals who refuse to work or treat patients during a pandemic, including reduction in pay, termination and, in some states that have adopted variations of the Model State Emergency Health Powers Act (MHEHPA), the possibilities of licensure actions, fines or imprisonment.56 and 57
Though the legal foundations of the duty to treat and its consequences are significant, the most compelling ground for these obligations is that health care is a moral enterprise.29 and 58 “All its efforts converge ultimately on decisions and actions which are presumed to be good for some person in need of help and healing.”58 Nurses and physicians have a professional commitment to healing the sick. They are morally accountable to this commitment and are expected to demonstrate the virtues that it entails—such as courage, compassion and fidelity.29 and 59 This virtue-based ethics is independent of the patient’s right to access to healthcare and the contract between the patient and physician. Rights-based and contract-based accounts of the duty to treat would allow nurses and physicians to opt out of caring for patients in an epidemic as long as others were willing to take their place.28 But nurses and physicians who opt out in such cases still fall short of their moral commitment.29
Emergency nurses and physicians, therefore, have a duty to care for Ebola-infected patients and, in most instances, accept the associated risks.30 and 60 But the duty is not unlimited. An “abstract limitless duty” obscures the discussion about reasonable risk acceptance among nurses and physicians.60 Allowing for reasonable and practical limits to the duty to treat—applied equitably to all clinicians—may increase the likelihood that nurses and physicians will live up to their individual obligations during an outbreak.30
The limit is illustrated by an account of a physician who, during the 1995 Ebola outbreak in the Democratic Republic of the Congo, “found 30 dying patients in an abandoned hospital, left to care for themselves amid rotting corpses, sometimes in the same bed.”30 A nurse or physician should not be expected to treat patients in a context where the risks are extraordinarily high and the potential benefit to patients extremely low.30 Indeed, the first duty of emergency nurses and physicians in the current Ebola outbreak or other emerging infectious disease is to protect themselves in the care of patients, if for no other reason than to ensure their availability to treat subsequent patients.61 By contrast, care of Ebola-infected patients in a US hospital with the proper PPE and training would fall well within the duty to treat.15
In the current state of the Ebola outbreak, establishing cadres of highly trained clinicians at well-resourced institutions may be the best way to deliver uniform care under a duty to treat and limit potential spread of infection in the US.42 Under the above-noted virtue and professionalism-based ethical framework,23, 24, 26, 58 and 59 emergency nurses and physicians may also volunteer in place of colleagues who they see experiencing exceptional moral or emotional distress over caring for Ebola-infected patients—for example, as a result of unusually severe consequences for loved ones should they become ill. But as the burden of Ebola-infected patients rises, the duty to treat is a responsibility of all emergency nurses and physicians who have the necessary training, skills, and experience.
While the duty to treat is intrinsic to health care professionals, institutions may also hold emergency nurses and physicians accountable to this standard. However, institutions may not invoke the duty to treat to coerce hospital employees into accepting unnecessarily dangerous conditions: for example, to expect them to deliver care to Ebola-infected patients without proper PPE or training. Institutional leaders have an ethical responsibility to prepare for outbreaks, ensure that the providers who risk their lives in the service of patients do so with as much protection and support as possible and make available appropriate channels for emergency physicians and nurses to communicate concerns about the adequacy of the training and preparation they receive. Preparation includes, but is not limited to, making high-quality PPE readily available, ensuring that all relevant staff is educated and trained to use it properly (especially proper donning and doffing) and limiting exposure to only those individuals needed to care for patients and prevent the spread of infection.
Experience with the 2003 SARS epidemic in Canada suggests that hospital leaders owe even more than merely providing equipment and training to nurses and physicians who fulfill their duty to treat under hazardous conditions. Some healthcare workers died from SARS, and some spread the disease to their families.55 Healthcare workers have moral obligations to their families, and institutions should make it possible for them to care for patients without abandoning their responsibility to their families or risking their families’ lives. Institutions should, for example, assist with childcare and provide temporary living quarters to reduce the risk of disease transmission to family members and the associated anxiety and moral distress.62 Institutions, as well as public health agencies, may also consider additional acts of reciprocity toward healthcare workers who fulfill their duty to treat, such as insurance to protect them and their families should they become ill or die as a result of caring for Ebola-infected patients. Ultimately, however, emergency nurses and physicians care for the sick primarily out of personal moral obligation; financial incentives alone are not likely to increase the likelihood that they will discharge their duty under epidemic conditions.63
The protections that institutions and society provide healthcare workers—for themselves and their families—are ethically required. Just as emergency nurses and physicians may not generally opt out of caring for the sick, institutions and communities may not opt out of caring for healthcare professionals and their families. In sum, the duty to treat patients with infectious diseases, including Ebola, is both a legal responsibility and an ethical obligation of the healthcare professions. The duty should be borne equitably by professionals, who in turn, should be adequately supported by institutions and society as a whole.
Given the expected low number of US cases, there is a role for institutions to ask healthcare providers to volunteer to serve on treatment teams for suspected Ebola patients as a means of limiting training efforts, time and expenditures (eg, credentialing of the ability to perform invasive procedures with PPE), reducing the potential risk of infection and ensuring relevant personnel and expertise are available to provide care. However, such volunteer-based plans do not address the special role of emergency departments where patients may present in an undifferentiated manner and potentially in acute distress, and where alternative providers may simply not be available. For emergency physicians and nurses, who through their choice of profession knowingly accept the above circumstances of patient care,23 and 24 the current state of the Ebola outbreak does not justify opting out of the care of suspected or confirmed Ebola patients who may present to the emergency department, but this obligation is contingent upon institutional and governmental resources that provide adequate training and equipment to fulfill this duty. There also needs to be a recognition by healthcare personnel, hospitals and other public health and legal authorities as well as patients that the duty of emergency physicians and nurses to treat must be absolutely contingent on first ensuring personal safety through the proper use of PPE.61 and 64 Should Ebola rise in prevalence in the US, contingency planning to meet the duty to treat should move beyond training and equipment to mechanisms to support the weighty obligations of emergency physicians and nurses to protect themselves and their families while caring for affected patients.
Are the Goals of Care Different in Patients Critically Ill with EVD?
With the high mortality rate, lack of specific treatment and need for specialized PPE in order to prevent transmission, there have been legitimate questions whether the goals of care should change in patients critically ill with EVD. Specifically, in the circumstance where a patient requires procedural interventions (central venous access, intubation, dialysis, etc) to provide intensive care level support, is the risk posed to providers too high compared to the low potential of benefit, if any, to a patient whose illness may have progressed to a point where such interventions are unlikely to be successful? Furthermore, given the time needed to don PPE—an absolute requirement prior to any procedural intervention on an EVD patient—should cardiopulmonary resuscitation during an arrest event be considered futile due to the potential delay in its initiation and again the likely prognosis of the patient?11, 64 and 65
Since the initial posing of these concerns about the risk versus benefit posed by critical care and resuscitation interventions in patients with EVD, case reports have appeared showing that aggressive, intensive care level interventions, including intubation, central venous access, large volume and blood resuscitation and dialysis, can be successful in treating critically ill individuals with this disease and do not pose an automatic risk to providers if PPE is properly used.66 and 67 While anecdotal and representative more of what is possible in idealized circumstances (specialized care units with previous expertise and training in care of EVD patients and a high number of dedicated providers), these cases imply that utilizing the full panoply of critical care resources for this patient population may be appropriate treatment. However, the highly contagious nature of EVD and the need for specialized PPE, along with the experience in Africa of rapid transmission to family members caring for ill patients, makes it appropriate for hospitals to not allow family presence during such procedures as is allowed in other critical care or resuscitation circumstances.
With respect to cardiopulmonary resuscitation, to our knowledge, no published report has indicated the successful or unsuccessful use of cardiopulmonary resuscitation in an arrest event in an Ebola patient, through resuscitation success in a US healthcare facility may be similar to other infectious diseases at similar stages, from initial manifestations to overwhelming sepsis. At this time, consideration of do-not-resuscitate status in a late-stage EVD patient is best determined on a case-by-case basis, taking into account potential benefit to the patient, any limitations of interventions imposed by the disease and the potential risks to the treatment team.
However, the circumstances described for the above patients are not typical of that seen in most emergency departments in the US. While the current state of the outbreak would likely lead to a typical ED encountering a patient early in their EVD process, if at all, and being able to isolate such an individual until transfer to a higher level of care, should the number of cases rise due to spread of the disease, it is conceivable that emergency departments could encounter patients in a variety of stages of Ebola with the risk-benefit calculation on procedural interventions being highly relevant. Unlike the above cases, should the current outbreak spread, emergency departments would encounter patients with fewer resources (fewer isolation facilities, lower ratios of providers to the patient) than those expended in the above-reported cases and having to simultaneously care for other patients with a variety of conditions. Here there is a need to refer to the special role played by emergency physicians and nurses in the healthcare system. The assumptions that accompany the choice of these professional roles (exposure to acutely ill, undifferentiated patients) and the specialized training and skills that emergency physicians and nurses possess impose a higher obligation than other medical professionals to be prepared to treat an acutely ill Ebola patient in the emergency department setting.23 and 24
At the same time, as we noted above, the duty to treat is not absolute. There is no obligation for an emergency physician or nurse to implement treatment measures in an acutely ill Ebola patient without training in the use of PPE, the availability of such supplies and, at a minimum, simulated experience with performing critical care procedures while utilizing PPE.15, 28 and 61 Without such minimum standards, the social contract that accompanies the professional standing and obligations of emergency physicians and nurses breaks down. This social contract calls for a rational person to expect an emergency physician or nurse to apply their skills to aid an acutely ill patient but at the same time for those professionals to have the requisite training and equipment to provide such aid in an appropriate manner.68
All emergency departments and hospitals should, therefore, consider that protocols for PPE training and isolating suspect patients, as called for in the current interim CDC guidelines,42 are likely inadequate should the current epidemic spread more prominently to the US. To fulfill the ethical obligations imposed by the duty to treat should the current outbreak become more prevalent domestically, more robust training with PPE and the performance of procedures with such equipment will be necessary for a wider cadre of emergency physicians and nurses to appropriately treat acutely ill Ebola patients in intermediate or late stages of the disease while ensuring the maximum feasible protection of the healthcare provider. Weighing when such expanded training may be warranted should take into account the continued status of the outbreak, the cost of such preparation and the availability of appropriate resources to be effective.
In the unexpected scenario where the number of patients with EVD overwhelms existing resources, more traditional disaster triage protocols would be applicable. Such protocols attempt to apply resources in a manner to benefit the largest number of patients. In the case of Ebola, where the evidence to date is that an overwhelming amount of critical care resources are required to effectively treat a late-stage patient, disaster triage protocols would need to weigh at what point in the treatment spectrum such resource expenditure would become untenable. Such protocols, to be ethically appropriate, would need to be transparent, proportionate and accountable to oversight along with having a legal imprimatur to be effective in the emergency department and acute care setting.69 To avoid such a crisis situation, the devotion of resources now to end the epidemic in the primary outbreak zone in Africa is vital.
Ebola Virus Disease Patients Should not Receive CPR Future Considerations
The outbreak of EVD in West Africa has presented a significant challenge to the health systems of the primarily affected nations and, even with a low case count, raised concerns about the preparedness of the US healthcare system to respond to uncommon infectious diseases. In some ways, Ebola is a unique test for US emergency departments, emergency physicians, emergency nurses and other stakeholders are given its rarity in the US, high mortality rate, high risk of transmission to healthcare staff and non-specific presenting symptoms that can make initial diagnosis more difficult. However, as shown with other unanticipated infectious disease outbreaks (HIV, SARS, MERS), emergency departments will almost certainly be a key location for patient identification and treatment. The ethical concepts applied in this paper are relevant, especially reciprocity, duty to treat and grounding in the specific facts of the disease process in question when considering how acute care facilities should prepare for likely future outbreaks of infectious disease. We propose that preparation for future emergency department responses to unanticipated infectious disease outbreaks should include ethical as well as logistical and medical factors.69 Given the multiple stakeholders represented in emergency department practice, the model shown here of multi-disciplinary and organizational consideration of the ethical issues involved would likely have application when considering the approach to future infectious disease challenges.
Ebola Virus Disease Patients Should not Receive CPR Conclusion
The outbreak of EVD in West Africa and the presentation of patients to US acute care facilities have raised a series of intertwined logistical and ethical issues of relevance to US emergency departments, emergency physicians and emergency nurses. While the current state of the epidemic has not led to a large number of EVD patients presenting to US facilities, consideration of ethical questions that are relevant now and of potential relevance in the future will allow emergency physicians, emergency nurses and other stakeholders to prepare appropriately for the challenges posed by Ebola and consider its implications for future epidemic infectious disease events. An emphasis on the principle of reciprocity, the obligations imposed by and underlying assumptions of the duty to treat and the specific characteristics of the disease process will aid in addressing the ethical challenges posed in the current outbreak of EVD.
Acknowledgments
The drafting authors wish to thank the ACEP Ebola Expert Panel and SAEM Global Academy of Emergency Medicine for their critical review of the manuscript during preparation and the leadership of ACEP, ENA, and SAEM for their sponsorship of this effort.
References
1
Centers for Disease Control and Prevention
Ebola outbreak in West Africa—case counts
http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html (2014) Updated February 4, 2015. Accessed February 5, 2015
2
R Dunklin, S Thompson
ER doctor discusses the role in Ebola patient’s initial misdiagnosis
Dallas Morning News (2014) http://www.dallasnews.com/ebola/headlines/20141206-er-doctor-discusses-role-in-ebola-patients-initial-misdiagnosis.ece, Accessed February 5, 2015
3
G Botelho, J Hanna, A Fantz
Nurse’s discharge leaves one Ebola case in the U.S., though larger battle continues. CNN Web site
http://www.cnn.com/2014/10/28/health/us-ebola/ Accessed February 5, 2015
4
A Hartocollis, M Santora
Plenty of hugs as Craig Spencer, recovered New York Ebola patient, goes home
N Y Times (2014) http://www.nytimes.com/2014/11/12/nyregion/craig-spencer-new-york-ebola-patient-bellevue.html?_r=0, Accessed February 5, 2015
5
C Moskowitz
Are U.S. Hospitals Prepared for the Next Ebola Case?
Sci Am (2014) Available from http://www.scientificamerican.com/article/are-us-hospitals-prepared-for-the-next-ebola-case/, Accessed February 5, 2015
6
A Soergel
Ebola quarantine questioned
US News and World Report (2014) http://www.usnews.com/news/newsgram/articles/2014/10/27/ebola-ethics-quarantine-questioned, Accessed February 5, 2015
7
American College of Emergency Physicians
Healthcare resources for suspected Ebola cases
http://www.acep.org/ebola/ Published 2014, Accessed February 5, 2015
8
Emergency Nurses Association
ENA topic brief: Ebola virus disease
http://www.ena.org/practice-research/Practice/Documents/EbolaTopicBrief.pdf Accessed February 5, 2015
9
Centers for Disease Control and Prevention
Ebola (Ebola virus disease)
http://www.cdc.gov/vhf/ebola/ Updated February 4, 2015, Accessed February 5, 2015
10
R Perl
Ebola response reveals a double standard in U.S. health care
Forbes (2014) http://www.forbes.com/sites/robertpearl/2014/12/11/ebola-double-standard/, Accessed February 5, 2015
11
L Altman
Ethicist calls CPR too risky in Ebola
N Y Times (2014) http://www.nytimes.com/2014/10/21/health/-ethicist-calls-cpr-too-risky-in-ebola-.html, Accessed February 5, 2015
12
N Kass
Ebola, ethics, and public health: what next?
Ann Intern Med, 161 (10) (2014), pp. 744–745
Full Text via CrossRef | View Record in Scopus | Citing articles (13)
13
Toner E, Adalja A, Inglesby T. A primer on Ebola for clinicians published online ahead of print October 17, 2014. Disaster Med Public Health Prep.
14
G Donovan
Ebola, epidemics, and ethics—what we have learned
Philos Ethics Humanit Med, 9 (2014), p. 15
Full Text via CrossRef
15
K Koenig, C Majestic, M Burns
Ebola virus disease: essential public health principles for clinicians
West J Emerg Med, 15 (7) (2014), pp. 728–731
Full Text via CrossRef | View Record in Scopus | Citing articles (9)
16
L Meyers, T Frawley, S Goss, et al.
Ebola virus outbreak 2014: a clinical review for emergency physicians
Ann Emerg Med, 65 (1) (2015), pp. 101–108
Article | PDF (1103 K)
| View Record in Scopus | Citing articles (14)
17
H Feldmann, T Geisbert
Ebola hemorrhagic fever
Lancet, 377 (9768) (2011), pp. 849–862
Article | PDF (2175 K)
| View Record in Scopus | Citing articles (429)
18
Centers for Disease Control and Prevention
Review of human-to-human transmission of Ebola virus
http://www.cdc.gov/vhf/ebola/transmission/human-transmission.html Updated October 29, 2014, Accessed February 5, 2015
19
L Sun, B Dennis
U.S. hospitals wary of caring for Ebola patients because of cost and stigma
The Washington Post (2014) http://www.washingtonpost.com/national/health-science/us-hospitals-wary-of-caring-for-ebola-patients-because-of-cost-and-stigma/2014/11/28/928aa2bc-71cc-11e4-893f-86bd390a3340_story.html, Accessed February 5, 2015
20
J Pines, R Mutter, M Zocchi
Variation in emergency department admission rates across the United States
Med Care Res Rev, 70 (2013), pp. 218–231
Full Text via CrossRef | View Record in Scopus | Citing articles (35)
21
Emergency Treatment and Active Labor Act (EMTALA), 42 USC §1395dd
(2008)
22
Center for Clinical Standards and Quality/Survey and Certification Group
Center for Medicare and Medicaid Services. Emergency Medical Treatment and Labor Act (EMTALA) requirements and implications related to Ebola virus disease (Ebola)
http://www.aha.org/content/14/141121-sc15-10emtala-ebola.pdf Published November 21, 2014. Accessed February 5, 2015
23
American College of Emergency Physicians
Code of ethics for emergency physicians
http://www.acep.org/Clinical—Practice-Management/Code-of-Ethics-for-Emergency-Physicians/ Accessed February 5, 2015
24
Emergency Nurses Association
ENA code of ethics
http://www.ena.org/about/ethics/Pages/Default.aspx Accessed February 5, 2015
25
Society for Academic Emergency Medicine
SAEM mission statement
http://www.saem.org/about-saem/mission Accessed February 5, 2015
26
American Medical Association
Opinion 9.067—Physician obligation in disaster preparedness and response
http://www.ama-assn.org.vlib.excelsior.edu/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion9067.page Accessed February 5, 2015
27
American Nurses Association
Code of ethics for nurses
http://www.nursingworld.org/codeofethics Accessed February 5, 2015
28
H Malm, T May, L Francis, et al.
Ethics, pandemics, and the duty to treat
Am J Bioeth, 8 (8) (2008), pp. 4–19
Full Text via CrossRef | View Record in Scopus | Citing articles (44)
29
A Zuger, S Miles
Physicians, AIDS, and occupational risk: historic traditions and ethical obligations
JAMA, 258 (14) (1987), pp. 1924–1928
Full Text via CrossRef | View Record in Scopus | Citing articles (110)
30
D Sokol
Virulent epidemics and scope of healthcare workers’ duty of care
Emerg Infect Dis, 12 (8) (2006), pp. 1238–1241
Full Text via CrossRef | View Record in Scopus | Citing articles (52)
31
W Austin
Ethics in a time of contagion: a relational perspective
Can J Nurs Res, 40 (4) (2008), pp. 10–24
View Record in Scopus | Citing articles (7)
32
World Health Organization
Statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa
http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/ Published August 8, 2014, Accessed February 5, 2015
33
Wildes R, Kayden S, Goralnick E, et al. Sign me up: rules of the road for humanitarian volunteers during the Ebola outbreak published online ahead of print October 24, 2014. Disaster Med Public Health Prep.
34
E Weiner
The nursing curriculum for emergency preparedness
http://www.nursing.vanderbilt.edu/advantage/emergency.html Accessed February 5, 2015
35
George Washington University School of Nursing
The National Nurse Emergency Preparedness Initiative (NNEPI)
http://nnepi.gwnursing.org/ Accessed February 5, 2015
36
Centers for Disease Control and Prevention
For general healthcare settings in West Africa: four keys to infection control
http://www.cdc.gov/vhf/ebola/hcp/international/keys-to-infection-control.html Updated December 19, 2014, Accessed February 5, 2015
37
M McCarthy
CDC rejects mandatory quarantine for travelers arriving from Ebola-stricken nations
BMJ, 349 (2014), p. g6499
Full Text via CrossRef | View Record in Scopus | Citing articles (3)
38
ACEP Ebola Expert Panel
Consensus statement on restrictive movement including quarantine of health care workers
http://www.acep.org/uploadedFiles/ACEP/practiceResources/issuesByCategory/publichealth/ACEP%20Ebola%20Expert%20Panel%20Consensus%20Statement.111314.pdf Published November 13, 2014, Accessed February 5, 2015
39
L Rosenbaum
License to Serve — U.S. Trainees and the Ebola Epidemic
New England Journal of Medicine, 372 (6) (2015), pp. 504–506
Full Text via CrossRef | View Record in Scopus | Citing articles (7)
40
Academic Consortium Combating Ebola in Liberia. http://accel.mit.edu/. Accessed December 30, 2014.
41
Centers for Disease Control and Prevention
Current Ebola Treatment Centers
http://www.cdc.gov/vhf/ebola/hcp/current-treatment-centers.html Accessed December 22, 2014
42
Centers for Disease Control and Prevention
Interim guidance for U.S. hospital preparedness for patients under investigation (PUIs) or with confirmed Ebola virus disease (EVD): a framework for a tiered approach
http://www.cdc.gov/vhf/ebola/hcp/us-hospital-preparedness.html Updated January 22, 2015, Accessed February 5, 2015
43
Accreditation Council for Graduate Medical Education
ACGME program requirements for graduate medical education in emergency medicine
https://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQ-PIF/110_emergency_medicine_07012013.pdf Published July 1, 2013, Accessed February 5, 2015
44
Accreditation Council for Graduate Medical Education
ACGME guidance statement on Ebola virus infection and resident/fellow training in the United States
https://www.acgme.org/acgmeweb/Portals/0/PDFs/Nasca-Community/ACGME-GME-Ebola-Final1.pdf Published October 2014, Accessed February 5, 2015
45
FL Counselman, MA Borenstein, CD Chisholm, et al.
The 2013 model of the clinical practice of emergency medicine
Acad Emerg Med, 21 (5) (2014), pp. 574–598
Full Text via CrossRef | View Record in Scopus | Citing articles (17)
46
R Bayer, GM Oppenheimer
AIDS Doctors: Voices From the Epidemic: An Oral History
Oxford University Press, Oxford, UK (2002)
47
JF Childress, RR Faden, RD Gaare, et al.
Public health ethics: mapping the terrain
J Law Med Ethics, 30 (2) (2002), pp. 170–178
Full Text via CrossRef | View Record in Scopus | Citing articles (257)
48
BBC News
Ebola: When health workers’ duty to treat is trumped
http://www.bbc.com/news/health-29573993 Published October 29, 2014, Accessed February 5, 2015
49
L Gruson
Montana nurses concerned about Ebola
Great Falls Tribune (2014) http://www.greatfallstribune.com/story/news/local/2014/10/15/montana-nurses-concerned-ebola/17340921/, Accessed February 5, 2015
50
J Schram, L Celona
Bellevue staffers call in “sick” after Ebola arrives
New York Post (2014) http://nypost.com/2014/10/25/many-bellevue-staffers-take-sick-day-in-ebola-panic/, Accessed February 5, 2015
51
Fox News
Hospital staffers reportedly take sick day rather than treat New York’s first Ebola patient
http://www.foxnews.com/health/2014/10/25/hospital-staffers-reportedly-take-sick-day-rather-than-treat-new-yorks-first/ Published October 25, 2014, Accessed February 5, 2015
52
K Qureshi
Health care workers’ ability and willingness to report to duty during catastrophic disasters
J Urban Health, 82 (3) (2005), pp. 378–388
Full Text via CrossRef | View Record in Scopus | Citing articles (184)
53
Payton v. Weaver, 131 Cal App 3d 38, 182 Cal Rptr 225 (Cal App 1 Dist 1982).
54
K Morin, D Higginson, M Goldrich
for the Council on Ethical and Judicial Affairs of the American Medical Association. Physician obligation in disaster preparedness and response
Camb Q Healthc Ethics, 15 (2006), pp. 417–421
View Record in Scopus | Citing articles (8)
55
P Singer, S Benatar, M Bernstein, et al.
Ethics and SARS: lessons from Toronto
BMJ, 327 (7427) (2003), p. 1342
Full Text via CrossRef | View Record in Scopus | Citing articles (90)
56
Center for Law and the Public’s Health
Model State Emergency Health Powers Act
http://www.publichealthlaw.net/MSEHPA/MSEHPA.pdf Accessed February 5, 2015
57
C Coleman, A Reis
Potential penalties for health care professionals who refuse to work during a pandemic
JAMA, 299 (2008), pp. 1471–1473
Full Text via CrossRef | View Record in Scopus | Citing articles (15)
58
E Pellegrino
Ethics and the moral center of the medical enterprise
Bull N Y Acad Med, 54 (7) (1978), p. 625
View Record in Scopus | Citing articles (3)
59
E Pellegrino
Toward a virtue-based normative ethics for the health professions
Kennedy Inst Ethics J, 5 (3) (1995), pp. 253–277
Full Text via CrossRef | View Record in Scopus | Citing articles (99)
60
M Meerschaert
Physicians’ duty to participate in pandemic care
JAMA, 300 (3) (2008), p. 284
Full Text via CrossRef | View Record in Scopus | Citing articles (2)
61
Koenig K. Ebola triage screening and public health: the new “vital sign zero” published online ahead of print October 29, 2014. Disaster Med Public Health Prep.
62
L Hawryluck, S Lapinsky, T Stewart
Clinical review: SARS–lessons in disaster management
Crit Care, 9 (4) (2005), p. 384
Full Text via CrossRef | View Record in Scopus | Citing articles (28)
63
C Irvin, L Cindrich, W Patterson, et al.
Survey of hospital healthcare personnel response during a potential avian influenza pandemic: will they come to work?
Prehosp Disaster Med, 23 (2008), pp. 328–335
Full Text via CrossRef | View Record in Scopus | Citing articles (56)
64
American Society of Anesthesiology
Recommendations from the ASA Ebola Workgroup
http://www.asahq.org/For-Members/Clinical-Information/Ebola-Information/Ebola-Guidelines-from-COH.aspx Accessed February 5, 2015
65
J Fins
Responding to Ebola: questions about resuscitation
http://www.thehastingscenter.org/Bioethicsforum/Post.aspx?id=7135&blogid=140 Published October 10, 2014, Accessed February 5, 2015
66
B Kreuels, D Wichmann, P Emmerich, et al.
A case of severe Ebola virus infection complicated by gram-negative septicemia
N Engl J Med, 37 (2014), pp. 2394–2401
Full Text via CrossRef | View Record in Scopus | Citing articles (106)
67
G Lyon, A Mehta, J Varkey, et al.
Clinical care of two patients with Ebola virus disease in the United States
N Engl J Med, 371 (2014), pp. 2402–2409
Full Text via CrossRef | View Record in Scopus | Citing articles (109)
68
J Rachels, S Rachels
The Idea of a Social Contract: The Elements of Moral Philosophy
(6th ed.)McGraw-Hill, Boston, MA (2010)
69
Institute of Medicine
Crisis Standards of Care: A Systems Framework for Catastrophic Disaster Response
National Academies of Science, Washington, DC (2012)
For correspondence, write Arvind Venkat, MD, FACEP, Department of Emergency Medicine, Allegheny Health Network, 320 East North Avenue, Pittsburgh, PA 15212.
Vitae
Arvind Venkat (ACEP, SAEM), Department of Emergency Medicine, Allegheny Health Network, Pittsburgh, PA.
Lisa Wolf (ENA), Institute of Emergency Nursing Research, Des Plaines, IL.
Joel M. Geiderman (ACEP), Department of Emergency Medicine, Cedars-Sinai Medical Center, Los Angeles, CA.
Shellie L. Asher (SAEM), Department of Emergency Medicine, Albany Medical Center, Albany, NY.
Catherine A. Marco (ACEP), Department of Emergency Medicine, Boonshoft School of Medicine, Wright State University, Dayton, OH.
Jolion McGreevy (SAEM), Department of Emergency Medicine, Boston Medical Center, Boston University School of Medicine, Boston, MA.
Arthur R. Derse (ACEP), Center for Bioethics and Medical Humanities (Institute for Health and Society) and Department of Emergency Medicine, Medical College of Wisconsin, Milwaukee, WI.
Edward J. Otten (SAEM), Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH.
John E. Jesus (ACEP), Department of Emergency Medicine, Christiana Care Health System, Wilmington, DE.
Natalie P. Kreitzer (SAEM), Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH.
Monica Escalante (ENA), Institute for Quality, Safety and Injury Prevention, Des Plaines, IL.
Adam C. Levine (SAEM), Department of Emergency Medicine, Warren Alpert Medical School of Brown University, Providence, RI.
ED Ebola Triage Algorithm: A Tool and Process for Compliance
2015, Journal of Emergency Nursing
more
Nursing and complex humanitarian emergencies: Ebola is more than a disease
2015, Nursing Outlook
more
Arterial Blood Gas Review
2015, Journal of Emergency Nursing
more
View more articles »
Related book content
For this week you should:
1. Use the assigned readings, web and professional resources, and the M1A1 interactive tutorial to compose an initial discussion post M1D1, complete with in-text citations and references of a minimum of 250 words to post be Carefully look at the AD Discussion Rubric prior to composing your post and make sure you answer every component of the discussion question.
2. Develop and post two (2) responses to the initial posts of two (2) different peers who have chosen a different idea than your initial post. Be sure to use the module content and reference it to support your post. The responses must be a minimum of 100 words for each post no later than 11:59 PM on Sunday, August 28, 2016. Make every attempt to post on different days earlier in the week to provide a scholarly exchange of ideas. References, citations, repeating the question, and quoting your peer do not count towards the 100-word minimum.
3. Take M1A2 content quiz to finish by 11:59 PM Eastern Standard Time US on Sunday, August 28, 2016
nursing 104 modules 1 paper.
The RN is developing a plan of care for an 86 year old patient who was admitted after falling at home. The patient is confused to place and time and has a right hip fracture that will be repaired tomorrow.
Question:
Develop A plan of care for this patient that includes the actions the RN will take for each step of the nursing process. Be sure to include how critical thinking will be used in the development of the plan.
Please cite two references from the textbook APA style
Textbook to use for this paper: Treas, L. & Wilkinson, J, (2014). Basic nursing: concepts, skills & reasoning. Philadelphia; F. A. Davis, Company.
Specific areas & chapters to read and collect information for this paper?
Basic nursing: concepts, skills & reasoning**
• Chapter 2: Critical thinking and the nursing process
• Chapter 3: Assessment
• Chapter 4: Diagnosis
• Chapter 5: Planning Outcomes
• Chapter 6: Planning Interventions
• Chapter 7: Implementation and Evaluation
• Chapter 18: Documenting and Reporting
• Chapter 44: Nursing
• Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Nursing Diagnosis Guidebook – A pocket-size nursing diagnosis guidebook of your choice that is no more than one edition old, that includes NANDA International-approved nursing diagnoses, definitions, defining characteristics, and possible nursing Interventions.
Nur213 module 1 paper.
Using the assigned readings and information from the literature, compose a response to the following statement:
Question: Patients with Ebola virus disease (EVD) should not receive CPR.
For this activity, you will weigh in on the RN’s ethical obligation when providing care to patients with EVD and the performance of CPR.
Please cite two references from the textbook APA style
Required Textbooks and assigned reading for this paper:
Brunner and Suddarth’s textbook of medical-surgical nursing**
• Chapter 3: Critical Thinking, Ethical Decision Making, and the Nursing Process
• Chapter 23: Management of Patients With Chest and Lower Respiratory Tract Disorders (section on “Pulmonary Tuberculosis”)
• Chapter 35: Assessment of Immune Function (section on “Function of the Immune System”)
• Chapter 37: Management of Patients With HIV Infection and AIDS
• Chapter 42: Management of Patients with Musculoskeletal Disorders (section on Musculoskeletal Infections”).
• Chapter 49: Assessment and Management of Patients With Hepatic Disorders (sections on “Viral Hepatitis, “Hepatitis A, B, and C”, and “Nonviral Hepatitis”)
• Chapter 55: Management of Patients With Urinary Disorders (sections on “Infections of the Urinary Tract”)
• Chapter 69: Management of Patients With Neurologic Infections, Autoimmune Disorders, and Neuropathies (section on “Infectious Neurologic Disorders”)
• Chapter 71: Management of Patients with Infectious Diseases
Pharmacology: A patient-centered nursing process approach**
• Chapter 14: Medications and Calculations
• Chapter 29: Penicillins and Cephalosporins
• Chapter 31: Sulfonamides
• Chapter 32: Antituberculars, Antifungals, Peptides, and Metronidazole
• Chapter 34: Drugs for Urinary Tract Disorders
• Chapter 36: Vaccines
Maternal & Child Health Nursing**
• Chapter 40: Nursing is of a Family When a Child has a Respiratory Disorder (section on Disorders of the lower respiratory tract: influenza and tuberculosis)
• Chapter 42: Nursing Care of a Family When a Child has an Immune Disorder
• Chapter 43: Nursing Care of a Family When a Child has an Infectious Disorder (section on “Infection”)
•Chapter 45: Nursing Care of a Family When a Child has a Gastrointestinal Disorder (section on “Hepatitis”)
• Chapter 49: Nursing Care of a Family When a Child has a Neurologic Disorder (section on “Bacterial Meningitis”)
• Chapter 51: Nursing Care of a Family When a Child has a Musculoskeletal Disorder (section on “Infectious and Inflammatory Disorders of the Bones and Joints”)
Nursing Diagnosis
• Use your chosen Nursing Diagnosis Guidebook to review the nursing diagnoses specific to the content covered in this module.
Web-based and Other Professional Resources:
• Hand Hygiene in Healthcare Settings
• Hospital: 2016 National Patient Safety Goals**
• Pre-licensure KSAs (2014)**
• Ebola virus disease: an emerging threat (2014)**
• Zika virus (2016)**
M1D1: The Ethical Obligations of the RN Providing care to the Patient with Ebola Virus Disease
Ethical Issues in the Response to Ebola Virus Disease in US Emergency Departments: A Position Paper of the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine
Arvind Venkat, MD, FACEP,
Lisa Wolf, Ph.D., RN, CEN, FAEN,
Joel M. Geiderman, MD, FACEP,
Shellie L. Asher, MD, FACEP,
Catherine A. Marco, MD, FACEP,
Jolion McGreevy, MD, MBE, MPH,
Arthur R. Derse, MD, JD, FACEP,
Edward J. Otten, MD, FACMT, FAWM,
John E. Jesus, MD, FACEP,
Natalie P. Kreitzer, MD,
Monica Escalante, MSN, BA, RN,
Adam C. Levine, MD, MPH, FACEP,
on behalf of the
American College of Emergency Physicians,
the
Emergency Nurses Association,
and the
Society for Academic Emergency Medicine
Show more
http://dx.doi.org.vlib.excelsior.edu/10.1016/j.jen.2015.01.012Get rights and content
Referred to byAnne Manton
Editor’s Note regarding the on-line position paper, “Ethical Issues in the Response to Ebola Virus Disease in US Emergency Departments: A Position Paper of the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine”
Journal of Emergency Nursing, Volume 41, Issue 2, March 2015, Page 99
PDF (58 K)
M1D1: The Ethical Obligations of the RN Providing care to the Patient with Ebola Virus Disease
The 2014 outbreak of Ebola Virus Disease (EVD) in West Africa has presented a significant public health crisis to the international health community and challenged US emergency departments to prepare for patients with a disease of exceeding rarity in developed nations. With the presentation of patients with Ebola to US acute care facilities, ethical questions have been raised in both the press and medical literature as to how US emergency departments, emergency physicians, emergency nurses and other stakeholders in the healthcare system should approach the current epidemic and its potential for spread in the domestic environment. To address these concerns, the American College of Emergency Physicians, the Emergency Nurses Association and the Society for Academic Emergency Medicine developed this joint position paper to provide guidance to US emergency physicians, emergency nurses and other stakeholders in the healthcare system on how to approach the ethical dilemmas posed by the outbreak of EVD. This paper will address areas of immediate and potential ethical concern to US emergency departments in how they approach preparation for and management of potential patients with EVD.
Keywords
Ethics;
Ebola virus disease;
Emergency department
Introduction
In March 2014, an outbreak of Ebola Virus Disease (EVD) was confirmed in the West African nation of Guinea with subsequent rapid spread to the neighboring countries of Liberia and Sierra Leone. Given the underdeveloped health infrastructures in the 3 primary affected nations and the high transmission and mortality rate of the disease, domestic and international public health agencies called for aid and personnel to be rapidly deployed to the affected nations to treat infected patients and prevent further spread of the Ebola outbreak. Yet despite significant efforts from the international community, EVD continues to represent a significant challenge in the region. As of January 2015, the Centers for Disease Control and Prevention (CDC) reports that the total case count stands at 21,689 with 8,626 deaths and continues to rise.1
In the United States, the transfer of Ebola-infected healthcare workers from the outbreak zone to US hospitals raised public awareness and fear of the spread of the disease. This fear was heightened after the initial missed diagnosis in a US emergency department of a patient with EVD who later died,2 the transmission of Ebola to 2 nurses who cared for this patient3 and a subsequent case of an emergency physician who traveled to West Africa to care for patients with EVD and required hospitalization after returning to the United States.4 These cases raised significant concerns that US emergency departments and hospitals were not adequately prepared to diagnose and treat patients with EVD. In addition, the infection of healthcare personnel created the specter of a more widespread outbreak in the general population due to poor infection control guidelines, inadequate training, and management protocols in US medical centers and initially absent mechanisms to identify potentially infected individuals arriving through US ports of entry.5 A subsequent controversy surrounding a nurse who returned from West Africa without symptoms of EVD and was held in quarantine highlighted concerns about how personal liberty and public health should be appropriately balanced.6 In response, both emergency medicine and emergency nursing organizations and federal agencies have issued guidance on the nature of EVD, approaches to identification, isolation, and treatment of potential patients and standards for use of personal protective equipment (PPE) by healthcare providers.7, 8 and 9
While the number of cases in the United States remains low to date (10 total patients, 4 diagnosed in the US and 2 deaths), the outbreak of EVD has raised ethical issues relevant to US emergency departments and hospitals, emergency physicians and emergency nurses. Issues articulated in the medical literature and by the press include the following: how resources should be used in preparation for the likely rare event of an undiagnosed patient with EVD who presents to a US emergency department,10 whether there should be a different standard for care of Ebola-infected patients than for other patients with less contagious and lethal diseases11 and whether healthcare providers are obligated to place themselves at a significant degree of risk while caring for these patients due to their professional status.12 To address these concerns, the American College of Emergency Physicians (ACEP), the Emergency Nurses Association (ENA), and the Society for Academic Emergency Medicine (SAEM) developed this joint position paper to provide guidance to US emergency physicians, emergency nurses and other stakeholders in the healthcare system on how to approach the ethical issues posed by the outbreak of EVD. This paper will address areas of immediate and potential ethical concern to US emergency departments in how they approach preparation for and management of potential patients with EVD.
Ebola Virus Disease Patients Should not Receive CPR and Characteristics of EVD of Ethical Relevance
Since the outbreak of EVD, numerous articles have been published on the epidemiologic characteristics of this condition and the microbiological details of the causative organism.13, 14, 15 and 16 However, particular characteristics of EVD are worth highlighting to provide the factual basis for addressing the ethical questions raised in this outbreak for US emergency departments. First, it is well recognized that individuals with EVD will often have relatively non-specific symptoms, common to many viral infections, in their initial stages of presentation (eg, fever, headache, myalgias).15 and 17 Such non-specific presentations make unrecognized infection with Ebola a realistic concern. Lack of prompt identification of potential patients by emergency department staff can increase the risk of spread of the disease and mandates a heightened awareness of the risk factors for the disease. Second, the pathophysiology of contagion is related to contact with blood or bodily fluids from an infected individual, with rising viremia in the late stages of disease presenting a particular risk for human-to-human transmission. However, even a low level of viral inoculation can lead to EVD.18 This recognized pathway of spread aids in evaluating the risk of transmission from patient to healthcare providers or the general public. At the same time, knowledge of how the Ebola virus is transmitted heightens the ethical concerns posed by the potential presence of the highly symptomatic and contagious patient(s) to an emergency department, especially if to a center without specialized experience in the care of EVD patients. Finally, the lack of specific effective treatment and the high mortality rate posed by EVD exacerbates public fears, may create irrational panic relative to the actual risk and lead to unexpected institutional consequences such as the avoidance of the use of healthcare facilities where EVD patients are being or have been treated.
Ebola Virus Disease Patients Should not Receive CPR and Characteristics of Emergency Department Practice of Ethical Relevance
The emergency department in the United States and increasingly worldwide serves as the primary gateway to the acute healthcare system. It is estimated that 50% of admissions to hospitals in the US are initially assessed and treated in emergency departments.20 The emergency department is also the only access point in the US acute healthcare system available to patients 24 hours per day-7 days per week. In the US there is a legal obligation under EMTALA to provide a medical screening exam for an emergency medical condition and treatment until the emergency medical condition is resolved or stabilized to the extent of that hospital’s capability (until appropriate transfer) regardless of insurance status or other socioeconomic factors.21 and 22 Finally, the emergency department is the primary location for the initial evaluation, diagnosis, and treatment of the acutely ill undifferentiated patient. These facts together help define the ethical construct of emergency medical practice where access to quality emergency care is a right of all patients in the US. As noted in the ACEP Code of Ethics, “Emergency physicians shall respond promptly and expertly, without prejudice or partiality, to the need for emergency medical care.”23 The ANA Code of Ethics states that “The emergency nurse works to improve public health and secure access to health care for all.”24 The Society for Academic Emergency Medicine, through its mission statement “to lead the advancement of emergency care through education and research, advocacy, and professional development in academic emergency medicine,”25 also supports the ethical mandate for all patients in the United States to have access to quality emergency medical care regardless of disease process, ability to pay or other characteristics.
While the above ethical framework emphasizes the critical importance of the availability of emergency care to all, it is clear from both published codes of ethics and the literature on the “duty to treat” that there are rare circumstances in which risk to the individual healthcare provider and institution should be weighed in determining the treatment plan for a patient who poses a significant risk to providers or the general public. The ACEP Code of Ethics notes the requirement of the adequacy of in-hospital and outpatient resources in the provision of emergency care.23 The American Medical Association Code of Ethics states that “Because of their commitment to care for the sick and injured, individual physicians have an obligation to provide urgent medical care during disasters. This ethical obligation holds even in the face of greater than usual risks to their own safety, health or life. The physician workforce, however, is not an unlimited resource; therefore, when participating in disaster responses, physicians should balance immediate benefits to individual patients with ability to care for patients in the future.”26 The American Nurses Association Code of Ethics specifically states, “The nurse owes the same duties to self as to others, including the responsibility to preserve integrity and safety.”27 Within the larger ethics literature, explorations of whether there is a duty to treat on the part of healthcare providers at risk to themselves also indicate that codes of ethics, historical references, and theoretical analysis do not mandate an absolute obligation. Rather, particular factors of disease process, availability of resources and training, countervailing responsibilities outside of the professional realm, personal viewpoints on the virtues of courage and resilience as well as relational ethics perspectives and obligations imposed by professional status have guided the evaluations of the obligations of healthcare providers in the face of outbreaks of infectious disease.28, 29, 30 and 31 For emergency departments, emergency physicians and emergency nurses, there is a need to weigh all of these considerations against the special role played by emergency departments in the US healthcare system and the duties that accompany the professional status of emergency physicians and emergency nurses.
Current and Potential Future Ethical Considerations with the Outbreak of EVD
With this background, we will present an ethical framework that has potential application for emergency departments, emergency physicians and emergency nurses along with other health system stakeholders in the particular response to EVD in the United States. This framework will address questions relevant to US emergency departments and separate consideration of the current situation (few confirmed cases within the United States with a relative abundance of resources to respond) versus 2 potential scenarios (increasing number of potential and confirmed domestic cases of EVD in a variety of locations due to spread in the US and widespread number of potential and confirmed domestic cases that would strain existing resources and creates a necessity of disaster triage response) where appropriate.
What are the Ethical Obligations of US Emergency Departments and Hospitals to Support or Encourage the Volunteering of Emergency Physicians and Emergency Nurses to Serve as Healthcare Providers in those Countries Most Affected by the Current Outbreak of EVD?
In the current outbreak of EVD, as of January 1, 2015, there are no extant active cases in the United States. As such, the most immediate issue is how to contain the spread of the disease from its present locus in West Africa and end the current epidemic there. With the underdeveloped nature of the health infrastructure in the primarily affected nations and the declaration of a Public Health Emergency of International Concern by the World Health Organization,32 there is widespread recognition that ending the epidemic does and will continue to require the volunteering of healthcare providers to serve in the outbreak zone.
Under the ethical principle of reciprocity, which calls for acting in a manner that one would want others to act in return, there is an obligation to support emergency physicians and nurses who volunteer to serve in the nations primarily affected by the current Ebola epidemic, just as we would welcome support or available expertise in a time of health crisis in the US. Yet as a practical matter, support of volunteerism needs to be weighed against the special logistical concerns faced by most emergency departments, where local staffing levels must be maintained to provide safe patient care. An application of the principle of reciprocity in this outbreak would include support of emergency physician and nurse volunteerism in the current outbreak through the covering of shifts and other professional obligations in the volunteer’s absence and acceptance by volunteering emergency physicians nurses of any potential risk of contagion on return to the US and the resultant need for monitoring for signs of the disease and possibly prolonged isolation.
We would propose that in considering the support of volunteerism by emergency physicians and nurses, the specific background, training, and education of the provider is a key decision making a factor. Education and training are essential components of preparation prior to disaster or disease outbreak response. Medical volunteers should be appropriately trained in disease management, including rendering effective supportive care within the resource constraints in the primary outbreak zone, prior to travel to infected areas. They should ensure to the extent possible that malpractice, health, and life insurance are in place to cover potential events, likely with the assistance of the Non-Governmental Organization or other agency sponsoring their volunteer efforts. They should be willing to undertake the risks of volunteerism, including infection or threats to individual safety and security.33, 34 and 35 Volunteers should be prepared to ensure appropriate infection control practices in their international work and to follow recommended protocols upon return for monitoring for symptoms of EVD and the isolation that might result.36, 37 and 38 Without this preparation, volunteering emergency physicians and nurses may be a liability rather than a benefit to the resource-poor countries primarily affected by the Ebola outbreak and a risk to the domestic population upon their return to the US.
It is appropriate for emergency departments and hospitals to query volunteering staff on their willingness to undergo the necessary training to be effective in the primary outbreak zone. With the continuing spread of the disease in West Africa, those volunteering emergency physicians and nurses with existing experience in Ebola and disaster response should be given priority over those without such training. Specific decisions regarding support for volunteer efforts should also include the number of volunteers and impact on ED staffing and potential impact on public health domestically (i.e., will the loss of experienced providers adversely affect the care of patients in the local area served by the emergency department?). If the current outbreak were to spread significantly within the US, the ethical evaluation of the appropriateness of supporting volunteerism overseas would likely change since this could result in the expertise on the management of EVD being shifted out of the country rather than being available domestically. This emphasizes the importance of supporting present efforts of containing and ending the current epidemic in West Africa, including with the volunteerism of trained emergency physicians and nurses, as the most effective means of preventing the spread of EVD to the US and other countries.
Some emergency departments have supported the volunteerism of emergency physicians in particular through altruistic coverage of shifts to allow staff to travel to the primary outbreak zone.39 In addition, private foundations have provided grant funding to alleviate the financial burden of volunteerism of emergency department staff in the outbreak zone.40 While these novel approaches have been largely confined to academic settings, they do suggest that there may be methods for individual centers to address the logistical difficulties that can arise when US emergency department providers volunteer in the primary outbreak zone. The application of these options to individual centers is one that is best judged on a case-by-case basis based on the factors noted above.
Finally, emergency departments, emergency medicine and nursing professional societies, Non-Governmental Organizations and government agencies can aid volunteer efforts by educating health care providers and the lay public using published evidence on the pathophysiology of Ebola and its transmission to alleviate the stigma that returning volunteer staff may experience after their efforts. At the same time, as noted above, volunteering emergency physicians and nurses have an obligation to adhere to monitoring and isolation protocols upon return to the US as a reciprocal ethical obligation for the support their efforts have received.
What are the Ethical Obligations of Emergency Departments and Hospitals to Support other Centers in the Domestic Response to EVD?
As of December 2014, 44 medical centers have been designated by the Centers for Disease Control and Prevention as having the necessary capability and equipment to care for patients diagnosed with EVD.41 It is anticipated that patients with a confirmed EVD diagnosis will be transferred to these hospitals which will have enough PPE and other treatment requirements (isolation rooms, dedicated equipment and designated physicians, nurses and other necessary health care professionals and staff with proper training under CDC guidelines) to manage patients for at least 7 days, after which governmental agencies would assist in acquiring more supplies and expertise if needed.42 However, not every state or locality has such a facility, nor is it likely that an undiagnosed patient would necessarily present to one of these centers. Therefore, the CDC has provided guidelines for so-called frontline (any emergency department or acute care facility) and Ebola assessment hospitals, which can safely isolate, treat and transfer patients with suspected or confirmed EVD. To meet these standards, the CDC has called for all emergency departments to have protocols in place for the recognition of potential Ebola patients and training for the proper isolation and assessment of these individuals.42
The hierarchy of treatment facilities for EVD codifies the reciprocity-based obligations that hospitals have to each other in the current state of the outbreak. Such reciprocity should extend to the sharing of PPE, trained staff and other necessary equipment as needed to care for a suspected or confirmed Ebola patient until the transfer can be effected to a designated treatment center. Hospitals and emergency departments should consider and develop relevant protocols for rapid credentialing of staff and transfer of equipment to allow resources to be brought to bear should there be additional cases in the US. If the current epidemic were to spread significantly in the US, hospitals should consider whether and how they can upgrade their capabilities to meet the needs of rising numbers of patients, presumably with the assistance of government resources.
Another ethical consideration is the reputational impact upon hospitals caring for Ebola patients. As has been reported in the press, hospitals have expressed concern that the potential costs and risks accrued in treating an Ebola patient along with the public fear generated by the disease may have an adverse impact on volumes and financial results for medical centers. The facility in Dallas that treated a recent case reported that afterward emergency department volumes dropped and still have not returned to their expected level.19 It is therefore imperative, in the face of a disease such as Ebola that has generated such public scrutiny and at times hysteria, for hospitals to be cognizant of their ethical responsibility to support the efforts of designated treatment centers as well as frontline facilities that might encounter Ebola patients and potentially be perceived adversely by the public. We affirm that the principle of reciprocity extends beyond physical means of support (equipment, personnel) to reputational support in the setting of an outbreak of EVD. Such support could, where appropriate, take the form of publicly confirming the safety and quality of other healthcare facilities with Ebola patients, educating other facilities on effective policies and procedures in caring for EVD patients and avoiding messages that implicitly suggest a competitive advantage from not treating patients with this highly infectious disease. Through such support, hospitals ensure that the public is aware and reassured of the unified response the medical system will take towards both the existing epidemic and the potential for worsening if the outbreak spreads from West Africa. Without such reputational support and cohesion in the healthcare system, should the epidemic worsen, it is conceivable that public doubt and panic may lead to untenable consequences such as facilities avoiding the care of at-risk patients and the public fearing certain hospitals as being sites of contagion rather than medical care?
Should Trainees be Allowed to Participate in the Care of Suspected or Confirmed EVD Patients?
Trainees (nursing students, medical students, residents, and fellows) routinely care for patients with infectious diseases in the ED and should understand and use proper measures to protect themselves while caring for patients with potential or confirmed contagious diseases. Both the Accreditation for Graduate Medical Education program requirements in emergency medicine and guidance on Ebola affirm that trainees should know how to recognize, treat and isolate patients with infectious disease in general and Ebola specifically.43 and 44 The 2013 Model of the Clinical Practice of Emergency Medicine goes further by listing within the domain of emergency medicine “understand[ing and apply[ing] the principles of disaster and mass casualty management including preparedness, triage, mitigation, response, and recovery.”45 Additional content areas in the Model relevant to Ebola response include the following: personal protection (equipment and techniques); universal precautions and exposure management; and emerging infections, pandemics and drug resistance.45 Together, these raise the issue of whether the current EVD outbreak should be viewed as an opportunity for trainees in emergency medicine and emergency nursing to care for patients during an international infectious disease epidemic. Few health care professionals in the United States have experience with the diagnosis and treatment of Ebola or the infection control precautions required to safely care for patients with this disease. Yet some such individuals may include trainees either with specific backgrounds in infectious diseases or previous experience with the PPE utilized in caring for such patients.
Historically, the outbreak of an unknown or uncommon infectious disease has led to initial concerns by health providers about the risk to self that ultimately gives way with time and knowledge to acceptance of an affirmative duty for trainees to learn to treat patients with these conditions. For example, the early fear and stigma surrounding HIV-infected patients in the 1980s gave way to a widely recognized duty to treat these patients and instill the same ethic in trainees.46 As knowledge of the pathophysiology and epidemiology of EVD and its implications for healthcare providers become more widely disseminated, a similar evolution may take place. However, based on the current conditions of the Ebola outbreak, it is likely that very few of these professionals will need to be called upon to fulfill this duty.
As long as the Ebola incidence in the United States remains low, each institution can and should manage its burden of suspected Ebola cases with a cadre of nurses and physicians highly trained in Ebola treatment and prioritize infection control. The ethical justification to restrict the number of caregivers who come in contact with Ebola-infected patients is that, given the limited experience with the disease in the United States, unnecessary exposure to infected patients would increase the risk to providers, other patients, and the public. It is prudent to limit the potential chain of infection when possible.
Because experienced or specially-trained nurses and attending physicians can effectively manage suspected or confirmed Ebola cases, trainee involvement is not required and would entail unnecessary risks to trainees and their patients. Trainees should, however, be fully prepared in case they find themselves in a position where their duty to treat an individual patient outweighs a duty to the public to limit exposure to the disease.44 However, if not trained or equipped properly, their duty to reasonably protect their own safety should not be superseded.
Non-participation of trainees in the care of Ebola-infected patients is then an instance of exclusion, rather than exemption. Institutions exclude trainees as an infection control strategy; trainees do not opt out. Some trainees may object to these policies, as they may feel ethically compelled to care for Ebola-infected patients as a function of their professional role and view their exclusion as a restriction of their own moral agency and liberty (to fulfill their commitment to treating the sick).39 However, this restriction is justified by the greater good of protecting public health. Ensuring trainee well-being and availability to care for other ED patients as well as limiting contagion are ethically justifiable reasons to exclude trainees. Exclusion of trainees from the care of Ebola-infected patients is not simply paternalistic because the primary aim is to protect patients and the public and represents a proportional response relative to the professionalism and moral agency consideration of trainees.47
At the same time, a blanket exclusion of trainees from the care of Ebola patients in the primary outbreak zone may be ethically inappropriate. If the trainee has the relevant experience and is able to meet the other requirements outlined above for volunteerism in the countries most affected by Ebola currently, a case-by-case evaluation would seem appropriate for supporting the participation of volunteering trainees in the international response where there is a desperate need for available healthcare providers.39 Such support would have the added benefit of growing the cadre of individuals with the relevant expertise in caring for patients with EVD should the current outbreak spread to the US. However, it is worthy of consideration whether academic medical centers can appropriately manage the risk to their trainees in the conditions posed by the outbreak in West Africa. There are additional reputational risks should a trainee contract Ebola or the public adversely view institutions where a large cadre of providers, including trainees, have traveled to care for patients in the primary affected countries.39
As such, we affirm the ethical appropriateness of academic medical centers to consider on an individual provider basis whether a trainee should be supported in volunteering to travel to Africa rather than endorsing a policy of automatic exclusion or support of providers in this regard. Such individualized evaluations should take specific account of the level of training, previous background, experience with Ebola and the PPE required to care for patients with this disease, the ability to undergo the necessary preparation for functioning effectively in the primary outbreak zone and the willingness to comply with monitoring and isolation protocols upon return to the US.
Is it Ethically Appropriate for Emergency Physicians or Emergency Nurses to Opt Out of the Care of Patients With EVD?
Under the current state of the Ebola outbreak, it is anticipated that cases in the US would be scattered and readily managed at designated treatment centers.41 At the same time, it is recognized that suspected patients may present to frontline emergency departments without specialized expertise in the management of EVD,42 and, as seen in the case of the patient in Dallas, this may pose a risk to health care providers, including emergency physicians and emergency nurses.3 As a result, various health care providers have expressed reluctance to care for patients with Ebola.48, 49, 50 and 51 Historically, such provider reluctance has often arisen with the emergence of unknown infectious diseases.29 A 2008 survey of thousands of healthcare workers in New York found that half would hesitate or refuse to report to work during a Severe Acute Respiratory Syndrome (SARS) outbreak (though 84% would report to work during a mass casualty situation). Most cited concern for family, followed by concern for self, as reasons not to report to work during a SARS epidemic. 52 Individual conscience then, rather than professional tradition, seems to be the main force that compels nurses and physicians to risk their lives in service of patients. 29 and 46
With this background, it is fair to ask whether there are circumstances under which emergency department providers could opt out of the care of Ebola patients. Under US law, nurses and physicians have a legal duty to treat patients with whom they have entered into a therapeutic relationship. Once undertaken, the duty continues until the patient and professional mutually agree to end the relationship or the care is transferred to another professional.53 Nurses and physicians have special duties in service of the sick, and since this obligation holds even in face of greater than usual risks to one’s own safety, healthcare professionals consequently accept greater risks than ordinary, balancing immediate benefits to individual patients with the professional’s own health and ability to treat future patients.54 But there is no consensus on the specific limits of this duty.30 and 55
Emergency nurses and physicians are front line in an outbreak and, implicit in their specialty choice, accept additional risk beyond what is typical for many of their colleagues. As noted above, this is acknowledged in professional codes of ethics and statutory mandates (e.g., EMTALA).21, 22, 23, 24 and 26 There are potential additional penalties for those health care professionals who refuse to work or treat patients during a pandemic, including reduction in pay, termination and, in some states that have adopted variations of the Model State Emergency Health Powers Act (MHEHPA), the possibilities of licensure actions, fines or imprisonment.56 and 57
Though the legal foundations of the duty to treat and its consequences are significant, the most compelling ground for these obligations is that health care is a moral enterprise.29 and 58 “All its efforts converge ultimately on decisions and actions which are presumed to be good for some person in need of help and healing.”58 Nurses and physicians have a professional commitment to heal the sick. They are morally accountable to this commitment and are expected to demonstrate the virtues that it entails—such as courage, compassion and fidelity.29 and 59 This virtue-based ethic is independent of the patient’s right to access to healthcare and the contract between the patient and physician. Rights-based and contract-based accounts of the duty to treat would allow nurses and physicians to opt out of caring for patients in an epidemic as long as others were willing to take their place.28 But nurses and physicians who opt out in such cases still fall short of their moral commitment.29
Emergency nurses and physicians, therefore, have a duty to care for Ebola-infected patients and, in most instances, accept the associated risks.30 and 60 But the duty is not unlimited. An “abstract limitless duty” obscures the discussion about reasonable risk acceptance among nurses and physicians.60 Allowing for reasonable and practical limits to the duty to treat—applied equitably to all clinicians—may increase the likelihood that nurses and physicians will live up to their individual obligations during an outbreak.30
The limit is illustrated by an account of a physician who, during the 1995 Ebola outbreak in the Democratic Republic of the Congo, “found 30 dying patients in an abandoned hospital, left to care for themselves amid rotting corpses, sometimes in the same bed.”30 A nurse or physician should not be expected to treat patients in a context where the risks are extraordinarily high and the potential benefit to patients extremely low.30 Indeed, the first duty of emergency nurses and physicians in the current Ebola outbreak or other emerging infectious disease is to protect themselves in the care of patients, if for no other reason than to ensure their availability to treat subsequent patients.61 By contrast, care of Ebola-infected patients in a US hospital with the proper PPE and training would fall well within the duty to treat.15
In the current state of the Ebola outbreak, establishing cadres of highly trained clinicians at well-resourced institutions may be the best way to deliver uniform care under a duty to treat and limit potential spread of infection in the US.42 Under the above noted virtue and professionalism-based ethical framework,23, 24, 26, 58 and 59 emergency nurses and physicians may also volunteer in place of colleagues who they see experiencing exceptional moral or emotional distress over caring for Ebola-infected patients—for example, as a result of unusually severe consequences for loved ones should they become ill. But as the burden of Ebola-infected patients rises, the duty to treat is a responsibility of all emergency nurses and physicians who have the necessary training, skills and experience.
While the duty to treat is intrinsic to health care professionals, institutions may also hold emergency nurses and physicians accountable to this standard. However, institutions may not invoke the duty to treat to coerce hospital employees into accepting unnecessarily dangerous conditions: for example, to expect them to deliver care to Ebola-infected patients without proper PPE or training. Institutional leaders have an ethical responsibility to prepare for outbreaks, ensure that the providers who risk their lives in the service of patients do so with as much protection and support as possible and make available appropriate channels for emergency physicians and nurses to communicate concerns about the adequacy of the training and preparation they receive. Preparation includes, but is not limited to, making high quality PPE readily available, ensuring that all relevant staff are educated and trained to use it properly (especially proper donning and doffing) and limiting exposure to only those individuals needed to care for patients and prevent the spread of infection.
Experience with the 2003 SARS epidemic in Canada suggests that hospital leaders owe even more than merely providing equipment and training to nurses and physicians who fulfill their duty to treat under hazardous conditions. Some healthcare workers died from SARS, and some spread the disease to their families.55 Healthcare workers have moral obligations to their families, and institutions should make it possible for them to care for patients without abandoning their responsibility to their families or risking their families’ lives. Institutions should, for example, assist with child care and provide temporary living quarters to reduce the risk of disease transmission to family members and the associated anxiety and moral distress.62 Institutions, as well as public health agencies, may also consider additional acts of reciprocity toward healthcare workers who fulfill their duty to treat, such as insurance to protect them and their families should they become ill or die as a result of caring for Ebola-infected patients. Ultimately, however emergency nurses and physicians care for the sick primarily out of personal moral obligation; financial incentives alone are not likely to increase the likelihood that they will discharge their duty under epidemic conditions.63
The protections that institutions and society provide healthcare workers—for themselves and their families—are ethically required. Just as emergency nurses and physicians may not generally opt out of caring for the sick, institutions and communities may not opt out of caring for healthcare professionals and their families. In sum, the duty to treat patients with infectious diseases, including Ebola, is both a legal responsibility and an ethical obligation of the healthcare professions. The duty should be borne equitably by professionals, who in turn, should be adequately supported by institutions and society as a whole.
Given the expected low number of US cases, there is a role for institutions to ask healthcare providers to volunteer to serve on treatment teams for suspected Ebola patients as a means of limiting training efforts, time and expenditures (eg, credentialing of the ability to perform invasive procedures with PPE), reducing the potential risk of infection and ensuring relevant personnel and expertise are available to provide care. However, such volunteer-based plans do not address the special role of emergency departments where patients may present in an undifferentiated manner and potentially in acute distress, and where alternative providers may simply not be available. For emergency physicians and nurses, who through their choice of profession knowingly accept the above circumstances of patient care,23 and 24 the current state of the Ebola outbreak does not justify opting out of the care of suspected or confirmed Ebola patients who may present to the emergency department, but this obligation is contingent upon institutional and governmental resources that provide adequate training and equipment to fulfill this duty. There also needs to be a recognition by healthcare personnel, hospitals and other public health and legal authorities as well as patients that the duty of emergency physicians and nurses to treat must be absolutely contingent on first ensuring personal safety through the proper use of PPE.61 and 64 Should Ebola rise in prevalence in the US, contingency planning to meet the duty to treat should move beyond training and equipment to mechanisms to support the weighty obligations of emergency physicians and nurses to protect themselves and their families while caring for affected patients.
Are the Goals of Care Different in Patients Critically Ill with EVD?
With the high mortality rate, lack of specific treatment and need for specialized PPE in order to prevent transmission, there have been legitimate questions whether the goals of care should change in patients critically ill with EVD. Specifically, in the circumstance where a patient requires procedural interventions (central venous access, intubation, dialysis, etc) to provide intensive care level support, is the risk posed to providers too high compared to the low potential of benefit, if any, to a patient whose illness may have progressed to a point where such interventions are unlikely to be successful? Furthermore, given the time needed to don PPE—an absolute requirement prior to any procedural intervention on an EVD patient—should cardiopulmonary resuscitation during an arrest event be considered futile due to the potential delay in its initiation and again the likely prognosis of the patient?11, 64 and 65
Since the initial posing of these concerns about the risk versus benefit posed by critical care and resuscitation interventions in patients with EVD, case reports have appeared showing that aggressive, intensive care level interventions, including intubation, central venous access, large volume and blood resuscitation and dialysis, can be successful in treating critically ill individuals with this disease and do not pose an automatic risk to providers if PPE is properly used.66 and 67 While anecdotal and representative more of what is possible in idealized circumstances (specialized care units with previous expertise and training in care of EVD patients and a high number of dedicated providers), these cases imply that utilizing the full panoply of critical care resources for this patient population may be appropriate treatment. However, the highly contagious nature of EVD and the need for specialized PPE, along with the experience in Africa of rapid transmission to family members caring for ill patients, makes it appropriate for hospitals to not allow family presence during such procedures as is allowed in other critical care or resuscitation circumstances.
With respect to cardiopulmonary resuscitation, to our knowledge, no published report has indicated the successful or unsuccessful use of cardiopulmonary resuscitation in an arrest event in an Ebola patient, though resuscitation success in a US healthcare facility may be similar to other infectious diseases at similar stages, from initial manifestations to overwhelming sepsis. At this time, consideration of do-not-resuscitate status in a late-stage EVD patient is best determined on a case-by-case basis, taking into account potential benefit to the patient, any limitations of interventions imposed by the disease and the potential risks to the treatment team.
However, the circumstances described for the above patients are not typical of that seen in most emergency departments in the US. While the current state of the outbreak would likely lead to a typical ED encountering a patient early in their EVD process, if at all, and being able to isolate such an individual until transfer to a higher level of care, should the number of cases rise due to spread of the disease, it is conceivable that emergency departments could encounter patients in a variety of stages of Ebola with the risk-benefit calculation on procedural interventions being highly relevant. Unlike the above cases, should the current outbreak spread, emergency departments would encounter patients with fewer resources (less isolation facilities, lower ratios of providers to patient) than those expended in the above reported cases and having to simultaneously care for other patients with a variety of conditions. Here there is need to refer to the special role played by emergency physicians and nurses in the healthcare system. The assumptions that accompany the choice of these professional roles (exposure to acutely ill, undifferentiated patients) and the specialized training and skills that emergency physicians and nurses possess impose a higher obligation than other medical professionals to be prepared to treat an acutely ill Ebola patient in the emergency department setting.23 and 24
At the same time, as we note above, the duty to treat is not absolute. There is no obligation for an emergency physician or nurse to implement treatment measures in an acutely ill Ebola patient without training in the use of PPE, the availability of such supplies and, at a minimum, simulated experience with performing critical care procedures while utilizing PPE.15, 28 and 61 Without such minimum standards, the social contract that accompanies the professional standing and obligations of emergency physicians and nurses breaks down. This social contract calls for a rational person to expect an emergency physician or nurse to apply their skills to aid an acutely ill patient but at the same time for those professionals to have the requisite training and equipment to provide such aid in an appropriate manner.68
All emergency departments and hospitals should therefore consider that protocols for PPE training and isolating suspect patients, as called for in the current interim CDC guidelines,42 are likely inadequate should the current epidemic spread more prominently to the US. To fulfill the ethical obligations imposed by the duty to treat should the current outbreak become more prevalent domestically, more robust training with PPE and the performance of procedures with such equipment will be necessary for a wider cadre of emergency physicians and nurses to appropriately treat acutely ill Ebola patients in intermediate or late stages of the disease while ensuring the maximum feasible protection of the healthcare provider. Weighing when such expanded training may be warranted should take into account the continued status of the outbreak, the cost of such preparation and the availability of appropriate resources to be effective.
In the unexpected scenario where the number of patients with EVD overwhelms existing resources, more traditional disaster triage protocols would be applicable. Such protocols attempt to apply resources in a manner to benefit the largest number of patients. In the case of Ebola, where the evidence to date is that an overwhelming amount of critical care resources are required to effectively treat a late-stage patient, disaster triage protocols would need to weigh at what point in the treatment spectrum such resource expenditure would become untenable. Such protocols, to be ethically appropriate, would need to be transparent, proportionate and accountable to oversight along with having a legal imprimatur to be effective in the emergency department and acute care setting.69 To avoid such a crisis situation, the devotion of resources now to end the epidemic in the primary outbreak zone in Africa is vital.
Future Considerations
The outbreak of EVD in West Africa has presented a significant challenge to the health systems of the primary affected nations and, even with a low case count, raised concerns about the preparedness of the US healthcare system to respond to uncommon infectious diseases. In some ways, Ebola is a unique test for US emergency departments, emergency physicians, emergency nurses and other stakeholders given its rarity in the US, high mortality rate, high risk of transmission to healthcare staff and non-specific presenting symptoms that can make initial diagnosis more difficult. However, as shown with other unanticipated infectious disease outbreaks (HIV, SARS, MERS), emergency departments will almost certainly be a key location for patient identification and treatment. The ethical concepts applied in this paper are relevant, especially reciprocity, duty to treat and grounding in the specific facts of the disease process in question, when considering how acute care facilities should prepare for likely future outbreaks of infectious disease. We propose that preparation for future emergency department responses to unanticipated infectious disease outbreaks should include ethical as well as logistical and medical factors.69 Given the multiple stakeholders represented in emergency department practice, the model shown here of multi-disciplinary and organizational consideration of the ethical issues involved would likely have application when considering the approach to future infectious disease challenges.
Conclusion
The outbreak of EVD in West Africa and the presentation of patients to US acute care facilities has raised a series of intertwined logistical and ethical issues of relevance to US emergency departments, emergency physicians and emergency nurses. While the current state of the epidemic has not led to a large number of EVD patients presenting to US facilities, consideration of ethical questions that are relevant now and of potential relevance in the future will allow emergency physicians, emergency nurses and other stakeholders to prepare appropriately for the challenges posed by Ebola and consider its implications for future epidemic infectious disease events. An emphasis on the principle of reciprocity, the obligations imposed by and underlying assumptions of the duty to treat and the specific characteristics of the disease process will aid in addressing the ethical challenges posed in the current outbreak of EVD.
Acknowledgments
The drafting authors wish to thank the ACEP Ebola Expert Panel and SAEM Global Academy of Emergency Medicine for their critical review of the manuscript during preparation and the leadership of ACEP, ENA and SAEM for their sponsorship of this effort.
References
1
Centers for Disease Control and Prevention
Ebola outbreak in West Africa—case counts
http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html (2014) Updated February 4, 2015. Accessed February 5, 2015
2
R Dunklin, S Thompson
ER doctor discusses role in Ebola patient’s initial misdiagnosis
Dallas Morning News (2014) http://www.dallasnews.com/ebola/headlines/20141206-er-doctor-discusses-role-in-ebola-patients-initial-misdiagnosis.ece, Accessed February 5, 2015
3
G Botelho, J Hanna, A Fantz
Nurse’s discharge leaves one Ebola case in U.S., though larger battle continues. CNN Web site
http://www.cnn.com/2014/10/28/health/us-ebola/ Accessed February 5, 2015
4
A Hartocollis, M Santora
Plenty of hugs as Craig Spencer, recovered New York Ebola patient, goes home
N Y Times (2014) http://www.nytimes.com/2014/11/12/nyregion/craig-spencer-new-york-ebola-patient-bellevue.html?_r=0, Accessed February 5, 2015
5
C Moskowitz
Are U.S. Hospitals Prepared for the Next Ebola Case?
Sci Am (2014) Available from: http://www.scientificamerican.com/article/are-us-hospitals-prepared-for-the-next-ebola-case/, Accessed February 5, 2015
6
A Soergel
Ebola quarantine questioned
US News and World Report (2014) http://www.usnews.com/news/newsgram/articles/2014/10/27/ebola-ethics-quarantine-questioned, Accessed February 5, 2015
7
American College of Emergency Physicians
Healthcare resources for suspected Ebola cases
http://www.acep.org/ebola/ Published 2014, Accessed February 5, 2015
8
Emergency Nurses Association
ENA topic brief: Ebola virus disease
http://www.ena.org/practice-research/Practice/Documents/EbolaTopicBrief.pdf Accessed February 5, 2015
9
Centers for Disease Control and Prevention
Ebola (Ebola virus disease)
http://www.cdc.gov/vhf/ebola/ Updated February 4, 2015, Accessed February 5, 2015
10
R Perl
Ebola response reveals double standard in U.S. health care
Forbes (2014) http://www.forbes.com/sites/robertpearl/2014/12/11/ebola-double-standard/, Accessed February 5, 2015
11
L Altman
Ethicist calls CPR too risky in Ebola
N Y Times (2014) http://www.nytimes.com/2014/10/21/health/-ethicist-calls-cpr-too-risky-in-ebola-.html, Accessed February 5, 2015
12
N Kass
Ebola, ethics, and public health: what next?
Ann Intern Med, 161 (10) (2014), pp. 744–745
Full Text via CrossRef | View Record in Scopus | Citing articles (13)
13
Toner E, Adalja A, Inglesby T. A primer on Ebola for clinicians published online ahead of print October 17, 2014. Disaster Med Public Health Prep.
14
G Donovan
Ebola, epidemics, and ethics—what we have learned
Philos Ethics Humanit Med, 9 (2014), p. 15
Full Text via CrossRef
15
K Koenig, C Majestic, M Burns
Ebola virus disease: essential public health principles for clinicians
West J Emerg Med, 15 (7) (2014), pp. 728–731
Full Text via CrossRef | View Record in Scopus | Citing articles (9)
16
L Meyers, T Frawley, S Goss, et al.
Ebola virus outbreak 2014: clinical review for emergency physicians
Ann Emerg Med, 65 (1) (2015), pp. 101–108
Article | PDF (1103 K)
| View Record in Scopus | Citing articles (14)
17
H Feldmann, T Geisbert
Ebola haemorrhagic fever
Lancet, 377 (9768) (2011), pp. 849–862
Article | PDF (2175 K)
| View Record in Scopus | Citing articles (429)
18
Centers for Disease Control and Prevention
Review of human-to-human transmission of Ebola virus
http://www.cdc.gov/vhf/ebola/transmission/human-transmission.html Updated October 29, 2014, Accessed February 5, 2015
19
L Sun, B Dennis
U.S. hospitals wary of caring for Ebola patients because of cost and stigma
The Washington Post (2014) http://www.washingtonpost.com/national/health-science/us-hospitals-wary-of-caring-for-ebola-patients-because-of-cost-and-stigma/2014/11/28/928aa2bc-71cc-11e4-893f-86bd390a3340_story.html, Accessed February 5, 2015
20
J Pines, R Mutter, M Zocchi
Variation in emergency department admission rates across the United States
Med Care Res Rev, 70 (2013), pp. 218–231
Full Text via CrossRef | View Record in Scopus | Citing articles (35)
21
Emergency Treatment and Active Labor Act (EMTALA), 42 USC §1395dd
(2008)
22
Center for Clinical Standards and Quality/Survey and Certification Group
Center for Medicare and Medicaid Services. Emergency Medical Treatment and Labor Act (EMTALA) requirements and implications related to Ebola virus disease (Ebola)
http://www.aha.org/content/14/141121-sc15-10emtala-ebola.pdf Published November 21, 2014. Accessed February 5, 2015
23
American College of Emergency Physicians
Code of ethics for emergency physicians
http://www.acep.org/Clinical—Practice-Management/Code-of-Ethics-for-Emergency-Physicians/ Accessed February 5, 2015
24
Emergency Nurses Association
ENA code of ethics
http://www.ena.org/about/ethics/Pages/Default.aspx Accessed February 5, 2015
25
Society for Academic Emergency Medicine
SAEM mission statement
http://www.saem.org/about-saem/mission Accessed February 5, 2015
26
American Medical Association
Opinion 9.067—Physician obligation in disaster preparedness and response
http://www.ama-assn.org.vlib.excelsior.edu/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion9067.page Accessed February 5, 2015
27
American Nurses Association
Code of ethics for nurses
http://www.nursingworld.org/codeofethics Accessed February 5, 2015
28
H Malm, T May, L Francis, et al.
Ethics, pandemics, and the duty to treat
Am J Bioeth, 8 (8) (2008), pp. 4–19
Full Text via CrossRef | View Record in Scopus | Citing articles (44)
29
A Zuger, S Miles
Physicians, AIDS, and occupational risk: historic traditions and ethical obligations
JAMA, 258 (14) (1987), pp. 1924–1928
Full Text via CrossRef | View Record in Scopus | Citing articles (110)
30
D Sokol
Virulent epidemics and scope of healthcare workers’ duty of care
Emerg Infect Dis, 12 (8) (2006), pp. 1238–1241
Full Text via CrossRef | View Record in Scopus | Citing articles (52)
31
W Austin
Ethics in a time of contagion: a relational perspective
Can J Nurs Res, 40 (4) (2008), pp. 10–24
View Record in Scopus | Citing articles (7)
32
World Health Organization
Statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa
http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/ Published August 8, 2014, Accessed February 5, 2015
33
Wildes R, Kayden S, Goralnick E, et al. Sign me up: rules of the road for humanitarian volunteers during the Ebola outbreak published online ahead of print October 24, 2014. Disaster Med Public Health Prep.
34
E Weiner
The nursing curriculum for emergency preparedness
http://www.nursing.vanderbilt.edu/advantage/emergency.html Accessed February 5, 2015
35
George Washington University School of Nursing
The National Nurse Emergency Preparedness Initiative (NNEPI)
http://nnepi.gwnursing.org/ Accessed February 5, 2015
36
Centers for Disease Control and Prevention
For general healthcare settings in West Africa: four keys to infection control
http://www.cdc.gov/vhf/ebola/hcp/international/keys-to-infection-control.html Updated December 19, 2014, Accessed February 5, 2015
37
M McCarthy
CDC rejects mandatory quarantine for travelers arriving from Ebola-stricken nations
BMJ, 349 (2014), p. g6499
Full Text via CrossRef | View Record in Scopus | Citing articles (3)
38
ACEP Ebola Expert Panel
Consensus statement on restrictive movement including quarantine of health care workers
http://www.acep.org/uploadedFiles/ACEP/practiceResources/issuesByCategory/publichealth/ACEP%20Ebola%20Expert%20Panel%20Consensus%20Statement.111314.pdf Published November 13, 2014, Accessed February 5, 2015
39
L Rosenbaum
License to Serve — U.S. Trainees and the Ebola Epidemic
New England Journal of Medicine, 372 (6) (2015), pp. 504–506
Full Text via CrossRef | View Record in Scopus | Citing articles (7)
40
Academic Consortium Combating Ebola in Liberia. http://accel.mit.edu/. Accessed December 30, 2014.
41
Centers for Disease Control and Prevention
Current Ebola Treatment Centers
http://www.cdc.gov/vhf/ebola/hcp/current-treatment-centers.html Accessed December 22, 2014
42
Centers for Disease Control and Prevention
Interim guidance for U.S. hospital preparedness for patients under investigation (PUIs) or with confirmed Ebola virus disease (EVD): a framework for a tiered approach
http://www.cdc.gov/vhf/ebola/hcp/us-hospital-preparedness.html Updated January 22, 2015, Accessed February 5, 2015
43
Accreditation Council for Graduate Medical Education
ACGME program requirements for graduate medical education in emergency medicine
https://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQ-PIF/110_emergency_medicine_07012013.pdf Published July 1, 2013, Accessed February 5, 2015
44
Accreditation Council for Graduate Medical Education
ACGME guidance statement on Ebola virus infection and resident/fellow training in the United States
https://www.acgme.org/acgmeweb/Portals/0/PDFs/Nasca-Community/ACGME-GME-Ebola-Final1.pdf Published October 2014, Accessed February 5, 2015
45
FL Counselman, MA Borenstein, CD Chisholm, et al.
The 2013 model of the clinical practice of emergency medicine
Acad Emerg Med, 21 (5) (2014), pp. 574–598
Full Text via CrossRef | View Record in Scopus | Citing articles (17)
46
R Bayer, GM Oppenheimer
AIDS Doctors: Voices From the Epidemic: An Oral History
Oxford University Press, Oxford, UK (2002)
47
JF Childress, RR Faden, RD Gaare, et al.
Public health ethics: mapping the terrain
J Law Med Ethics, 30 (2) (2002), pp. 170–178
Full Text via CrossRef | View Record in Scopus | Citing articles (257)
48
BBC News
Ebola: When health workers’ duty to treat is trumped
http://www.bbc.com/news/health-29573993 Published October 29, 2014, Accessed February 5, 2015
49
L Gruson
Montana nurses concerned about Ebola
Great Falls Tribune (2014) http://www.greatfallstribune.com/story/news/local/2014/10/15/montana-nurses-concerned-ebola/17340921/, Accessed February 5, 2015
50
J Schram, L Celona
Bellevue staffers call in “sick” after Ebola arrives
New York Post (2014) http://nypost.com/2014/10/25/many-bellevue-staffers-take-sick-day-in-ebola-panic/, Accessed February 5, 2015
51
Fox News
Hospital staffers reportedly take sick day rather than treat New York’s first Ebola patient
http://www.foxnews.com/health/2014/10/25/hospital-staffers-reportedly-take-sick-day-rather-than-treat-new-yorks-first/ Published October 25, 2014, Accessed February 5, 2015
52
K Qureshi
Health care workers’ ability and willingness to report to duty during catastrophic disasters
J Urban Health, 82 (3) (2005), pp. 378–388
Full Text via CrossRef | View Record in Scopus | Citing articles (184)
53
Payton v. Weaver, 131 Cal App 3d 38, 182 Cal Rptr 225 (Cal App 1 Dist 1982).
54
K Morin, D Higginson, M Goldrich
for the Council on Ethical and Judicial Affairs of the American Medical Association. Physician obligation in disaster preparedness and response
Camb Q Healthc Ethics, 15 (2006), pp. 417–421
View Record in Scopus | Citing articles (8)
55
P Singer, S Benatar, M Bernstein, et al.
Ethics and SARS: lessons from Toronto
BMJ, 327 (7427) (2003), p. 1342
Full Text via CrossRef | View Record in Scopus | Citing articles (90)
56
Center for Law and the Public’s Health
Model State Emergency Health Powers Act
http://www.publichealthlaw.net/MSEHPA/MSEHPA.pdf Accessed February 5, 2015
57
C Coleman, A Reis
Potential penalties for health care professionals who refuse to work during a pandemic
JAMA, 299 (2008), pp. 1471–1473
Full Text via CrossRef | View Record in Scopus | Citing articles (15)
58
E Pellegrino
Ethics and the moral center of the medical enterprise
Bull N Y Acad Med, 54 (7) (1978), p. 625
View Record in Scopus | Citing articles (3)
59
E Pellegrino
Toward a virtue-based normative ethics for the health professions
Kennedy Inst Ethics J, 5 (3) (1995), pp. 253–277
Full Text via CrossRef | View Record in Scopus | Citing articles (99)
60
M Meerschaert
Physicians’ duty to participate in pandemic care
JAMA, 300 (3) (2008), p. 284
Full Text via CrossRef | View Record in Scopus | Citing articles (2)
61
Koenig K. Ebola triage screening and public health: the new “vital sign zero” published online ahead of print October 29, 2014. Disaster Med Public Health Prep.
62
L Hawryluck, S Lapinsky, T Stewart
Clinical review: SARS–lessons in disaster management
Crit Care, 9 (4) (2005), p. 384
Full Text via CrossRef | View Record in Scopus | Citing articles (28)
63
C Irvin, L Cindrich, W Patterson, et al.
Survey of hospital healthcare personnel response during a potential avian influenza pandemic: will they come to work?
Prehosp Disaster Med, 23 (2008), pp. 328–335
Full Text via CrossRef | View Record in Scopus | Citing articles (56)
64
American Society of Anesthesiology
Recommendations from the ASA Ebola Workgroup
http://www.asahq.org/For-Members/Clinical-Information/Ebola-Information/Ebola-Guidelines-from-COH.aspx Accessed February 5, 2015
65
J Fins
Responding to Ebola: questions about resuscitation
http://www.thehastingscenter.org/Bioethicsforum/Post.aspx?id=7135&blogid=140 Published October 10, 2014, Accessed February 5, 2015
66
B Kreuels, D Wichmann, P Emmerich, et al.
A case of severe Ebola virus infection complicated by gram-negative septicemia
N Engl J Med, 37 (2014), pp. 2394–2401
Full Text via CrossRef | View Record in Scopus | Citing articles (106)
67
G Lyon, A Mehta, J Varkey, et al.
Clinical care of two patients with Ebola virus disease in the United States
N Engl J Med, 371 (2014), pp. 2402–2409
Full Text via CrossRef | View Record in Scopus | Citing articles (109)
68
J Rachels, S Rachels
The Idea of a Social Contract: The Elements of Moral Philosophy
(6th ed.)McGraw-Hill, Boston, MA (2010)
69
Institute of Medicine
Crisis Standards of Care: A Systems Framework for Catastrophic Disaster Response
National Academies of Science, Washington, DC (2012)
For correspondence, write: Arvind Venkat, MD, FACEP, Department of Emergency Medicine, Allegheny Health Network, 320 East North Avenue, Pittsburgh, PA 15212.
Vitae
Arvind Venkat (ACEP, SAEM), Department of Emergency Medicine, Allegheny Health Network, Pittsburgh, PA.
Lisa Wolf (ENA), Institute of Emergency Nursing Research, Des Plaines, IL.
Joel M. Geiderman (ACEP), Department of Emergency Medicine, Cedars-Sinai Medical Center, Los Angeles, CA.
Shellie L. Asher (SAEM), Department of Emergency Medicine, Albany Medical Center, Albany, NY.
Catherine A. Marco (ACEP), Department of Emergency Medicine, Boonshoft School of Medicine, Wright State University, Dayton, OH.
Jolion McGreevy (SAEM), Department of Emergency Medicine, Boston Medical Center, Boston University School of Medicine, Boston, MA.
Arthur R. Derse (ACEP), Center for Bioethics and Medical Humanities (Institute for Health and Society) and Department of Emergency Medicine, Medical College of Wisconsin, Milwaukee, WI.
Edward J. Otten (SAEM), Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH.
John E. Jesus (ACEP), Department of Emergency Medicine, Christiana Care Health System, Wilmington, DE.
Natalie P. Kreitzer (SAEM), Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH.
Monica Escalante (ENA), Institute for Quality, Safety and Injury Prevention, Des Plaines, IL.
Adam C. Levine (SAEM), Department of Emergency Medicine, Warren Alpert Medical School of Brown University, Providence, RI.
ED Ebola Triage Algorithm: A Tool and Process for Compliance
2015, Journal of Emergency Nursing
more
Nursing and complex humanitarian emergencies: Ebola is more than a disease
2015, Nursing Outlook
more
Arterial Blood Gas Review
2015, Journal of Emergency Nursing
more
View more articles »
Related book content
Ebola Virus Disease Patients Should not Receive CPR Sample Answer
In recent years, the healthcare sector emphasizes the importance of having practical and ethical considerations while handling various infectious diseases such as Ebola. There is various ethical consideration resulting from questions when it comes to offering critical care to patients. The main issues that result to the ethical obligations involve the treatment decisions regarding therapy limitations for EVD patients (Smeltzer et al, 2004). The circumstances under which the providers decline to care for the patient in consideration of whether it I ethically appropriate or not is an issue of concern. The vital ethical obligation while caring for EVD patients is that no individual is denied therapy and efforts should focus on preventing unnecessary risks. The ethical obligations require RN to adopt the right approaches facilitating ethically justifiable, evidence-based and rigorous decisions that are informed by nature. It is an ethical obligation for care providers to balance their roles to a patient who is highly infectious and their duty of self-protection (Smeltzer et al, 2004). There is an obligation that patients are provided with therapies that lead to the best outcomes and effective risk management. It is an obligation that strict protocols should not be breached while making decisions. It is an obligation for RN to adhere to protocols, e.g., ensuring the patient remains in the ultra-isolation during admission and imaging for patients is restricted. It is an ethical obligation to ensure consistency and transparency during processes of care which should be endorsed and evidence-based (Venkat et al, 2015).
The provision or withholding CPR to EVD patients in the critical stage is a factor of consideration in ethical practices while caring for patients. The balance of the RN responsibility for their well-being and personal safety while promoting the health of EVD patients is an ethical obligation emphasized (Venkat et al, 2015). Safer circumstances and environment should be the center focus by the RN while performing CPR procedures on the patients. The EVD patients deserve excellent health care from the RN. In a nutshell, transparency, adherence to ethical obligations and balanced health operations would result in positive impacts and desired outcomes.
Ebola Virus Disease Patients Should not Receive CPR References
Smeltzer, S. C., Bare, B. G., Hinkle, J. L., Cheever, K. H., Townsend, M. C., & Gould, B. (2004). Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 10th editions. Lippincott, Williams& Wilkins.
Venkat, A., Asher, S. L., Wolf, L., Geiderman, J. M., Marco, C. A., McGreevy, J., … & Escalante, M. (2015). Ethical issues in the response to Ebola virus disease in United States emergency departments: a position paper of the American College of Emergency Physicians, the Emergency Nurses Association, and the Society for Academic Emergency Medicine. Academic Emergency Medicine,
Diagnostic and Statistical Manual of Mental Disorders
This assignment will require you to develop a plan for your second major assignment in this course – the essay. You will need to select one essay topic from the list below, analyze it in terms of its key components, locate and read at least five relevant journal articles and then prepare an essay synopsis (essay plan). This plan will indicate how you will address the topic and what resources and information you will need to locate to address the topic. This assessment assesses Graduate Qualities 2 (lifelong learning), 3 (effective problem solver), and 6 (communicates effectively).
Essay Topics
Choose ONE of the five topics listed below. This is the topic you will also be writing your Essay (Assessment 2) on, so make sure you think carefully before making your decision.
1. Describe the trait theory of personality. Select one “factor” or “trait” from a prominent trait theory and discuss the relative strengths and weaknesses of someone who strongly exhibits this trait.
2. Jean Piaget proposed a step-wise sequence of mental development during childhood. Provide an overview of Piaget’s core ideas, discussing the evidence for and against these ideas.
3. Discuss the factors that affect the likelihood that people will engage in prosocial behavior. What is the evidence for these effects, and how might changes in our society affect the likelihood of people acting pro-socially?
4. Describe the main social factors that influence attraction between people. Select one of these factors and describe the empirical support for its influence.
5. Select a psychological disorder that features in the current version of the Diagnostic and Statistical Manual of Mental Disorders. Describe this disorder, providing evidence for the major contributing factors to the onset of the disorder.
Diagnostic and Statistical Manual of Mental Disorders Presentation
Your work must be word-processed, font size 12, with a 3cm margin and with double-line spacing. American Psychological Association (APA; 5th edition or later) referencing conventions must be strictly adhered to both in the body of the synopsis for in-text citations and in the Reference List at the end of the synopsis. The recommended writing guide contains important information on APA style referencing & citation as well as how to prepare and present an essay.
The Essay Synopsis will be given a mark out of 15% of the total course grade, and you will be graded on the following criteria:
1. Topic analysis
2. Coherence and structure of the plan
3. Clarity of expression
4. Adherence to word length (800 words)
5. Relevance of references
Note: A copy of the Feedback Form that will be used to help grade your work for the Essay Synopsis will be posted on the course website.
***More detailed information, including examples, will be provided in class***
Assessment 1 – Essay synopsis
This assignment will require you to develop a plan for your second major assignment in this course – an essay. You will need to select your essay topic from the list below, analyze it in terms of its key components, locate and read at least five relevant peer-reviewed journal articles and then prepare an essay synopsis (essay plan). This plan will indicate how you will address the topic and what resources and information you will need to locate to address the topic.
Essay Topics
Choose ONE of the five topics listed below. This is the topic you will be writing your Essay (Assessment 2) on so make sure you think about it carefully before making your decision.
1. Describe the trait theory of personality. Select one “factor” or “trait” from a prominent trait theory and discuss the relative strengths and weaknesses of someone who strongly exhibits this trait.
2. Jean Piaget proposed a step-wise sequence of mental development during childhood. Provide an overview of Piaget’s core ideas, discussing the evidence for and against these ideas.
3. Discuss the factors that affect the likelihood that people will engage in prosocial behavior. What is the evidence for these effects, and how might changes in our society affect the likelihood of people acting pro-socially?
4. Describe the main social factors that influence attraction between people. Select one of these factors and describe the empirical support for its influence.
5. Select a psychological disorder that features in the current version of the Diagnostic and Statistical Manual of Mental Disorders. Describe this disorder, providing evidence for the major contributing factors to the onset of the disorder.
Presentation
Your work must be word-processed, font size 12, with a 3cm margin and with double-line spacing. American Psychological Association (APA; 5th edition or later) referencing conventions must be strictly adhered to both in the body of the synopsis for in-text citations and in the Reference List at the end of the synopsis. The recommended writing guide contains important information on APA style referencing & citation as well as how to prepare and present an essay.
The Essay Synopsis will be given a mark out of 15% of the total course grade, and you will be graded on the following criteria:
1. Topic analysis
2. Coherence and structure of the plan
3. Clarity of expression
4. Adherence to word length (800 words)
5. Relevance of references
Note: A copy of the Feedback Form that will be used to help grade your work for the Essay Synopsis will be posted on the course website.
Diagnostic and Statistical Manual of Mental Disorders Sample Answer
The main social factors that influence attraction between people include; people’s perception of their own attractiveness, beauty, similarity and re, reciprocity. The perception of a people about their attractiveness is also referred to as self esteem (Brown, 2014). Beauty is a contributor to attraction between people. This quality of people makes them feel the ease and urge to meet and socialize on many levels (McGinley, et al., 2015). This is why it is important to have such proximity between people who are attracted to one another (Brown, 2014).
Beauty is defined as the experience of pleasure or satisfaction based on perception. That is why beauty can only be seen and not felt (Weidenfeld & Leask, 2013). What people see as beautiful is often a creation of their social setting. It is a form of influence that ends up making the person to feel that what they see as beautiful is not as beautiful or appealing as they suppose. Beauty is thus a form of influence that is borne out of what the society considers to be appealing or not. Beauty is however the greatest contributor to perceptions about attraction (Launay & Dunbar, 2015). Where there is an attraction, beauty is often a factor that is critical and central to the theme.
Beauty is about the traits that make one seem to have a beautiful character and to some extent, beautiful build and look. It applies to both persons of the male and those of the female gender (Talamas, Mavor & Perrett, 2016). Despite the variations in perception across various cultures, beauty remains to be one of the most influential factors in establishing attraction between people. In such a case, beauty becomes defined by the intrinsic features that a person possesses and not their outward appearances (Launay & Dunbar, 2015).
There are various stereotypes that are related to beauty. Most people tend to think that people naturally get attracted to those individuals whom they have certain common features with (McGinley, et al., 2015). This stereotyping concept involves both men and female, and in this example, the proponents of this belief argue that the existing high number of integration, interaction, marriage, and business establishments between people of the same ethnicity proves that people get attracted to others whom they share a certain common (Brown, 2014). In other words, one does not need to be beautiful or to possess certain features for them to be loved by another individual.
There are two major forms of beauty that are in existent at the moment. These are; augmented beauty and natural beauty. Whereas naturally beauty is acquired naturally and one may possess it from the time they are born, augmented beauty is acquired artificially (Diessner, et.al, 2012). To acquire augmented beauty, a person uses various artificial beauty products and solutions to enhance their appearance by becoming more beautiful than they were previously (Launay & Dunbar, 2015). Even though both these two types of beauty make one attractive, there are various concerns about the longevity of augmented beauty.
Vacker & Key (2013) argue that beauty only causes short-term attraction. Similarity in people’s perception of beauty is really what matters. It is the views they hold about a beautiful place, beautiful hoses, activities and people that male them attracted to one another for long (Vacker & Key, 2013). Similarity is the state of resemblance between entities. (Mitteness, et al., 2016). When people share similar feelings, they have a likeness for same places, beliefs, tangible things and approaches to life (Mitteness, et al., 2016). Similarity is one aspect that traverses all other concepts in attraction because there is a significant relationship between the concept of beauty, perception of attractiveness and reciprocity on similarity. Each concept requires that there be another person sharing a similar opinion as another before a bond can be established (Brown, 2014). This unites the people on a common ideology or belief.
The importance of being beautiful creates the need for one to put in the effort so as to become beautiful (Talamas, Mavor, &Perrett, 2016). This is because, without beauty, a person may not be attractive to others. As a result, they may end up feeling dejected and living a lonely life. Since human beings are social species, it is wise to put in an effort to enhance beauty so as to live a comfortable and soothing life with many admirers as compared to living unfulfilling life as a result of lowbeauty levels (Weidenfeld & Leask, 2013). Therefore, as Englis, Solomon and Ashmore (2014) argue, that it is more sensible to put in the effort so as to improve a person’s beauty as compared to leaving it the way it is and undergoing a tough social life.
Many people consider the feeling of attraction to be related to the symmetrical shape of the person, shape or thing. Many people are attracted to beauty and not value. There is thus the general feeling that most human beings will often proverbially ‘read a book by its cover.’ This is a concern among persons who mask their attractive qualities by not being very outgoing and expressive about their characters.
Diagnostic and Statistical Manual of Mental Disorders References
Brown, J. D. (2014). Self-esteem and self-evaluation: Feeling believes. Psychological perspectives on the self, 4, 27-58.
Diessner, R., Solom, R. C., Frost, N. K., Parsons, L., & Davidson, J. (2012).Engagement with beauty: Appreciating natural, artistic, and moral beauty.The Journal of Psychology, 142(3), 303-29. Retrieved from http://search.proquest.com/docview/213828232?accountid=45049.
Englis, B. G., Solomon, M. R., &Ashmore, R. D. (2014). Beauty before the eyes of beholders: The cultural encoding of beauty types in magazine advertising and music television.Journal of Advertising, 23(2), 49. Retrieved from http://search.proquest.com/docview/236550542?accountid=45049
Launay, J., & Dunbar, R. M. (2015). Playing with Strangers: Which Shared Traits Attract Us Most to New People?. Plos ONE, 10(6), 1-17.doi:10.1371/journal.pone.0129688
McGinley, S., Zhang, L., Mattila, A., & O’Neill, J. (2015). Attraction to Hospitality Companies: How Processing Fluency Moderates Value Fit. Journal Of Human Resources In Hospitality & Tourism, 14(1), 25-44.doi:10.1080/15332845.2014.904171
Mitteness, C. R., DeJordy, R., Ahuja, M. K., &Sudek, R. (2016). Extending the Role of Similarity Attraction in Friendship and Advice Networks in Angel Groups. Entrepreneurship: Theory & Practice, 40(3), 627-655. doi:10.1111/etap.12135
Talamas, S. N., Mavor, K. I., &Perrett, D. I. (2016). Blinded by Beauty: Attractiveness Bias and Accurate Perceptions of Academic Performance. Plos ONE, 11(2), 1-18.doi:10.1371/journal.pone.0148284
Vacker, B., & Key, W. R. (2013). Beauty and the beholder: The pursuit of beauty through commodities.Psychology & Marketing (1986-1998), 10(6), 471. Retrieved from http://search.proquest.com/docview/230393591?accountid=45049
Weidenfeld, A., &Leask, A. (2013). Exploring the relationship between visitor attractions and events: definitions and management factors. Current Issues In Tourism, 16(6), 552-569. doi:10.1080/13683500.2012.702736
In this assignment we are going to look at Mrs Gwendolyn Harris. Mrs Gwendolyn Harris is an 82 year old war widow who has presented to the nurse practitioner wound management clinic after being referred by her GP Dr Greenwood. Six weeks ago she was scratched on the lower right leg by her cat Whiskers. The wound has not healed well. She has had increasing pain over the past six weeks which has been relieved to some degree after her daughter advised her to elevate her leg in the evenings. She has also been applying a small crepe bandage, which she has been washing every other day, to her lower leg daily to reduce the exudate soiling her clothes. Julia (the daughter) drives her mother to the vascular nurse practitioner (VNP) clinic. He reviews her bilateral Doppler ultrasound and bilateral ankle brachial pressure index (ABPI) results which confirm R) lower leg venous insufficiency and deep venous disease.
Mrs Gwendolyn has a Past medical history of ;Congestive cardiac failure (CCF), bilateral leg varicose veins, R) leg deep vein thrombosis (DVT) five years ago, gastrointestinal bleed (GI) bleed 10 years ago
She has a Past surgical history of; Cholecystectomy 40 years ago
Her Past family history include ;Sister, Jessie (deceased), cardiovascular disease (CVD), macular degeneration.
She is Allergic to Penicillin, Voltaren
In this assignment we are to discuss in-depth the pathophysiology of Gwendolyn’s condition firstly, therefore pathophysiology of pain and wound healing. We are then to identify objective and subjective data & formulate relevant actual or potential four (4) nursing issues based on the data presented in the scenario. The four (4) nursing issues identified for Gwendolyn are;
1) Chronic wound healing
2) Chronic pain
3) Poor eyesight
4) Hearing loss.
For each of the nursing issues identified above, we are to provide a brief pathophysiology for each one, provide excellent understanding of current evidence based practice and patient centred care. We are also to discuss the inter-professional roles likely involved, discuss/link pharmacology (Macuvision for her poor eyesight, antibiotics for her wounds and chronic pain management medication like Metronidazole, Ciprofloxacin), discuss lifespan issues (how her age can affect wound healing, Poor eyesight and hearing loss because of her age), discuss also briefly her psychosocial issues (she is a 82 yr. old widow living independently) This should be included for each of the nursing issues. We should demonstrate clear links between these concepts and the case scenario and nursing practice.
SAMPLE ANSWER
Pain has a warning damage as well as a protective function in nature, which calls for adequate medication and treatment of the affected areas as in the case of Mrs. Gwendolyn. Wounds resulting to pain is identified to have failed to heal in an orderly reparative process. The wounds lead to poor functional, and anatomy integrity due to pain that follows. Pain influences poor perfusion and low oxygen tension reduces the rate of collagen deposition in the tissues. Consequently, vasoconstriction follows due to severe pain which also impairs the healing of wounds. Infection, ischemia, nerve damage or the severe injury on the skin are the major causes of wound pain similar to the case of Mrs. Gwendolyn. The decrease of oxygen in the tissues results to production of low leucocytes which causes infection as the bacteria is given a chance to colonize the wound (Robb, 2016, pg. 56). In this case, the patient suffers severe pain and makes the healing process of the wound cumbersome. However, pain is identified to be a personal thing that is dependent on what the patient would express.
Etiology and pathology of pain dictate the sort of pain experienced by the patients. In this case, Mrs. Gwendolyn suffers from severe pain since the deep venous disease is a peripheral vascular problem which affects the healing process (Roberts et al, 2016, pg. 88). The deep venous disease in the patient also causes the venous ulcers which need to be addressed carefully through the right treatment and management strategies. Provision of a moist wound environment, compression therapy necrotic tissues’ debriment is essential during the pain and wound healing process of a patient (Bester & Van, 2015, pg. 79).
Patients with chronic wounds require quick management to prevent its progression to fatal stages causing severe pain. The accurate assessment of the patient’s pain progression is vital before the adoption of treatment strategies for chronic wounds. Venous insufficiency as identified in Mrs. Gwendolyn is one of the major causes that leads to the progression of wounds to be chronic. Other factors include arterial perfusion, unrelieved pressure, and immunosuppression. The chronic wound healing issue as identified is affected by many systematic and local factors (Robb, 2016, pg. 105). Age factor affects wound healing. The altered inflammatory process is related to impaired healing of chronic wounds among the elderly. Delayed infiltration of T-cell and chemokine production influence the delayed healing of chronic wounds among the elderly. Exercise is proved to enhance faster wound healing among the elderly. Elimination of the noxious stimuli and identifying the underlying cause is crucial while managing the chronic wound issues. Chronic wounds healing is closely associated with the high intensity of the acute postoperative pain.
It is essential to follow the patient centered care and evidence-based practices while treating patients with chronic wounds. While addressing chronic wound healing complications, there are various elements identified using TIME mnemonic device (Mehmood et al, 2015, pg. 112). The device is set to identify elements of chronic wound healing impairment. These elements include tissue surrounding the wound, infection or inflammation, moisture balance and edges blood supply. Preserving vital tissue is essential as there are many impediments that hinder optimal healing. Sharp debridement as an effective evidence-based practice used in the treatment of chronic wounds arising from venous related ulceration such as the patient in our case study. Topical antibiotics such as Vitamin A& D ointments, antacids, regranex, and collagen are used to enhance the faster and more efficient healing of chronic wounds (Mehmood et al, 2015, pg. 60). Silver-containing dressings are used in improving the healing rates for wounds. Nurses and other medical practitioners are supposed to treat the patient through proper dressing of wounds, enhancing adequate nutrition, ensuring proper tissue oxygenation as well as treating underlying infections. It is the role of the nurse to follow-up even after debriment and treatment of infections to ensure wound care is efficient to control chronic contamination of the wound (Rhee et al, 2015, pg. 109).
It is the professional role of nurses to provide wound management education and training to patients and their family members. Such measures and practices have been seen to improve the efficacy and quality of the treatment strategies used thus preventing the complication of situations. Optimal care should be provided to the patients, especially the elderly who have numerous cases of malnutrition which affects their wound healing process (Hosseini et al, 2016, pg. 93). The collaboration between the physician and patient enhances the better management of the chronic wounds.
The chronic pain is another nursing issue identified and requiring the quick address to prevents further complications experienced by the patient. The initiating causes and the patient’s threshold for pain is used in differentiating whether the pain is chronic or not. Multiple neurobiological mechanisms are said to contribute to pain making its categorization cumbersome (Lee et al, 2014, pg. 156). Nevertheless, some of the most common types of pain include nociceptive pain, central pain augmentation, and inflammatory pain. Aberrant somatosensory processing which occurs in the central nervous system is used to explain the chronic pain. Inflammation or damage to the tissue sensitizes nociceptors which are the nerve ending transmitting signals of pain in the nervous system (Scherer et al, 2016, pg. 112). Chronic pain is identified to be a persistent maladaptive response where psychological comorbidities are common.
Better pain management is made possible through adherence to the right evidence-based practices as well as the provision of patient-centered care to the patient. Such strategies would include understanding the pathophysiology of chronic pain appropriately before the administration of management strategies. Interventional and behavioral therapy should be combined as practices by the nurses while offering professional assistance to patients experiencing chronic pain (Fox et al, 2016, pg. 145). Full involvement of the family members and the patient would ensure they also contribute to making of clinical decisions towards their treatment making management of situations such as chronic pain more efficient in nature. Rehabilitation practices such as occupational, physical and cognitive therapy are used in the management of chronic pain reducing medication needs (Lukewich et al, 2015, pg. 92). Various drugs such as simple analgesics, opioid, and tricyclic antidepressants are used as the medication for treating patients with chronic pain (Scherer et al, 2016, pg. 156). It is the role of the nurse to offer proper clinical guidance to the patient as well as the prescriptions of drugs. Anti-inflammatory drugs are used in the management of pain among patients. Other medication drugs include ciprofloxacin and metronidazole (Patel et al, 2016, pg. 135).
The inter-professional role of the nurse ensures that approach of pain management is organized in nature. The approach entails, routine chronic pain evaluation, encouraging patients to share their chronic pain experiences, adopting evidence-based practices during treatment as well as selective modification of opioid regulatory policies and practices. Adherence to Consistent pain management strategies and minimizing pain is the major role performed by those caring for the patient. The psychosocial issues should be handled effectively; it is most likely that the woman feels lonely which might also affect her recovery process (Rommem et al, 2015, pg. 137). It is essential to administer therapies and advice that a person is attached to the patient to offer her necessary support. Nurse Follow-up of her medication and treatment, while she is at home, would help alleviate the psychosocial issues that could affect her recovery.
Poor eyesight is another nursing issue identified and requires proper management. Poor eyesight causes people to have a blurry vision which makes various objects appear hazy or seems to be out of focus. Some of the poor eyesight problems include astigmatism, refractory errors and also presbyopia (Waldron, 2012, pg. 43). A comprehensive eye assessments such as Snellen eye chart and the spatial contrast sensitivity test would be helpful in identifying the particular eyesight problem. Age has been consistently identified as a factor influencing poor eyesight among patients (Wadlron, 2012, pg. 64). There is macular degeneration which is age-related and leads to blurry vision and gradual loss of vision. The elderly also experience distortions which can lead to blindness at the end. The patient in our cases study has a family history of macular degeneration which can be a cause of her poor eyesight problems due to genetic factors. Through macular degeneration, the central vision would become blurred due to damage of macula. Age is a major contributing factor since most people suffering from poor eyesight problems are above the age of 65years while the risk rises with the increase in age (Dutta et al, 2015, pg. 117). Other than macular degeneration vision impairment in the elderly patient would result due to cataract and glaucoma.
Treatment and management of poor eyesight problems to prevent the progression to severe stages is essential when caring for the patients. The diagnosis of poor eyesight problem should be done correctly before undertaking any treatment strategies. Treatment is dependent on specific causes. Psychosocial reasons such as stress and loneliness might hinder the patient from taking care of herself well even to follow the diet that helps improve eyesight (Willis et al, 2016, pg. 138). In this case, it is vital to have a caregiver who is there almost all times. Alterations in vision, especially among the old, is detected using Amsler grid (Simsek et al, 2015, pg. 143). To reduce the risks of suffering from the age-related macular degeneration (AMD), intake of foods with high levels of carotenoids is useful. Foods rich in zeaxanthin and lutein are also required to solve the problem. Mineral supplements and antioxidant vitamin are offered to the patient to manage the situation (Sismek et al, 2015, pg. 73). Complete blindness is not related to AMD, thus the management of poor eyesight is easier. Radiation therapy and provision antiangiogenic drugs are recommended among the evidence-based practices to manage poor eyesight.
Hearing loss results from poor or lack of sound transmission to the cochlea. Hearing loss is usually categorized into various levels such as slight, mild, moderate, severe and profound hearing losses. Presbycusis is one of an age-related hearing loss problem which is experienced among the elderly people like Mrs. Gwendolyn (Werfel et al, 2016, pg. 75). The hearing loss gradually progresses as one gets old with time. Equal effects are experienced in both ears when one is affected by the problem. Past medications toxic to ensory cells, past medical conditions such as hypertension or chemotherapy drugs influence hearing loss among elderly people. Hearing loss affect the functioning of the tympanic membrane (Schlauch et al, 2015, pg. 83).
It is the professional role to involve the patient and the family actively in training and educating about hearing loss. Referral of patients to special programs or audiologist to assist in improving auditory reception is important. Social workers can also be assigned to those who already suffer from hearing loss to assist them in their daily activities since elderly people have psychosocial problems which call for the caregiver to be present (Rudner et al, 2016, p.g 70). The management and provision of patient-centered care are essential for the elderly patient during prevention or treatment of the problem (Van et al, 2016, p.g 112).
References List
Bester, P, & Van Deventer, Y 2015, ‘Holistic care for patients living with chronic wounds’, Wound Healing Southern Africa, 8, 2, pp. 78-81, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Dutta, S, Caplan, D, & Marcinko, D 2014, ‘Blurred Vision, Perilous Future: Management Fraud at Olympus’, Issues In Accounting Education, 29, 3, pp. 459-480, Business Source Complete, EBSCOhost, viewed 3 August 2016.
Fox, L, Walsh, J, Morrison, T, O’ Gorman, D, Ruane, N, Mitchell, C, Carey, J, Coughlan, R, & McGuire, B 2016, ‘Cognitive Coping Style and the Effectiveness of Distraction or Sensation-Focused Instructions in Chronic Pain Patients’, Plos ONE, 11, 4, pp. 1-12, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Hosseini, S, Idani, I, Rashidi, S, & Yadollahpour, A 2016, ‘Ultrasound based techniques for treatment of chronic Wounds: A comprehensive review of therapeutic efficacies and clinical considerations’, International Journal Of Pharmaceutical Research & Allied Sciences, 5, 2, pp. 387-397, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Lee, C, Crawford, C, Teo, L, & Spevak, C 2014, ‘An Analysis of the Various Chronic Pain Conditions Captured in a Systematic Review of Active Self-Care Complementary and Integrative Medicine Therapies for the Management of Chronic Pain Symptoms’, Pain Medicine, 15, pp. S96-S103, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Lukewich, J, Mann, E, VanDenKerkhof, E, & Tranmer, J 2015, ‘Self-management support for chronic pain in primary care: a cross-sectional study of patient experiences and nursing roles’, Journal Of Advanced Nursing, 71, 11, pp. 2551-2562, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Mehmood, N, Hariz, A, Templeton, S, & Voelcker, N 2015, ‘A flexible and low power telemetric sensing and monitoring system for chronic wound diagnostics’, Biomedical Engineering Online, 14, 1, pp. 1-17, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Patel, T, Chang, F, Mohammed, H, Raman-Wilms, L, Jurcic, J, Khan, A, & Sproule, B 2016, ‘Knowledge, Perceptions and Attitudes toward Chronic Pain and Its Management: A Cross-Sectional Survey of Frontline Pharmacists in Ontario, Canada’, Plos ONE, 11, 6, pp. 1-14, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Rhee, S, Valle, M, Wilson, L, Lazarus, G, Zenilman, J, & Robinson, K 2015, ‘Negative pressure wound therapy technologies for chronic wound care in the home setting: A systematic review’, Wound Repair & Regeneration, 23, 4, pp. 506-517, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Robb, C 2016, ‘Chronic wound management’, Chemist & Druggist, 284, 6965, pp. 12-14, Business Source Complete, EBSCOhost, viewed 3 August 2016.
Roberts-Turner, R 2016, ‘Quality Improvement. Pain Management: An Evidence-Based Approach’, Pediatric Nursing, 42, 1, pp. 39-49, Professional Development Collection, EBSCOhost, viewed 3 August 2016.
Romem, A, Tom, S, Beauchene, M, Babington, L, Scharf, S, & Romem, A 2015, ‘Pain management at the end of life: A comparative study of cancer, dementia, and chronic obstructive pulmonary disease patients’, Palliative Medicine, 29, 5, pp. 464-469, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Rudner, M, Mishra, S, Stenfelt, S, Lunner, T, & Rönnberg, J 2016, ‘Seeing the Talker’s Face Improves Free Recall of Speech for Young Adults With Normal Hearing but Not Older Adults With Hearing Loss’, Journal Of Speech, Language & Hearing Research, 59, 3, pp. 590-599, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Scherer, M, Hansen, H, Gensichen, J, Mergenthal, K, Riedel-Heller, S, Weyerer, S, Maier, W, Fuchs, A, Bickel, H, Schön, G, Wiese, B, König, H, van den Bussche, H, & Schäfer, I 2016, ‘Association between multimorbidity patterns and chronic pain in elderly primary care patients: a cross-sectional observational study’, BMC Family Practice, 17, pp. 1-8, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Schlauch, R, Koerner, T, & Marshall, L 2015, ‘Effective Identification of Functional Hearing Loss Using Behavioral Threshold Measures’, Journal Of Speech, Language & Hearing Research, 58, 2, pp. 453-465, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Şimşek, Y, Şenol, S, Canöz, Ö, Selçuklu, A, Diri, H, & Keleştimur, F 2015, ‘A Case of Pituicytoma Presenting with Blurred Vision and Hormone Deficiency’, Turkish Journal Of Endocrinology & Metabolism, 19, 3, pp. 115-118, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Van Eynde, C, Swillen, A, Lambeens, E, Verhaert, N, Desloovere, C, Luts, H, Vander Poorten, V, Devriendt, K, & Hens, G 2016, ‘Prevalence and Nature of Hearing Loss in 22q11.2 Deletion Syndrome’, Journal Of Speech, Language & Hearing Research, 59, 3, pp. 583-589, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
Waldron, J 2012, ‘Talking labels boost compliance in patients with poor eyesight’, Chemist & Druggist, 278, 6834, p. 11, Business Source Complete, EBSCOhost, viewed 3 August 2016.
Werfel, K, & Hendricks, A 2016, ‘Identifying Minimal Hearing Loss and Managing Its Effects on Literacy Learning’, Teaching Exceptional Children, 48, 4, pp. 213-217, Professional Development Collection, EBSCOhost, viewed 3 August 2016.
Willis, J, & Ramulu, P 2016, ‘Poor Vision and Self-Reported Functional Difficulties among Recently Hospitalized Individuals in the United States’, Ophthalmic Epidemiology, 23, 3, pp. 154-161, Academic Search Premier, EBSCOhost, viewed 3 August 2016.
We can write this or a similar paper for you! Simply fill the order form!
Here are the most essential part of the instructions:
Summary
For each source listed, begin with a summary of the information you found in that specific source. The summary section gives your reader an overview of the important information from that source. Remember that you are focusing on a source’s method and results, not paraphrasing the article’s argument or evidence.
The questions below can help produce an appropriate, scholarly summary:
What is the topic of the source?
What actions did the author perform within the study and why?
What were the methods of the author?
What was the theoretical basis for the study?
What were the conclusions of the study?
Critique
After each summary,
?the?
annotations should include a critique or analysis of each source. In this section, focus on the strengths of the article or the study (the things that would make your reader want to read this source), but do not be afraid to address any deficiencies or areas that need improvement. The idea of a critique is that you act as a critic—addressing both the good and the bad.
In
?the?
critique/analysis, answer ?as many?
of the following questions? as possible?
:
Was the research question well framed and significant?
How well did the authors relate the research question to the existing body of knowledge?
Did the article make an original contribution to the existing body of knowledge?
Was the theoretical framework for the study adequate and appropriate?
Has the researcher communicated clearly and fully?
Was the research method appropriate?
Is there a better way to find answers to the research question?
Was the sample size sufficient?
Were there adequate controls for researcher bias?
Is the research replicable?
What were the limitations in this study?
How generalizable are the findings?
Are the conclusions justified by the results?
Did the writer take into account differing social and cultural contexts?
Application
The last part of each annotation should justify the source’s use? (why did we choose this source)?
and address how the source might fit into ?my
research. Consider a few questions:
How is this source different than others in the same field or on the same topic?
How does this source inform your future research?
Does this article fill a gap in the literature?
How would you be able to apply this method to your area of focus or project?
Is the article universal?
?PLEASE NOTE THAT IF YOU CAN SUGGEST DIFFERENT ARTICLES THAT WOULD FIT THE RESEARCH BETTER, I AM OPEN TO THAT.
My research is autism topic is caring for an autistic child. I have close relatives in my family who are raising a 5 year old autistic child. The goal is to help the parents raise their son most successfully.
Basics of Synthesis
As you incorporate published writing into your own writing, you should aim for synthesis of the material. Read the following pages for more help on synthesis.
Synthesizing means comparing different material and highlighting similarities, differences, and connections. When a writer synthesizes successfully, he or she presents new ideas based on interpretations of other evidence or arguments. Critical reading and critical thinking are key components of successful synthesizing.
Please feel free to ask me for any clarifications.
SAMPLE ANSWER
Annotated Bibliography
Caring for Autistic Individuals
Johnson, B. P., Papadopoulos, N., Fielding, J., Tonge, B., Phillips, J. G., & Rinehart, N. J. (2013). A quantitative comparison of handwriting in children with high-functioning autism and attention deficit hyperactivity disorder. Research in Autism Spectrum Disorders, 7(12), 1638-1646.
This article focused on establishing the difference in handwriting between children suffering from attention deficit hyper- reactivity disorder (ADHD) and those with high- functioning autism (HFA) to establish the effects of this disorders in academic welfare of the children. The author achieved this by having children duplicate words cat and dog repeatedly paying attention to space, size errors and speed. The study involved 49 participants all boys between ages of 7 and 14 years who had to complete the handwriting performance test (HPT). The base of this study is to illustrate how HFA and ADHD affect children in their academics limiting their expression through writing. The findings of this task indicate the existence of writing impairments in these children, and therefore there need tailored writing therapies. As it has been found in other studies, ADHD and HFA significantly affects the writing speed of the individuals. However, it has been found that other factors contribute to the lower writing speed. The study is limited in that the sample size was small.
The findings are applicable for caregivers especially teachers who care for autistic children. As such, the teachers can be able to apply different teaching methods with these children. Since the article explains the differences in factors that contribute to slow handwriting in children with ADHD and HFA, teachers are enlightened on how to how children with different disorders differently.
Kreider, C. M., Bendixen, R. M., Mann, W. C., Young, M. E., & McCarty, C. (2015). Mixed-method exploration of social network links to participation. OTJR: occupation, participation and health, 1539449215578650.
This article discusses the importance of Social Networks (SNs), and how this network affects the participation of youths especial those with Attention Deficit Hyper- Reactivity Disorder (ADHD),Learning Disorder (LD), and Autism Spectrum Disorder (ASD). The participants were interviewed individually, and the author performed personal link investigation to determine their level of participation. The method used was a combination of both qualitative and quantitative analysis blended in a mixed method design. This exercise was based on assessing the relationship between SN and participation and how these disorders affect the participation of youths. The findings of this study point out the communication impairments in individuals with these disorders. This, therefore, indicates the need to encourage the youths to participate more in social interactions to enhance their social skills. This reading has focused on the role of peers, family members and other acquaintances that comprise the SNs of these individuals in promoting their participation. The study is limited in that it lacked online participations. In addition, the sample was small, and only a few participants have complex cognitive disorders.
It is, however, beneficial to parents, friends and other family members interacting with youth with any of the disorders. Therefore, it is important for family members and friends to encourage the participation of these youths in different social activities. The study indicates that some of these individuals do not make much sense during the conversations; however, friends and relatives should not shun or discourage them. What they need is encouragement and be treated like normal persons in case of such incidents.
Heyvaert, M., Saenen, L., Campbell, J. M., Maes, B., & Onghena, P. (2014). Efficacy of behavioral interventions for reducing problem behavior in persons with autism: An updated quantitative synthesis of single-subject research. Research in developmental disabilities, 35(10), 2463-2476.
In this paper, the writer evaluates essence of behavioral interventions in eradicating the problem behavior in individuals diagnosed with autism. To come up with relevant information, the author conducted searches from journals, bibliographies, and databases. The analysis was then done to align the various sources of original studies. The method applied was a quantitative blend of mono subject studies comprising of 213 sources representing 358 individuals with autism. This study is based on the numerous problems that originate from autism and how their impacts can be reduced. The results indicate that behavioral interventions are effective in reduction of these problems; however, some are better than others are. This study has managed to cover most of the details concerning different behavioral interventions and how they can be employed to cater for problems resulting from autism. As such, it is a good piece for caregivers of individuals with challenging behaviors because of autism.
The different behavioral interventions that are described by the author of this article can be applied by parents and caregivers to handle different challenging behaviors portrayed by individuals with these disorders. This article provides crucial information for these caregivers because some of the challenging behaviors can have detrimental effects to these individuals their siblings or the caregivers. For instance self-injury behaviors can be managed through stories talks or combined therapy that has been proved efficient.
Hebron, J., Humphrey, N., & Oldfield, J. (2015). Vulnerability to bullying of children with autism spectrum conditions in mainstream education: a multi‐informant qualitative exploration. Journal of Research in Special Educational Needs, 15(3), 185-193.
This paper lays focus on how autism results in bullying of affected children in schools, and how this bullying affects them as well as how it should be handled. The author conducted interviews with five children with autism aged between 5-13 years, their parents as well as teachers. The method put into practice by the author is a cross-sectional qualitative analysis with semi-structured interviews for data gathering. The base of this study is the rampant cases of bullying of children with autism raising a lot of concern. The study concluded that bullying in schools is a serious problem for children with autism hence affecting their peer relationships. This creates the need for school staff to create a strong protective role for these children. As such, teachers should build a good relationship with these children to encourage communication and hence reduce the bullying risk. The limitation of this study is that the size of the sample is very small. However, the author has managed to cover principal areas such as the role of parents, teachers, and the entire school in the reduction of the bullying risk.
This study helps the caregivers on the signs to look out for to detect bullying and the actions to take in case of an incident. It also explains the role of teachers and parents in containing bullying. The article also describes how teachers can discourage bullying through punishment of the culprits. It also explains how children who have undergone bullying can be mentored to recover their self-confidence and hence social participations.
Daley, T. C., Weisner, T., & Singhal, N. (2014). Adults with autism in India: A mixed-method approach to make meaning of daily routines. Social Science & Medicine, 116, 142-149.
In this book, the author focuses assessment of daily activities for grown-ups with autism in India. The data was collected from 32 participants by verbal interviewing as well as engaging them in a series of tasks outside their homes. Questioners were also given to the parents of the participant to fill. Mixed method was used to acquire the information. The basis of this study was the need to evaluate how and where adults with autism performed their daily activities. The results show that majority of the adults are let out in the public at least occasionally. Although the parents reported challenges from abnormal behaviors, it was conclusive that these individuals are not hidden. Like with other studies, this one used a small number of participants and the study time was limited.
This article has been successful in determining how parents and other family members can deal with adults diagnosed with autism without restricting them. In addition, this reading describes the importance of letting these individuals free when performing their daily activities. Parents are therefore provided with different guidelines on how they can encourage these individuals to perform their chores and interact with the outside world without supervising them all the time.
Artiste, F. M. (2014). Characteristics of Successful Classroom Behavior Therapists of Individuals with Autism: A Qualitative Case Study (Doctoral dissertation, University of Akron).
The author of this reading had an aim of bringing out the attributes that classroom therapist should have for successful caregiving for individuals with autism in a class setting. The author selected and interviewed teachers from different schools. One of the methods used by the author is behavior based interviewing of individuals to obtain meaningful information and qualitative design to analyze the information. The reading is based on the rising cases of children diagnosed with autism creating the need for special care in classrooms as well as interventions to cater for their behavioral problems. The findings of this study indicate that for quality intervention, teachers require dedication, teamwork with other teachers and mastery of other teaching methods. The major limitation of this study is that it had inadequate number of participants as well as study time. The author has also failed to describe the nature of questions asked from the participants
Despite these limitations, teachers and therapists in their preparations for teaching can apply the article to attain the different attributes that teachers need to have. For instance to handle some behaviors like screaming of the individuals can be handled through a song asking the individual to answer some questions. The article also described how the classroom therapists can attain the different attributes they need to handle their students with autism.
Basics of the synthesis
After analysis of these readings, different modes of handling individuals with autism have been put forward to assist caregivers such as parents; teachers, siblings and therapist provide effective care. Different measures have been established to care for these individuals at different ages. For instance, the first article enlightens oh how to establish the difference between a child with autism and one with attention deficit hyper reactivity disorder through errors in their handwriting. On the other hand, the second article discusses how social networks contribute to social participations for youths with autism and learning disorder. Although the topics of discussion are different the basis is the same; how to differentiate autism from similar illnesses using different parameters. The third article talks about existence of bullying for children with autism and how it can be handled. As such, the ultimate goal of the writer is to establish the challenges that children with autism face. Although all the readings cover different subjects, all are have an ultimate objective in providing efficient care for people with autism whether children, youth, or adults. The readings also educate on the effects of autism in academics, daily routines as well as social lives of the affected individuals. More so, the roles of different shareholders in caring for this individuals are outlined.
Annotated Bibliography
Caring for Autistic Individuals
Johnson, B. P., Papadopoulos, N., Fielding, J., Tonge, B., Phillips, J. G., & Rinehart, N. J. (2013). A quantitative comparison of handwriting in children with high-functioning autism and attention deficit hyperactivity disorder. Research in Autism Spectrum Disorders, 7(12), 1638-1646.
This article focused on establishing the difference in handwriting between children suffering from attention deficit hyper- reactivity disorder (ADHD) and those with high- functioning autism (HFA) to establish the effects of this disorders in academic welfare of the children. The author achieved this by having children duplicate words cat and dog repeatedly paying attention to space, size errors and speed. The study involved 49 participants all boys between ages of 7 and 14 years who had to complete the handwriting performance test (HPT). The base of this study is to illustrate how HFA and ADHD affect children in their academics limiting their expression through writing. The findings of this task indicate the existence of writing impairments in these children, and therefore there need tailored writing therapies. As it has been found in other studies, ADHD and HFA significantly affects the writing speed of the individuals. However, it has been found that other factors contribute to the lower writing speed. The study is limited in that the sample size was small.
The findings are applicable for caregivers especially teachers who care for autistic children. As such, the teachers can be able to apply different teaching methods with these children. Since the article explains the differences in factors that contribute to slow handwriting in children with ADHD and HFA, teachers are enlightened on how to how children with different disorders differently.
Kreider, C. M., Bendixen, R. M., Mann, W. C., Young, M. E., & McCarty, C. (2015). Mixed-method exploration of social network links to participation. OTJR: occupation, participation and health, 1539449215578650.
This article discusses the importance of Social Networks (SNs), and how this network affects the participation of youths especial those with Attention Deficit Hyper- Reactivity Disorder (ADHD),Learning Disorder (LD), and Autism Spectrum Disorder (ASD). The participants were interviewed individually, and the author performed personal link investigation to determine their level of participation. The method used was a combination of both qualitative and quantitative analysis blended in a mixed method design. This exercise was based on assessing the relationship between SN and participation and how these disorders affect the participation of youths. The findings of this study point out the communication impairments in individuals with these disorders. This, therefore, indicates the need to encourage the youths to participate more in social interactions to enhance their social skills. This reading has focused on the role of peers, family members and other acquaintances that comprise the SNs of these individuals in promoting their participation. The study is limited in that it lacked online participations. In addition, the sample was small, and only a few participants have complex cognitive disorders.
It is, however, beneficial to parents, friends and other family members interacting with youth with any of the disorders. Therefore, it is important for family members and friends to encourage the participation of these youths in different social activities. The study indicates that some of these individuals do not make much sense during the conversations; however, friends and relatives should not shun or discourage them. What they need is encouragement and be treated like normal persons in case of such incidents.
Heyvaert, M., Saenen, L., Campbell, J. M., Maes, B., & Onghena, P. (2014). Efficacy of behavioral interventions for reducing problem behavior in persons with autism: An updated quantitative synthesis of single-subject research. Research in developmental disabilities, 35(10), 2463-2476.
In this paper, the writer evaluates essence of behavioral interventions in eradicating the problem behavior in individuals diagnosed with autism. To come up with relevant information, the author conducted searches from journals, bibliographies, and databases. The analysis was then done to align the various sources of original studies. The method applied was a quantitative blend of mono subject studies comprising of 213 sources representing 358 individuals with autism. This study is based on the numerous problems that originate from autism and how their impacts can be reduced. The results indicate that behavioral interventions are effective in reduction of these problems; however, some are better than others are. This study has managed to cover most of the details concerning different behavioral interventions and how they can be employed to cater for problems resulting from autism. As such, it is a good piece for caregivers of individuals with challenging behaviors because of autism.
The different behavioral interventions that are described by the author of this article can be applied by parents and caregivers to handle different challenging behaviors portrayed by individuals with these disorders. This article provides crucial information for these caregivers because some of the challenging behaviors can have detrimental effects to these individuals their siblings or the caregivers. For instance self-injury behaviors can be managed through stories talks or combined therapy that has been proved efficient.
Hebron, J., Humphrey, N., & Oldfield, J. (2015). Vulnerability to bullying of children with autism spectrum conditions in mainstream education: a multi‐informant qualitative exploration. Journal of Research in Special Educational Needs, 15(3), 185-193.
This paper lays focus on how autism results in bullying of affected children in schools, and how this bullying affects them as well as how it should be handled. The author conducted interviews with five children with autism aged between 5-13 years, their parents as well as teachers. The method put into practice by the author is a cross-sectional qualitative analysis with semi-structured interviews for data gathering. The base of this study is the rampant cases of bullying of children with autism raising a lot of concern. The study concluded that bullying in schools is a serious problem for children with autism hence affecting their peer relationships. This creates the need for school staff to create a strong protective role for these children. As such, teachers should build a good relationship with these children to encourage communication and hence reduce the bullying risk. The limitation of this study is that the size of the sample is very small. However, the author has managed to cover principal areas such as the role of parents, teachers, and the entire school in the reduction of the bullying risk.
This study helps the caregivers on the signs to look out for to detect bullying and the actions to take in case of an incident. It also explains the role of teachers and parents in containing bullying. The article also describes how teachers can discourage bullying through punishment of the culprits. It also explains how children who have undergone bullying can be mentored to recover their self-confidence and hence social participations.
Daley, T. C., Weisner, T., & Singhal, N. (2014). Adults with autism in India: A mixed-method approach to make meaning of daily routines. Social Science & Medicine, 116, 142-149.
In this book, the author focuses assessment of daily activities for grown-ups with autism in India. The data was collected from 32 participants by verbal interviewing as well as engaging them in a series of tasks outside their homes. Questioners were also given to the parents of the participant to fill. Mixed method was used to acquire the information. The basis of this study was the need to evaluate how and where adults with autism performed their daily activities. The results show that majority of the adults are let out in the public at least occasionally. Although the parents reported challenges from abnormal behaviors, it was conclusive that these individuals are not hidden. Like with other studies, this one used a small number of participants and the study time was limited.
This article has been successful in determining how parents and other family members can deal with adults diagnosed with autism without restricting them. In addition, this reading describes the importance of letting these individuals free when performing their daily activities. Parents are therefore provided with different guidelines on how they can encourage these individuals to perform their chores and interact with the outside world without supervising them all the time.
Artiste, F. M. (2014). Characteristics of Successful Classroom Behavior Therapists of Individuals with Autism: A Qualitative Case Study (Doctoral dissertation, University of Akron).
The author of this reading had an aim of bringing out the attributes that classroom therapist should have for successful caregiving for individuals with autism in a class setting. The author selected and interviewed teachers from different schools. One of the methods used by the author is behavior based interviewing of individuals to obtain meaningful information and qualitative design to analyze the information. The reading is based on the rising cases of children diagnosed with autism creating the need for special care in classrooms as well as interventions to cater for their behavioral problems. The findings of this study indicate that for quality intervention, teachers require dedication, teamwork with other teachers and mastery of other teaching methods. The major limitation of this study is that it had inadequate number of participants as well as study time. The author has also failed to describe the nature of questions asked from the participants
Despite these limitations, teachers and therapists in their preparations for teaching can apply the article to attain the different attributes that teachers need to have. For instance to handle some behaviors like screaming of the individuals can be handled through a song asking the individual to answer some questions. The article also described how the classroom therapists can attain the different attributes they need to handle their students with autism.
Basics of the synthesis
After analysis of these readings, different modes of handling individuals with autism have been put forward to assist caregivers such as parents; teachers, siblings and therapist provide effective care. Different measures have been established to care for these individuals at different ages. For instance, the first article enlightens oh how to establish the difference between a child with autism and one with attention deficit hyper reactivity disorder through errors in their handwriting. On the other hand, the second article discusses how social networks contribute to social participations for youths with autism and learning disorder. Although the topics of discussion are different the basis is the same; how to differentiate autism from similar illnesses using different parameters. The third article talks about existence of bullying for children with autism and how it can be handled. As such, the ultimate goal of the writer is to establish the challenges that children with autism face. Although all the readings cover different subjects, all are have an ultimate objective in providing efficient care for people with autism whether children, youth, or adults. The readings also educate on the effects of autism in academics, daily routines as well as social lives of the affected individuals. More so, the roles of different shareholders in caring for this individuals are outlined.
We can write this or a similar paper for you! Simply fill the order form!