Turntin Score must be less than 50% or will not be accepted for credit, must be your own work and in your own words. You can resubmit, Final submission will be accepted if less than 50%. Copy paste from websites or textbooks will not be accepted or tolerated. Please see College Handbook with reference to Academic Misconduct Statement.
This sheet is to help you understand what we are looking for, and what our margin remarks might be about on your write ups of patients. Since at all of the white-ups that you hand in are uniform, this represents what MUST be included in every write-up.
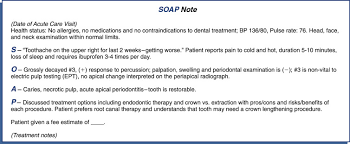
1) Identifying Data (___5pts): The opening list of the note. It contains age, sex, race, marital status, etc. The patient complaint should be given in quotes. If the patient has more than one complaint, each complaint should be listed separately (1, 2, etc.) and each addressed in the subjective and under the appropriate number.
2) Subjective Data (___30 pts.): This is the historical part of the note. It contains the following:
a) Symptom analysis/HPI(Location, quality , quantity or severity, timing, setting, factors that make it better or worse, and associate manifestations.(10pts).
b) Review of systems of associated systems, reporting all pertinent positives and negatives (10pts).
c) Any PMH, family hx, social hx, allergies, medications related to the complaint/problem (10pts). If more than one chief complaint, each should be written u in this manner.
3) Objective Data(__25 pt.): Vital signs need to be present. Height and Weight should be included where appropriate.
a) Appropriate systems are examined, listed in the note and consistent with those identified in 2b.(10pts).
b) Pertinent positives and negatives must be documented for each relevant system.
c) Any abnormalities must be fully described. Measure and record sizes of things (likes moles, scars). Avoid using ok, clear, within normal limits, positive/ negative, and normal/abnormal to describe things. (5pts).
4) Assessment (___10pts.): Diagnoses should be clearly listed and worded appropriately.
5) Plan (___15 pts.): Be sure to include any teaching, health maintenance and counseling along with the pharmacological and non-pharmacological measures. If you have more than one diagnosis, it is helpful to have this section divided into separate numbered sections.
6) Subjective/ Objective, Assessment and Management and Consistent (___10pts.): Does the note support the appropriate differential diagnosis process? Is there evidence that you know what systems and what symptoms go with which complaints? The assessment/diagnoses should be consistent with the subjective section and then the assessment and plan. The management should be consistent with the assessment/ diagnoses identified.
7) Clarity of the Write-up(___5pts.): Is it literate,
organized and complete?
We can write this or a similar paper for you! Simply fill the order form!
An allergy can be defined as an adaptive immune response directed against non-infectious environmental substances. Allergens are antigens that cause allergic responses (McCance, Huether 2014). In this case, Janet is experiencing different symptoms accompanied with different diagnosis that indicate an underlying allergy response. She has itchy eyes, nasal congestion, and watery nasal discharge. She also states that she has a tickling cough along with episodes of sneezing. Janet also gets frequent “colds” every spring and fall. Although many of these symptoms overlap when diagnosing, Janet is experiencing allergic rhinitis, acute sinusitis, and allergic conjunctivitis.
Allergic rhinitis is characterized by having symptoms of sneezing, nasal pruritus, airflow obstruction, and mostly clear nasal discharge. Not only was she experiencing these symptoms mentioned above but also presented with medium polyps on each side which is linked to allergic rhinitis (Wheatley & Togias, 2015). Upon physical examination, she also experienced tenderness over maxillary sinuses indicating acute sinusitis. Clinically, sinusitis is classified by nasal congestion, rhinorrhea, facial pain, and sneezing (Aring & Chan, 2016). Finally, she is also presenting redness on sclera and slightly swollen exhibiting allergic conjunctivitis.
Although there is a lot of information supporting allergies, there are a few questions that could be asked upon examination.
1. How long have you been experiencing these symptoms?
2. Have you ever had allergy testing?
3. Do you have any pets?
4. Have you ever had a history of asthma?
5. Are you exposed to smoke, mold, dust?
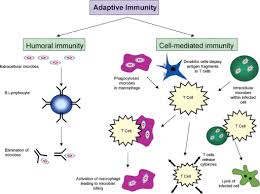
Rhinitis is the inflammation of the nasal mucosa. When a person is exposed to an allergen (pollen, molds, smoke, dust, etc.) it causes in an infiltration of mast cells, T cells, B cells, macrophages, and eosinophils within the nasal lining. The T cells release cytokines that promote the production of IgE. IgE later triggers the release of histamine and leukotrienes that cause vasodilation, increased capillary permeability, itching, runny nose, mucous secretion and smooth muscle contraction. The mediators and cytokines that have been released during this first exposure to the allergen then prompt a further cellular inflammatory response (late-phase inflammatory response) which occurs over the following 4-8 hours leading to nasal congestion and recurrent symptoms (Small & Kim, 2011).
Hypersensitivities are over-exaggerated immune responses and can be broken down into different classified reactions: allergy, autoimmunity, and alloimmunity. Hypersensitivity Type I (IgE-mediated) reactions are mediated through the binding of IgE to Fc receptors on mast cells. This causes mast cell degranulation and in turn causes the release of histamine and other inflammatory substances. Type II (tissue-specific) occurs when antibody binds to tissue-specific antigens. It is mediated by IgM or IgG targeting membrane-associated antigens. This hypersensitivity can be caused by five possible mechanisms: complement-mediated lysis; opsonization and phagocytosis; neutrophil-mediated tissues damage; antibody- dependent, cell mediated cytotoxicity; and modulation of cellular function. Type III (immune complex-mediated) reactions are caused by the formation of immune complexes that are deposited in target issues, where they activate the complement cascade, producing chemotactic fragments that attract neutrophils into the inflammatory site. Neutrophils then release lysosomal enzymes that result in tissue damage. Type IV (cell-mediated) has a cell-mediated response rather than antibodies unlike other hypersensitivity reactions. These reactions can involve either cytotoxic T lymphocytes (Tc cells) or Th1 cells (McCance, Huether 2014). All of Janet’s signs and symptoms that she presented with are indicative of type 1 hypersensitivity.
McCance, K.L, Huether, M. (2014). Pathophysiology: The biologic basis for disease in adults and children (7th Ed.). St. Louis, Missouri. Elsevier Mosby.
Small, P., & Kim, H. (2011). Allergic rhinitis. Allergy, asthma, and clinical immunology: official journal of the Canadian Society of Allergy and Clinical Immunology, 7 Suppl 1(Suppl 1), S3. doi:10.1186/1710-1492-7-S1-S3
Wheatley, L. M., & Togias, A. (2015). Clinical practice. Allergic rhinitis. The New England journal of medicine, 372(5), 456-63.
Week 2 responses 2
Based on her symptoms, Atopic dermatitis would be consistent with Janet’s flaky, erythematous rash on her arms. Up to 80% of people with atopic dermatitis have a personal or family history of asthma, allergic rhinitis, or food allergy. The cause of this dermatitis “involves an interplay of genetic predisposition, altered skin barrier function associated with filaggrin gene missense mutations (proteins that bind keratin in the epidermis), reduced ceramide (a stratum corneum lipid) levels, altered innate immunity, and altered immune responses to allergens, irritants, and microbes” (McCann & Huether, 2014, p. 1654). Memory T cells express cutaneous lymphocyte antigen, which leads to lymphocytes traveling to the skin. When mast cells are activated, eosinophils, macrophages and expression of IgE contribute to the inflammatory process (McCann & Huether, 2014, p. 1654).
Since Janet has a history of getting frequent colds, that would be another differential diagnosis I would consider. Signs and symptoms would include a runny or stuffy nose, in which she complains of watery nasal discharge. A sore throat, which could account for her pharynx being slightly erythematous, as well as cough, congestion, and sneezing, in which she complains of all. A cold could also cause slight body aches, mild headache, and a low-grade fever and malaise. Her temperature was 98.8, but she has not complained of any head or body aches.
My third and primary diagnosis is allergic rhinitis which is seasonal or perennial itching, sneezing, rhinorrhea, nasal congestion, and sometimes conjunctivitis, caused by exposure to pollens or other allergens. Diagnosis is by history and occasionally skin testing. First-line treatment is with a nasal corticosteroid (with or without an oral or a nasal antihistamine) or with an oral antihistamine plus an oral decongestant.
To further evaluate her and to make a more definitive diagnosis, there are several other questions I’d like to ask Janet. These would be:
• Do you have a family history of allergic reactions, seasonal allergies, etc.? This question would help confirm my primary diagnosis of allergic rhinitis, as research shows that if one or both parents has a history of allergies, the child could have a 40-80% chance of also being susceptible (Rote & McCance, 2014).
• Are you exposed to animals and pet dander, dusty environments, cigarette smoke, etc.? These are fairly common triggers of allergic rhinitis, so establishing if there is exposure could help determine the causes of Janet’s symptoms, as well as help her avoid them and decrease her incidence of flare-ups.
• In regard to the skin symptoms, is the rash localized to the flexor surface of the elbow, and does the rash come and go or worsen with exposure to certain environmental factors? Or is the rash on other parts of the body as well, such as the scalp, and flares up regardless of exposure? These questions will assist in differentiating eczema versus psoriasis, as eczema, or atopic dermatitis, is often brought on by exposure, whereas psoriasis is an autoimmune response.
• Have the symptoms of both the allergic rhinitis and skin rash recently started, or have these symptoms occurred throughout your lifetime?
• Is there history of immediate family having skin issues similar to your symptoms? This can also help differentiate psoriasis, as it is often genetically hereditary (McCann & Huether, 2014).
The pathophysiological process of allergic rhinitis is a Type I hypersensitivity reaction. The tissues most commonly affected by histamine effects are the ones containing large amounts of mast cells, which include the skin, the gastrointestinal tract, and the respiratory tract. The allergens cause the inflammation of the mucous membranes in the nose, sinuses, sclera, and pharynx, and also cause increased mucus production and itching. Janet is experiencing textbook symptoms of allergic rhinitis and should be started on a daily antihistamine, such as cetirizine or loraditine, among others.
There are four types of hypersensitivity reactions.
Type I – mediated by IgE and the tissue mast cells.
Type I most often occurs in response to environmental antigens
Type II – Generally when the immune response targets a certain cell or tissue. Type II occurs when antibody binds to tissue-specific antigens.
Type III – Causes by antigen-antibody complexes that are made in circulation and dropped off later in vessel walls or tissues. The antibody binds to a soluble antigen, then deposits it into a tissue, but are not organ-specific.
Type IV – This type is the only one mediated by T lymphocytes and do not involve antibody. Tissue breakdown is usually caused by either Tc cell toxins killing the cell or the release of enzymes and toxic reactive oxygen species (Rote & McCance, 2014).
Janet is experiencing a type I hypersensitivity reaction. Some type I allergic responses can be controlled by blocking histamine receptors with antihistamines, however the primary mechanism of control is the autonomic nervous system. This system includes biochemical mediators such as epinephrine and acetylcholine, which like the mediators of the inflammatory response, have profound effects on cells. They bind to appropriate receptors on mast cells and the target cells of inflammation thereby controlling the release of inflammatory mediators from mast cells and the degree to which target cells respond to inflammatory mediators (McCann & Huether, 2014, p. 272).
References
McCann, S. A., & Huether, S. E. (2014). Structure, function, and disorders of the integument. In K. L. McCance, S. E. Huether, V. L. Brashers, & N. S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (7th ed., pp. 1616-1652). St. Louis, MO: Elsevier Mosby.
Rote, N. S., & McCance, K. L. (2014). Alterations in immunity and inflammation. In K. L. McCance, S. E. Huether, V. L. Brashers, & N. S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (7th ed., pp. 262-297). St. Louis, MO: Elsevier Mosby.
We can write this or a similar paper for you! Simply fill the order form!
1. Identify an area of clinical interest 2. Find a minimum of one peer-reviewed journal article (no older than 5 years) related to your clinical topic of interest. Do not use a meta-analysis or systematic review. 3. Critique the journal article, fully answering the following questions:
Research Problems, Research Questions and Hypotheses
What is the research problem?
Does the problem build a persuasive argument for the new study?
Is the problem statement easy to locate?
What are the research questions and hypothesis?
Do the hypothesis state a predicted relationship between two or more variables?
Ethical Aspects of a Study
Was the study approved and monitored by an Institutional Review Board, Research Ethics Board or similar committee?
Were appropriate informed consent procedures used with all participants?
Research Design
Was the design experimental, quasi-experimental, or non-experimental?
Was the study longitudinal or cross-sectional?
What are the threats to the studies internal validity?
Sampling
What type of sampling design was used?
Are possible sample biases or weaknesses identified?
Data Collection
What methods of data collection were utilized (Self-reports, Scales, Observation, and Rating Scales)? If self report methods were used, did the researchers make good decisions about specific methods (in-person interviews, mailed questionnaires, etc.)?
If observational methods were used, did the report adequately describe what the observations entailed?
Statistical Analysis
Identify the type of analyses undertaken to address each research question or test each hypothesis.
Were appropriate statistical methods used, given the level of measurement of the variables, number of groups being compared, and so on?
Results/Findings
Were the findings effectively summarized, with good use of experts? Do the themes adequately capture the meaning of the data?
Does it appear that the researcher satisfactorily conceptualized the themes or patterns in the data?
Did the analysis yield an insightful, provocative, and meaningful picture of the phenomenon under investigation?
Clinical Practice
Did the researchers discuss the study’s implications for clinical practice or future research and if so, were the implications grounded in the study evidence, and in evidence from earlier research?
We can write this or a similar paper for you! Simply fill the order form!
All written assignments must be submitted via turn it in dropbox area, must be on a Microsoft Word Document, be in proper APA format: Meaning that your assignments should be typed out, font size 12 font, font names: Times New Roman, Ariel, or Calibri, normal margins (no more than 1 inch), double spaced, .5 indentation at the beginning of each paragraph and .5 hanging references. Make sure your title page consist of your name (First and Last), Panther ID number and research topic/title (APA format).
You will become the subject matter expert by conducting research based on your chosen title/topic and then reporting your findings in a potentially publishable manuscript. You do not have to seek approval for your topic. Choose any health/healthcare related topic of your choice that you feel is a significant problem within the United States.
For each written assignment make sure you address all required instructions/criteria as noted within each assignment located within the assignment instructions/grading rubric.
There’s no specific amount of pages and or word count for each assignment. Address all questions presented and if the instructions/criteria states a paragraph make sure your paragraphs consist of minimum of five complete sentences.
Assignment #2 (Literature Review)Preview the document
Example Assignments:
Found below are example assignments for this course. You are not obligated to follow exactly what’s on the example, however, you are required to complete all criteria for each assignment (see above assignment instructions/grading rubric). I am posting examples so that you get an idea of what each assignment may consist of. Please note that the examples are actually written by a former student. Therefore, you may not see all criteria requirements for each example posted and it is strongly advise that you follow the assignment instructions/ grading rubric criteria given.
The Outcomes of Neural Stem Cell Transplantation and Localized Drug Therapy on Patients
Suffering from Traumatic Brain Injury
John Doe
Panther ID: 1212121
Assignment #2
Literature Review
Within a literature review, often scientists, academic reviewers and even social experimenters review and discuss published information in a particular subject area or concentration. It usually encompasses am organizational pattern that effectively combines both summary and synthesis; by doing this, information on old material can be given a new light or a distinct and unique interpretation. Lastly, a focused literature review can also evaluate the sources and advise the reader on the most pertinent or relevant bits of information. For the sake of this literature review, I hope to express to potential readers the efficacy of neural stem cell engraftment treatment on patients who suffer from Traumatic Brain Injury (TBI) and by leaning on this form of treatment the likely outcomes it can play on society as a whole. I will provide a comprehensive knowledge based outline on the current pathway of Neural Stem Cell (NSC)
Therapy so as to then lead into these main concepts for further expansion:
Major impact of transplantation on motor and cognitive behavior.
The application of NSC engraftment increasing histopathological outcomes and the likelihood of increasing hippocampal neurogenesis in patients who suffer from Projectile Ballistics Brain Injury (PBBI).
Comparative analysis of surgical intervention versus NSC engraftment treatment outcomes on TBI based patients and how they affect physician/patient decision making.
As aforementioned above, in the next section I will elaborate on NSC treatment outcomes and how there is a significant correlation between it and the extent of transplantation affecting motor and cognitive behavior.
Overview of Literature Concept 1
According to Dr. Goldberg (2015), NSC have had tremendous positive results in rescuing both cognitive and motor based dysfunction in mice models that have sustained extensive amounts of damage in the midbrain area due to TBI. By localizing the affected region(s) of the brain that have most incurred damages, University of Michigan Clinical Scientists under Dr. Goldberg have been able to inject these impaired areas with a mix of specially designated Schwann cells that protect healthy myelinated nerve fibers, with NSC to help proliferate healthy tissue within the designated areas. On average, after 16 days of this same regimen based treatment, more than 75 percent of afflicted mice models that suffered from stroke due to TBI and PBBI based models vastly improved in both cognition and motor deficits (Goldberg et. al, 2015).
Based on Dr. Gajavelliís reports to the U.S. Department of Defense (DOD) regarding cognitive treatment for TBI veterans, to date most treatment is based on examining questions related to synucleinopathies propagation, but have overlooked the therapeutic potential of NSC transplantation to modulate cognition disorders such as dementia, PTSD and Parkinsonís disease that can all be attributed to some level of TBI (2016). At the Miami Project to Cure Paralysis Lab, work is being conducted on transgenic NSC mice that have shown consistently to improve performance in multiple levels of cognitive domains. This gradual recovery process in mice is associated with NSC expression of brain derived neurotrophic factors (BDNF), which restore depleted levels and modulates glutamatergic [modulates protein construction and synthesis] systems in the brain (Atkins, Gajavelli, Herdeen, 2016).
Post-Doctoral fellow Zachary Belrin-Lufreny at the Miami Project to Cure Paralysis, also stipulates the major implications that NSC treatment has attributed on Sprague Dawley mice 4 motor function (2016). The overall attenuation and efficacy of treatment due to NSC’s, has allowed mice who have suffered a stroke for 90 minutes to essentially be revived from the dead, and still have limited motor function. That within itself is completely unheard of in the field of Neuroscience (Belrin-Lufreny, Bramlett, Sequeira, 2016). Most mice who suffered a stroke for just a couple of minutes had prolonged and sometimes irreversible effects due to the nature of occluded blood vessels. Being at the helm of TBI research that demonstrates the probable use of future medication and treatment, data suggests that we just may be able to reverse symptoms and signs of degenerative brain loss thanks to NSC application. In the next section, I will review the components of NSC engraftment and how it responds to PBBI based injuries that may need newer and healthier neural cells so that the brain may begin to heal effectively and efficiently.
Overview of Literature Concept 2
Neurogenesis is a process in Neurology that is used to describe the growth and development of nervous tissue. It is a biological process that is almost exclusively done during the pre-natal development stage and is responsible for populating the growing brain with neurons. According to Dr. Helen Bramlett (2015), her research has shown that without a doubt in more than 3,200 laboratory controlled mice NSC injection and engraftment has led the way in increasing neurogenesis productivity at later stages in the development cycle. This is even more evident in damaged brain that needs healing and restoring capabilities that it by itself cannot perform adequately. The mouse brain, functioning just like that of the human brain, just at a much smaller rate, articulates dendrite activity just like humans do. In turn this reflects that the way they respond to injuries is very much like that of the human brain.
5
Efficacy of Dr. Bramlettís PBBI treatment procedures demonstrates extensively that when the midbrain is injured, the area where most of the neurogenesis takes place, neurons coming from the cerebral wall join up and bind at the specific injury site. When adult staged neurons enter this region, immuno-histological markers are activated in the brain and antibodies come in and do a lot more harm than good in the service of trying to protect the brain (Bramlett al, 2015). By introducing an FDA patented drug created at the University of Miami Miller School Of Medicine, researchers there have been able to inject a cocktail of the CA20 medication along with NSC’s at specific localized origin sites of injured brain regions within the hippocampus, and in more than 90 percent of mice, brain glucose metabolism decreased and provided the perfect conditions for the proliferation of NSC to grow in small proportions. But, even greater than that and more unprecedented was the facilitation of neurogenesis that CA20 and NSC combined afforded the hippocampus to do at such a steady rate (Bramlet et. al, 2015).
Dr. Bramlett and her research team have identified a tremendous factor within injury induced neurogenesis that suggests endogenous repair mechanism exists for cognitive dysfunction following traumatic brain injury (2015). When biochemical receptors of the brain lay dormant, much like that of the brain when it is injured, glucose metabolism increases drastically so as to give the brain a fighting chance at survival when it is at its lowest functional point. By lowering brain glucose metabolism which is what CA20 does, then using NSC engraftment strategies at specialized openings within traumatic brain areas is when this strategy was proven to be most effective (Bramlet et. al, 2015). The next section will evaluate where the NSC engraftment modality of treatment works most effective in. By comparing the effectiveness of treatment methodology, future healthcare professionals can outweigh the risks and benefits associated with surgical intervention or NSC engraftment for reducing TBI effects on patients.
6
Overview of Literature Concept 3
A myriad of the focus on TBI effectiveness in both the lab setting and the clinical environment has been placed on highly invasive procedures that at most times can become quite worrisome and least cost effective for families involved with patients who suffer from TBI. According to Clinical Director Dr. Ross Bullock (2016), although clinical findings in the laboratory setting validate the confidence and support for treatment in various aspects of the healthcare realm, nothing is more important and more pivotal than supplying the highest level of quality basic education/information to the families of the victims that are involved. Being a top Neurosurgeon within the country, as well as, a gifted researcher who has obtained his PhD in the field of Neuroscience, the synthesis given below will encompass a broader scope of NSC engraftment approaches and how to relay that information both sensibly and compassionately to victims and patient family members.
Based on studies conducted by Dr. Bullockís team, his data implicates that prior to any decision that the physician can make in regards to treatment procedure and viability, he must first discover the optimal location site that can produce maximal engraftment (Bullock, Dietrich, Gajavelli, 2016). If a respective localized injury site that is not compatible with tissue or cellular engraftment can’t be discovered, then unfortunately a more invasive and possibly dangerous procedure must take place in order to save the life of a patient, in this case the life of the rat is being discussed. When presented with actual human beings, this onset problem can be quite tricky to navigate; by being upfront, empathetic to a patient’s family wishes, and honest with both consequences and possible outcomes play a significant role in maintaining that family members are up to speed, as well as confidently put at ease with treatment recommendations (Bullock, Dietrich, Gajavelli, 2016).
7
If and when a NSC engraftment is possible, it is imperative that the optimal time window that produces maximal engraftment is obtained. This is discovered in mice right after onset of PBBI. Intracranial swelling is at its highest peak and glucose activity decreases around the wound drastically so neurons have not reached to injury site to protect it yet (Bramlett et. al, 2015). A radiography report and Comprehensive metabolic panel (CMP) do a remarkable job at identifying both occurrences. Once this is done at a relatively quickly, both researchers and clinicians alike must determine at what concentration of NSC is cell dose most optimal. By assessing optimal site, time, and cell concentration to produce maximal engraftment of NSC’s in a wide variety of TBI procedures, physicians can verify the best possible treatment options and in turn medical errors due to TBI procedures can be reduced when an interdisciplinary team of collaborative researchers, physicians, and family members of afflicted patients can all be in agreement of what is best for the patient (Bullock, Dietrich, Gajavelli, 2016).
References
Atkins, C., Gajavelli, S., Herdeen, B. (2016). Review of collected works for Veteran Affairs: Transplantation of Neural Stem Cells to Modulate and Aid in the Effects of Cognitive Impairments in Military Personnel. Miami Project to Cure Paralysis. Department of Veterans Affairs Medical Center, University of Miami Miller School of Medicine. Published on January 2016.
Belrin-Lufreny, Z., Bramlett, H., Sequeira, D. (2016). Hypothermic induced TBI and vehicle motility for irreversible effects: Attenuation of Motor Response in Stroke Based TBI Victims. Miami Project to Cure Paralysis. Department of Veterans Affairs Medical Center, University of Miami Miller School of Medicine. Published on January 2016.
Bramlett, H., Bullock, R., Diaz, J., Gajavelli, S., Jackson, C., Spurlock, M., et al. (2015). Penetrating Ballistic Brain Injury Systems and Methodology: A hippocampal regenerative effect study in a rat model. Miami Project to Cure Paralysis, Department of Neurosurgery, University of Miami Miller School of Medicine. Published on June 2015.
Bullock, R., Dietrich, WD., Gajavelli, S. (2016). Penetrating Ballistic Brain Injury Systems and Methodology: Optimal maximal engraftment of human NSCís via surgical intervention or localized therapy injection. Miami Project to Cure Paralysis, Department of Neurosurgery, University of Miami Miller School of Medicine. Published on February 2016.
Goldberg, N., Park, A., Sedgh, S., Silosenov, G., Zasliah,E., Zlurton, M. (2015). National institute of health: Neural Stem Cell Rescue Cognitive and Motor Dysfunction in a Transgenic Model TBI. Department of Neuro-trauma, University of Michigan School of Medicine. Published on October 2015.
Title Here
Student Name (First and Last)
Panther ID
Florida International University
Month Year
Literature Review
This section is the literature review. You will need a minimum of three concepts to elaborate on relative to your research topic. Within this section “Literature Review” you are required to include one paragraph which gives a brief overview of what a literature review is and what concepts you plan to discuss. Briefly introduce your next research section. While this may seem redundant at each section, it is important to remind the reader at the beginning of each section.
Overview of Literature Concept 1
Research your topic by reading articles, dissertations, and other scholarly materials. Elaborate on one concept that stood out to you as important for your research topic. This section requires three paragraphs in length.
Overview of Literature Concept 2
Research your topic by reading articles, dissertations, and other scholarly materials.
Elaborate on one concept that stood out to you as important for your research topic. This section
requires three paragraphs in length.
Overview of Literature Concept 3
Research your topic by reading articles, dissertations, and other scholarly materials.
Elaborate on one concept that stood out to you as important for your research topic. This section requires three paragraphs in length.
References
Remember that any reference in your reference list must be present in your paper in the form of a citation (Author, year). Likewise, any citation in your paper must be present in your reference list. Refer to your APA Handbook 6th edition for more detailed information on developing a reference list. For your Assignment 2 you need a minimum of four (4) scholarly references.
3. Research your topic and submit a two page report that includes the following information? Identify your topic and summarize three main points using documented research.? You must use at least two different sources. (NOT including the textbook)
In addition to your research, you should include how you or your family member (who does not have to be identified) has been affected and what is being done to minimize further harm or educate yourself and others about this disease or behavior.
We can write this or a similar paper for you! Simply fill the order form!
Students much review the case study and answer all questions with a scholarly response using APA and include 2 scholarly references. Answer both case studies on the same document and upload 1 document to Moodle.
Case Study 3 & 4 Seizure Disorders & Thyroiditis
Case Studies will be uploaded to Moodle and put through TURN-It-In (anti-Plagiarism program)
Turn it in Score must be less than 50% or will not be accepted for credit, must be your own work and in your own words. You can resubmit, Final submission will be accepted if less than 50%. Copy paste from websites or textbooks will not be accepted or tolerated. Please see College Handbook with reference to Academic Misconduct Statement.
Seizure Disorder Case Study
A 12-year-old boy began to complain of frequent headaches 4 months before his hospital admission. On the day of his admission, he had a major motor seizure, which his parents observed. During the seizure he lost bladder and bowel control. On physical examination he appeared to be in deep postictal sleep. He had no focal neurologic signs. On examination of the optic fundi, no evidence of papilledema was found. Studies Results Routine laboratory work Within normal limits (WNL) Skull X-ray study, p. 1062 No evidence of skull fracture Lumbar puncture, p. 651 Opening pressure 250 cm H2O (normal: <200 cm H2O) Closing pressure 220 cm H2O (normal: <200 cm H2O) Cerebrospinal fluid (CSF) examination, p. 651 Blood Negative Color Clear Cells Lymphocytes 0-2/mm3 (normal: <5/mm3 ) Polymorphonuclear leukocytes None (normal: none) Protein 120 mg/dL (normal: 15-45 mg/dL) Glucose 50 mg/dL (normal: 50-75 mg/dL) Cytology Questionably malignant cells Serologic test for venereal disease Negative (normal: negative) Electroencephalography (EEG), p. 549 Focal slowing of wave pattern in posterior aspect of the cerebrum (normal: regular, rhythmic, electrical waves) Brain scan, p. 785 Increase in radioactivity in the posterior aspect of the brain (normal: homogenous and minimal uptake of radioactive material) Cerebral angiography, p. 988 Neovascularity (tumor vessels) in the posterior aspect of the brain, involving the cerebellum and the occipital lobe of the cerebrum (normal: normal carotid vessels and terminal branches) Magnetic resonance imaging (MRI) of the brain, p. 1106 Tumor of the cerebellum extending into the posterior cerebrum Computed tomography (CT) scan of the brain, p. 1026 A soft tissue mass arising out of the cerebellum and invading the occipital lobe of the cerebrum Case Studies 2 Diagnostic Analysis The skull X-ray study ruled out the possibility of a skull fracture as the cause of the boy’s problem. Lumbar puncture excluded the possibility of meningitis or subarachnoid hemorrhage; however, the high protein count and questionable positive cytology indicated a possible neoplasm. An EEG located an area of nonspecific abnormality in the posterior aspect of the brain. Brain scanning, cerebral angiography, and CT scanning indicated a posterior fossa tumor. These tests are mentioned in this case study mostly for historical interest. Under most circumstances, this young boy would have a MRI of the brain early in the diagnostic period. Because of these findings, the patient underwent a craniotomy. In many centers, this young boy would have a nonoperative stereotactic brain biopsy instead of a craniotomy. An invasive medulloblastoma was found to be arising from the patient’s cerebellum and involving the occipital lobe of the cerebrum. The tumor was unresectable. Postoperatively, the patient was given phenytoin (Dilantin) and radiation therapy to the involved area. A chemotherapy regimen was administered. The patient’s tumor did not respond to the therapy, and he died 4 months after the onset of disease. Critical Thinking Questions 1. What are the major assessments that the nurse should make during seizure activity? 2. Why is the EEG a priority study for patients with seizure disorders?
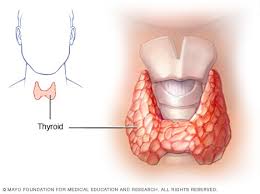
Thyroiditis Case Study
The patient, a 23-year-old woman, has had a bout of flulike symptoms over the past few weeks. Most recently, she has become increasingly tired. She is taking birth control pills to control her menses. Her anterior neck became painful during the past few weeks. The physical examination results reveal that her thyroid is diffusely enlarged and mildly tender. Studies Results Routine laboratory tests Within normal limits (WNL) Total thyroxine (T4), p. 497 8 mcg/dL (normal: 5-12 mcg /dL) Free T4 0.5 ng/dL (normal: 0.8-2.7 ng/dL) Free T4 index 0.4 ng/dL (normal: 0.8-2.4 ng/dL) Triiodothyronine (T3), p. 506 52 ng/dL (normal: 70-205 ng/dL) Thyroxine-binding globulin (TBG), p. 495 12 mg/dL (normal: 1.7-3.6 mg/dL) Thyroid stimulating hormone (TSH), p. 486 32 microunits/mL (normal: 2-10 microunits/mL) Thyroid scanning, p. 839 Enlarged gland; normal shape, position, and function of the thyroid gland. No areas of decreased or increased uptake Thyroid ultrasound, p. 895 Enlarged gland; normal shape and position of the thyroid gland Thyroid antibodies Antithyroglobulin antibody, p. 102 1:250 (normal: titer <1:100) Antithyroid peroxidase antibody, p. 104 1:500 (normal: titer <1:100) Thyroid-stimulating immunoglobulins, p. 491 Negative Diagnostic Analysis Total T4 measures protein-bound and unbound T4. Because the patient was taking birth control pills, her TBG was elevated; therefore, her total T4 was normal. Free T4 and FT4 index tests measure unbound T4. When the free T4 and the FT4 index were measured, they were found to be low, indicating that the patient had hypothyroidism. The TSH level was elevated because of primary failure of the thyroid. The thyroid antibodies were elevated, indicating that the patient had Hashimoto thyroiditis. Her long-acting thyroid stimulator (LATS) levels were normal, discounting Graves disease as a cause of her diffusely enlarged thyroid. Her thyroid ultrasound and scan failed to show any localized, defined tumor. The patient was started on thyroid replacement therapy, and her TSH level returned to normal. Over the next few weeks, she felt markedly better. Her thyroid pain and tiredness disappeared. Critical Thinking Questions 1. Why were the thyroid antibodies important in this patient’s diagnosis? 2. What symptoms might she experience if too much thyroid replacement medication were administered?
We can write this or a similar paper for you! Simply fill the order form!
Injuries from Blunt Force Trauma Vs Sharp Force Injuries Review the following scenario:
A 911 call came in at 3 a.m. from a local nightclub. It was reported that an individual was injured and unconscious. Upon EMS arrival, the victim was dead. You are called to the scene to investigate. This is your first death scene. You are having difficulty identifying the wounds on the body. Answer the following questions:
Morphine effects, adverse effects, and contraindications
Morphine effects, adverse effects, and contraindications
Always review the assigned readings for the week before developing your discussion. Always include references in at the end of your discussion. Do not copy and post as it is in your text book, paraphrase in your own words to indicate that you understood what you read.
Write a discussion to explain;
1. Sumatriptan including its side effects, adverse effects, and contraindications
2. Morphine including its side effects, adverse effects, and contraindications
3. Quetiapine including its side effects, adverse effects, and contraindications
Resources
Richard A. Lehne (2013). Pharmacology for Nursing care (8th ed.). ISBN: 978143773586
Chapter 28-Opioid analgesics & antagonists
Control of Communicable and Noncommunicable Disease
Control of Communicable and Noncommunicable Disease
1st discussion: From Public Health 101, page 149: “Your hometown of 100,000 is faced with a crisis as an airplane lands containing a passenger thought to have a new form of severe influenza that has recently gained the ability to spread from person to person through airborne transmission. As the mayor of the city, what do you decide to do?” Why? Be sure to justify your decision. Be sure to address the following:
What other healthcare disciplines would you include on your team? Why?
What information is important to collect and from whom? Why?
N.B.
need 2 pages and 3 reference sources
2nd discussion: The Healthcare Workforce
In this discussion, examine the current increase in longevity within the Kingdom of Saudi Arabia. What impact will this aging of the nation have on the current and future healthcare system? What plans does the Kingdom have in place to meet these demands now and for the long-term?
N.B.
need 2 pages and 3 reference sources
We can write this or a similar paper for you! Simply fill the order form!
Interstellar Voyage To The Serpent Nebula Write a 3-5 page (approximately 900-1500 word) paper responding to ONE of the following prompts.
Interstellar Voyage To The Serpent Nebula
Your paper should be typed, double-spaced, 12 pt. font, with one-inch margins. Make sure to include your name, class name and section, and date.
Your paper is due on FRIDAY, MARCH 1st Each day that your paper is late you will lose 2/3 of a grade off of whatever grade you receive.
Either EMAIL me a copy or turn it in on the blackboard.
MAKE SURE THAT YOUR OWN LAST/SURNAME/FAMILY NAME IS IN THE NAME OF YOUR FILE!!! I WILL NOT BE ACCEPTING PAPERS WITH TITLES LIKE “PAPER 1”!!!
TOPIC #1
It’s the year 2180. You have been given the honor of being a member on an interstellar voyage to the Serpent Nebula. Upon arrival in the nebula, you discover the planet Tuchanka, which is a harsh planet with few resources. Indeed, it seems like most of the wildlife on Tuchanka evolved to be incredibly deadly. The dominant humanoids you find on this world are the Krogan, a hyper-aggressive species of bipedal reptiles. The main social institution in Krogan society is the clan, and clans are more or less in constant warfare with one another. They raid each other on a regular basis both to steal supplies and take prisoners but also to assert their dominance over their neighbors. These raids are violent and often erupt in full-fledged war. Nuclear warfare is not uncommon and neither is the death and environmental destruction that accompanies it. Nearly all Krogan activities are characterized by violence. Everyday arguments are settled with violent head butts and fistfights to the death and recreational activities largely consist of space-dog fighting and the hunting of large and highly dangerous game. Even peace negotiations between clans have been known to turn violent at the drop of a hat. In short, violence and killing appear to be key features of Krogan society.
How should we feel about the Krogan? That is, are Krogan practices morally objectionable? Or does the fact that Krogan society is so different from our own make it the case that we are in no position to judge them?
In this essay I want you to answer these questions. That is, I want you to give a reasoned argument for whether we are in a position to judge the Krogan and why you hold that position. In your paper, you should begin by saying what this situation is and what you think should be said about it. Next, construct reasons for thinking that the Krogan are or are not a morally objectionable group. You should say why one might think the Krogan are morally wrong and then either show why this view is correct or why it is incorrect. When doing this you will probably want to draw on Rachels’ article on Cultural relativism and/or Tavani’s discussions of Cultural Relativism (or any of the other readings that you might find useful). You will also want to make sure to say what Cultural Relativism actually is. Make sure to say how the considerations you bring up are relevant to the case of the Krogan. Things you might want to touch on include the consequences of Krogan actions, what we know of their environments and their cultures, what we don’t know of their environment and cultures, how Krogan culture compares with human culture, what the Krogan suggest about morality more generally (don’t try to address all these things, just the ones you think are most relevant). After you lay out your argument you might want to consider how someone might respond to (but you don’t have to). Conclude with a short summary of your argument.
TOPIC #2
One day you’re walking down the street with your best friend, Chewbacca. As you walk there is suddenly a bright flash of light and a bang so loud that you get knocked to the ground. When you stand up and gather your wits, there standing in front of you is the devil.
The devil tells you he is bored and in need of some entertainment. Since he is the devil, this means that someone has to die. The devil makes you an offer. The offer is this: if you want you, can take the gun that the devil is holding out to you and shoot Chewbacca. If you do this, the devil will dispose of the body and make sure that no one ever knows that you killed Chewbacca. He will then go on his way and you will never see him again. If you do not shoot Chewbacca, however, the devil will randomly pick a town somewhere in the United States with about 10,000 residents, and make them all die excruciating deaths within the next hour. He then says you and Chewbacca have five minutes to confer and decide what to do.
Chewbacca turns to you and says, “I am convinced that Act Utilitarianism is correct. Therefore I think you should kill me and here is why.” Chewbacca then proceeds to present his argument for thinking that you should take the gun the Devil is offering and kill him.
In this paper, provide an account of the sort of argument Chewbacca is likely to make and then assess his argument.
To do this your paper should have something like the following structure. Begin by laying out this out this bizarre scenario and provide an account for how the paper will proceed. Then, lay out the sort of argument that Chewbacca the Act Utilitarian is likely to use to convince you to shoot him. In this section make sure you say what Act Utilitarianism actually is, what they conclude about how you should act, and why being an Act Utilitarian would lead Chewbacca to conclude that you should shoot him. Next, assess whether Chewbacca’s argument is a good one and whether or not it has convinced you to shoot him. In this section, you are probably going to want to say what some of the main problems are that people bring up for Act Utilitarianism are and whether you think these arguments actually undermine Chewbacca’s argument. (That is, you might say that one thing that Chewbacca is forgetting about is ______ and that this undermines his argument because of ______. If you do this you might then want to consider how Chewbacca might respond. Alternatively, you could say that one thing that someone else might try to say in response to Chewbacca is _____ but that this isn’t really a problem for his argument because of _______. Make sure to tell me whether, in the end, you accept Chewbacca’s reasons for telling you to shoot him.) Finish your paper with a short conclusion summing things up
Topic #3
One day you’re walking down the street with two classmates, who are named Luke and Leia. As you walk there is suddenly a bright flash of light and a bang so loud that you get knocked to the ground. When you stand up and gather your wits, there standing in front of you is the devil.
The devil tells you he is bored and in need of some entertainment. Since he is the devil, this means that someone has to die. The devil makes Luke an offer. The offer is this: if Luke wants, he can take the gun that the devil is holding out to him and shoot Leia. If he does this, the devil will dispose of your body and make sure that no one ever knows that Luke has killed Leia. The devil will then go on his merry way and you will never see him again. If Luke does not shoot Leia, however, the devil is going to randomly pick a town somewhere in the United States with about 10,000 residents, and make them all catch plague and die excruciating deaths within the next hour. He then says you, Luke, and Leia has five minutes to confer and decide what to do.
So Luke turns to you and Leia says, “I am convinced that Deontology of the sort described by Kant is correct. Therefore I fully believe that killing Leia would be the wrong thing to do and here is why.” Luke then proceeds to present his argument for thinking that killing Leia would be wrong.
In this paper, provide an account of the sort of argument that Luke is likely to make and then assess his argument.
Your paper should have something like the following structure. Begin by laying out this out this bizarre scenario and provide an account for how the paper will proceed. Then, lay out the sort of argument that Luke the Deontologist is likely to use to convince you that he shouldn’t shoot Leia. In this section make sure you say what Deontology actually is, what deontologists conclude about how people should act, and why being a Deontologist would lead Luke to think that he shouldn’t shoot Leia. Next, assess whether Luke’s argument is a good one and whether or not it has convinced you that Luke really shouldn’t shoot Leia. In this section, you are probably going to want to say what some of the main problems are that people bring up for Deontology these arguments actually undermine Luke’s argument. (That is, you might say that one thing that Luke is forgetting about is ______ and that this undermines his argument because of ______. If you do this you might then want to consider how Luke might respond. Alternatively, you could say that one thing that someone else might try to say in response to Luke is _____ but that this isn’t really a problem for her argument because of _______. If you do this you might then want to consider how this other person might then respond in turn). Make sure to tell me whether, in the end, you accept Luke’s reasons to not shoot Leia. Finish your paper a short conclusion summing things up.